Original Article Urogenit Tract Infect 2015;10(2):120-125
Characteristics of Patients Who Visited the Emergency Room after Prostate Biopsy: Single Center Retrospective Study
Seung Chan Jeong, Seungsoo Lee, Jae Min Chung, Sang Don Lee
Department of Urology, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea
Purpose: To educate patients and prevent biopsy-related complications, it is helpful to understand the causes for visiting the emergency room (ER).
Therefore, we want to analyze the causes and factors of complications that cause patients to visit the ER after prostate biopsy.
Materials and Methods: We conducted a study of in-patients who visited the ER of Pusan National University Yangsan Hospital after prostate biopsy from De- cember 2008 to July 2015. Age, postoperative interval before visiting the ER, Charlson comorbidity index (CCI) score, symptoms in ER, prostate size, pathologic result, and number of biopsy cores were analyzed retrospectively.
Results: Among all 1,694 cases of patients who had undergone prostate biopsies during a 7-year period, only 37 patients (2.2%) visited the ER. Diabetes mellitus (DM) is the most common underlying disease among patients with accompanying infection-related symptoms compared to patients with accompanying non-infec- tion-related symptoms (p<0.001). In univariate analysis, DM (p=0.004) and CCI score (p=0.030) were statistically significant risk factors for infection, but only DM was significant in multivariate analysis (p=0.004). Prostate size (p=0.044) was a significant risk factor for acute urinary retention (AUR) in univariate analysis, but not statistically significant in multivariate analysis. CCI score was a statistically significant risk factor for bleeding (p=0.005 [univariate], 0.035 [multivariate]).
Conclusions: AUR after transrectal ultrasound-biopsy is the most common reason for visiting the ER. CCI score showed correlation with bleeding and DM showed correlation with infection. Consideration of risk factors of complications after prostate biopsy will be helpful to the patients in the treatment and prevention of complication.
Keywords: Infection; Diabetes mellitus; Comorbidity; Biopsy; Prostate
Copyright 2015, Korean Association of Urogenital Tract Infection and Inflammation. All rights reserved.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 September, 2015 Revised: 17 October, 2015 Accepted: 19 October, 2015
Correspondence to: Sang Don Lee http://orcid.org/0000-0001-9459-3887 Department of Urology, Pusan National University Yangsan Hospital, 20 Geumo-ro, Mulgeum-eup, Yang- san 50612, Korea
Tel: +82-55-360-2134, Fax: +82-55-360-2164 E-mail: [email protected]
INTRODUCTION
Prostate cancer (PCA) is the most frequently diagnosed cancer among males in western countries. In South Korea, incidence of PCA has shown a continuous increase, because of the rapid increase of the aged population and wester-
nization of diet. Transrectal ultrasound (TRUS)-guided pro- state biopsy is the standard procedure commonly performed for patients with elevated prostate-specific antigen (PSA≥4 ng/ml) or abnormal digital rectal examination. The benefits and risks of prostate biopsy for PCA screening and treatment are under debate. Although minor complications such as
voiding difficulty, dysuria and bleeding are frequent, major complications are not common after prostate biopsy [1].
In the majority of cases, prostate biopsy was performed in the outpatient setting. Patients who developed a com- plication visited the emergency room (ER). The objective of this study was to analyze the causes and factors of complications that cause patients to visit the ER after TRUS-guided prostate biopsy.
MATERIALS AND METHODS
Our study was conducted on 37 patients who visited the ER after prostate biopsy among all patients who under- went TRUS-guided prostate biopsy from December 2008 to July 2015 at Pusan National University Yangsan Hospital (Yangsan, Korea).
We compared and studied three complications: infection- related symptoms, acute urinary retention (AUR), and bleed- ing such as hematuria or rectal bleeding. In our study, the Charlson comorbidity index (CCI) was used as an indicator of comorbidity. CCI was stratified according to four catego- ries: 1: CCI=0 (control), 2: CCI=1, 3: CCI=2, 4: CCI≥3 [2].
The risk factors following TRUS-guided prostate biopsy included age, PSA, prostate size, PCA, diabetes mellitus (DM), and CCI score.
We respectively analyzed and compared age, interval to revisit ER after prostate biopsy, CCI score, symptoms in ER, prostate size, the relevance of the PCA and the number of biopsy cores, using PASW ver. 18 software (IBM Co., Armonk, NY, USA). Relative risk was calculated using chi-square and logistic regression tests.
This study was approved by the Institutional Review Board of Pusan National University Yangsan Hospital (IRB 05-2015-011).
RESULTS
During our 7-year single institutional study, 1,694 TRUS- guided prostate biopsies were performed. Among the cases, 37 patients (2.2%) visited the ER within 2 weeks postopera- tively. The mean age of patients who visited the ER after prostate biopsy was 66.8±1.3 years, mean prostate size was 50.0±2.7 ml, and mean PSA was 17.7±4.6 ng/ml.
The mean CCI score was 3.8±0.2 points.
Among patients who visited the ER after prostate biopsy,
17 patients (45.9%) were diagnosed with PCA. After prostate biopsy, mean interval to visit the ER was 3.4±0.6 days.
TRUS-guided prostate biopsy was performed in the out- patient setting, except one patient in whom it was performed during hospitalization.
Eight patients complained of hematuria, one of whom also complained of rectal bleeding. Three patients among eight patients were hospitalized because of severe bleeding and anxiety. The one patient with accompanying rectal bleeding required indwelling of a Foley catheter, and squee- zing the area with gauze, the patient was hospitalized in the gastroenterology division. Thirteen patients complained of AUR, three of whom were hospitalized after receiving an indwelling Foley catheter, and 10 patients were dis- charged to the ER after receiving an indwelling Foley catheter or using a Nelaton catheter.
Six patients complained of fever and myalgia, three of whom complained of neurological abnormality such as syncope at the same time were diagnosed with stroke and hospitalized in the department of neurology; among these, one patient who complained of chest pain showed no abnormal findings. Three patients were hospitalized in the Department of Urology.
Six patients complained of nausea and dizziness, but there were no abnormal findings in evaluation. After hyd- ration and taking absolute rest, the symptoms were relieved, so that all six patients were discharged.
Four patients who complained of dysuria were discharged after pain control.
None of the patients underwent transfusion, and the patient with accompanying rectal bleeding did not undergo endoscopic management; after squeezing, the symptoms were relieved.
After primary treatment, 25 patients (67.6%) were dis- charged and 12 patients (32.4%) were admitted to hospital.
The symptoms of admitted patients were fever (6), AUR (3), hematuria (2), and rectal bleeding with hematuria (1), among whom one patient died despite administration of broad-spectrum antibiotics.
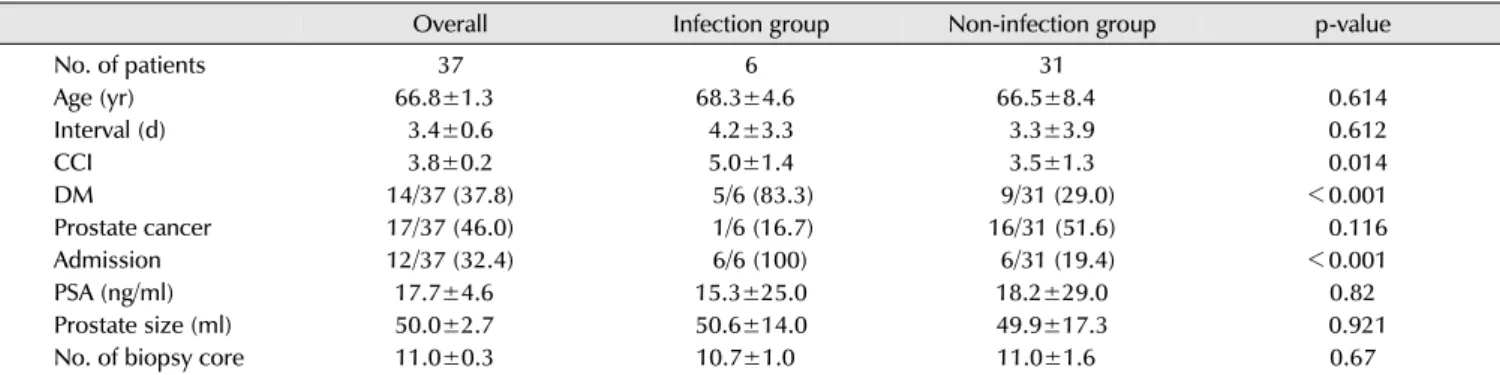
DM is the most frequent underlying disease among patients with accompanying infection-related symptoms compared to the patients with accompanying non-infection- related symptoms (p<0.001) (Table 1).
DM (p=0.004) and CCI (p=0.030) were statistically signi- ficant risk factors for infection in univariate analysis;
Table 2. Risk factors for infection after transrectal ultrasound-guided prostate biopsy
Risk factor Infection-related symptoms (n=6, 16.2%)
Univariate RR 95% CI p-value Multivariate RR 95% CI p-value
Age 0.970 0.864-1.088 0.604 1.36 0.765-2.419 0.295
CCI 0.405 0.179-0.916 0.030 0.2 0.015-2.706 0.226
Prostate cancer 0.188 0.020-1.796 0.147 1.278 0.009-1.907 0.923
DM 3.375 3.093-3.865 0.004 3.375 3.092-3.682 0.004
PSA 1.004 0.970-1.040 0.814 0.992 0.906-1.087 0.870
Biopsy number 1.127 0.665-1.910 0.658 1.854 0.369-9.308 0.453
Prostate size 0.997 0.946-1.051 0.918 1.027 0.895-1.177 0.707
RR: relative risk, CI: confidence interval, CCI: Charlson comorbidity index, DM: diabetes mellitus, PSA: prostate-specific antigen.
Table 1. Overall characteristics of patients who visited the emergency room after prostate biopsy
Overall Infection group Non-infection group p-value
No. of patients 37 6 31
Age (yr) 66.8±1.3 68.3±4.6 66.5±8.4 0.614
Interval (d) 3.4±0.6 4.2±3.3 3.3±3.9 0.612
CCI 3.8±0.2 5.0±1.4 3.5±1.3 0.014
DM 14/37 (37.8) 5/6 (83.3) 9/31 (29.0) <0.001
Prostate cancer 17/37 (46.0) 1/6 (16.7) 16/31 (51.6) 0.116
Admission 12/37 (32.4) 6/6 (100) 6/31 (19.4) <0.001
PSA (ng/ml) 17.7±4.6 15.3±25.0 18.2±29.0 0.82
Prostate size (ml) 50.0±2.7 50.6±14.0 49.9±17.3 0.921
No. of biopsy core 11.0±0.3 10.7±1.0 11.0±1.6 0.67
Values are presented as number, mean±standard deviation, or number/total number (%).
Infection group: infection-related symptoms group, Non-infection group: non-infection-related symptoms group, Interval: interval to revisit emergency room after biopsy, CCI: Charlson comorbidity index, DM: diabetes mellitus, Prostate cancer: prostate cancer diagnosed following prostate biopsy, PSA: prostate-specific antigen.
Table 3. Risk factors for acute urinary retention after transrectal ultrasound-guided prostate biopsy
Risk factor Acute urinary retention (n=13, 35.1%)
Univariate RR 95% CI p-value Multivariate RR 95% CI p-value
Age 0.950 0.867-1.041 0.075 0.098 0.811-1.018 0.097
CCI 1.055 0.642-1.734 0.083 5.340 0.771-3.697 0.090
Prostate cancer 2.667 0.664-10.704 0.167 6.292 0.519-7.625 0.149
DM 0.001 0.001-0.002 0.999 0.001 0.001-0.003 0.900
PSA 0.988 0.964-1.013 0.352 1.056 1.056-0.993 0.085
Biopsy number 1.531 0.922-2.544 0.100 2.559 0.973-6.727 0.057
Prostate size 0.914 0.914-0.999 0.044 0.905 0.811-1.010 0.075
RR: relative risk, CI: confidence interval, CCI: Charlson comorbidity index, DM: diabetes mellitus, PSA: prostate-specific antigen.
however, in multivariate analysis only DM was a significant risk factor for infection (p=0.004) (Table 2).
Prostate size (p=0.044) was a significant risk factor for AUR in univariate analysis but not in multivariate analysis (Table 3).
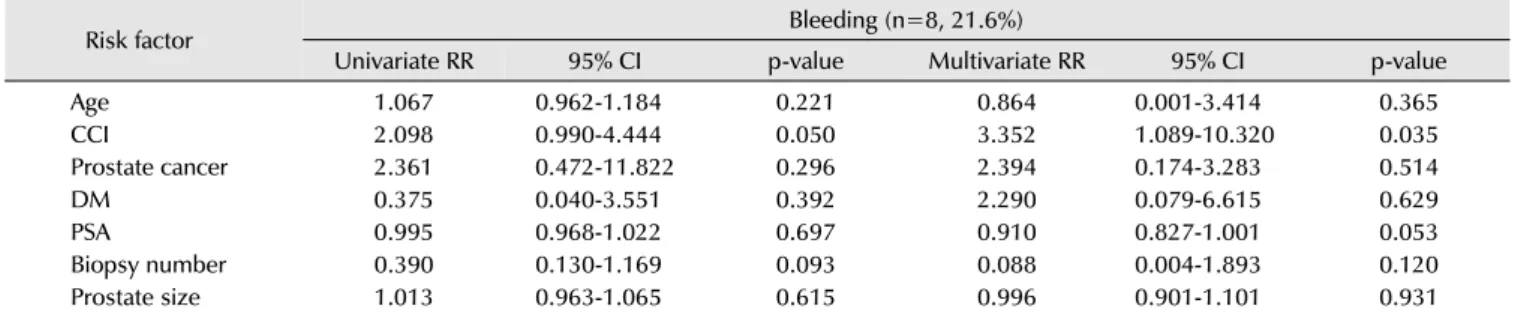
CCI score was a statistically significant risk factor for bleeding (p=0.005, 0.035) (Table 4).
DISCUSSION
TRUS-guided prostate biopsy is a standard procedure commonly performed for patients with elevated PSA ≥4 ng/ml or abnormal digital rectal examination. As the inci- dence and prevalence of PCA increase, concern over pros- tate biopsy-related complications is rising. One patient among six patients who complained of fever and myalgia died, despite administration of broad-spectrum antibiotics. In our single institutional 7-year study, sepsis-related mortality after
Table 4. Risk factors for bleeding after transrectal ultrasound-guided prostate biopsy
Risk factor Bleeding (n=8, 21.6%)
Univariate RR 95% CI p-value Multivariate RR 95% CI p-value
Age 1.067 0.962-1.184 0.221 0.864 0.001-3.414 0.365
CCI 2.098 0.990-4.444 0.050 3.352 1.089-10.320 0.035
Prostate cancer 2.361 0.472-11.822 0.296 2.394 0.174-3.283 0.514
DM 0.375 0.040-3.551 0.392 2.290 0.079-6.615 0.629
PSA 0.995 0.968-1.022 0.697 0.910 0.827-1.001 0.053
Biopsy number 0.390 0.130-1.169 0.093 0.088 0.004-1.893 0.120
Prostate size 1.013 0.963-1.065 0.615 0.996 0.901-1.101 0.931
RR: relative risk, CI: confidence interval, CCI: Charlson comorbidity index, DM: diabetes mellitus, PSA: prostate-specific antigen.
prostate biopsy was 0.06%. This result is lower than the three-country (Finland, Netherlands, and Sweden) European Randomized Study of Screening for Prostate Cancer (ERSPC) trial rate of 0.24% [3]. It is also lower than the 0.13%
sepsis-related mortality reported by Wei et al. [4].
Previous studies have reported an extremely minimal sepsis-related mortality rate following TRUS biopsy. PCA can be detected in the early stage by TRUS-prostate biopsy, thus it may reduce mortality of individuals diagnosed with PCA. Among 1,694 TRUS-guided prostate biopsies, 37 patients (2.2%) who visited the ER within two weeks were the subject of our study. In our study, 17 patients (45.9%) were diagnosed with PCA, much higher than the 32.3%
in the PLCO trial [5], the 17.1% in the Surveillance Epi- demiology and End Result study (SEER) [6], and the 36%
reported by Wei et al. [4]. This may be due to the limited scope of the current study.
Infection is a well-established risk of TRUS-biopsy [7].
We studied two major complication types following TRUS prostate biopsy: infection-related symptoms and non-infec- tion symptoms.
The rates of these complications were 16.2% and 83.8%, respectively.
Findings of our study using the entire prostate biopsy cohort showed fever or myalgia (0.35%), AUR (0.77%), and bleeding (0.47%). This was lower than the 6.59%, 9.76%
and 1.14% by Wei et al. [4], who reported that AUR was most common among postoperative complications. Loeb et al. [6] reported bleeding as the most common symptom after prostate biopsy. However, in our study, AUR was the most common. These symptoms were minor and resolved spontaneously except for those of three patients hospitalized after receiving an indwelling Foley catheter.
Ten patients were discharged to the ER after receiving an
indwelling Foley catheter or using a Nelaton catheter. On the other hand, infection-related symptom (0.35%, 16.2%) was the least common cause of the ER visit, but the most common symptom among patients in hospitalization. The infection complication rate in the Rotterdam section of the ERSPC was 4.2% [8], higher than our study. Among the 72,500 biopsies performed in the United Kingdom, 2.15-3.6% patients were readmitted because of infection- related complications [9]. In the Global Prevalence Study of Infections in Urology, 3.5% of patients complained of febrile UTI, and 3.1% required hospitalization after prostate biopsy [10].
Simsir et al. [11] reported a similar frequency of 3.06%.
However, other studies from North America [12,13] reported lower rates of sepsis (0.6%), and an Asian study [14] reported that 0.5% of prostate biopsy cases had fever, similar to the data of our study.
An Asian study reported no septic complications [15].
Infection-related complications after prostate biopsy have been an increasing issue, and numerous strategies have been evaluated to reduce the risk of complications. Assess- ment of risk factors for infection and antibiotics resistance, thorough history, and physical examination was recommen- ded [16]. Earlier studies reported that risk factors of infection- related complications were DM [8,11,17-19], comorbidities [6], more biopsy cores [11,20-22], and repeat biopsy [11,16, 23]. Significant risk factors for fever after TRUS biopsy included prostate size and DM in the Rotterdam section of the ERSPC trial [8]. In the SEER study, Loeb et al. [6]
reported that significant risk factors included nonwhite ethnicity and higher comorbidity scores.
In our study, DM (p=0.004), and CCI (p=0.030) were statistically significant risk factors for infection in univariate analysis; however, in multivariate analysis, only DM was
a significant risk factor for infection (p=0.004).
Earlier studies reported that the complication rate of AUR after prostate biopsy ranges from 0.2% to 1.7% [12,24-30].
Raaijmakers et al. [31] reported that risk factors of urinary retention after prostate biopsy included prostate size, ratio of transition zone size to total size, and an IPSS. Zaytoun et al. [26] and Chiang et al. [32] reported that prostate size predicted AUR after prostate biopsy. On the other hand, in our study, prostate size (p=0.044) was a significant risk factor for AUR in univariate analysis but not in multivariate analysis (p=0.075).
Gross hematuria after TRUS-biopsy is common, and the reported rate of complication was 10-84% [2,8,16] because of different definitions for hematuria. Another study re- ported that hematuria lasting >3 days was seen in 22.6%
and had relevance to prostate size (r=0.096; p<0.001) and transition zone volumes (r=-0.076; p<0.001) [31]. Others have also reported increased hematuria with larger prostate volume [26].
In our study, CCI score was a statistically significant risk factor for bleeding (p=0.005 [univariated], 0.035 [multiva- riated]). We know that there was a problem comparing our study to earlier studies, due to difference in scope.
In our study, the possibility that patients with complication after prostate biopsy visited other hospitals with ER or visited outpatient clinics was overlooked.
CONCLUSIONS
We concluded that AUR after TRUS-biopsy is the most common complication. CCI score showed correlation with bleeding and DM showed correlation with infection.
Referring to risk factors of complications after prostate biopsy will be helpful to the patients in the treatment and prevention of complications.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
ACKNOWLEDGMENTS
This work was supported by two years by Pusan National University Research Grant.
REFERENCES
1. Rosario DJ, Lane JA, Metcalfe C, Donovan JL, Doble A, Goodwin L, et al. Short term outcomes of prostate biopsy in men tested for cancer by prostate specific antigen: prospective evaluation within ProtecT study. BMJ 2012;344:d7894.
2. Quan H, Sundararajan V, Halfon P, Fong A, Burnand B, Luthi JC, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care 2005;43:1130-9.
3. Carlsson SV, Holmberg E, Moss SM, Roobol MJ, Schröder FH, Tammela TL, et al. No excess mortality after prostate biopsy:
results from the European Randomized Study of Screening for Prostate Cancer. BJU Int 2011;107:1912-7.
4. Wei TC, Lin TP, Chang YH, Chen TJ, Lin AT, Chen KK. Transrectal ultrasound-guided prostate biopsy in Taiwan: a nationwide database study. J Chin Med Assoc 2015;78:662-5.
5. Pinsky PF, Parnes HL, Andriole G. Mortality and complications after prostate biopsy in the Prostate, Lung, Colorectal and Ovarian Cancer Screening (PLCO) trial. BJU Int 2014;113:
254-9.
6. Loeb S, Carter HB, Berndt SI, Ricker W, Schaeffer EM. Com- plications after prostate biopsy: data from SEER-Medicare. J Urol 2011;186:1830-4.
7. Puig J, Darnell A, Bermúdez P, Malet A, Serrate G, Baré M, et al.
Transrectal ultrasound-guided prostate biopsy: is antibiotic prophylaxis necessary? Eur Radiol 2006;16:939-43.
8. Loeb S, van den Heuvel S, Zhu X, Bangma CH, Schröder FH, Roobol MJ. Infectious complications and hospital admissions after prostate biopsy in a European randomized trial. Eur Urol 2012;61:1110-4.
9. Batura D, Gopal Rao G. The national burden of infections after prostate biopsy in England and Wales: a wake-up call for better prevention. J Antimicrob Chemother 2013;68:247-9.
10. Wagenlehner FM, van Oostrum E, Tenke P, Tandogdu Z, Çek M, Grabe M, et al; GPIU investigators. Infective complications after prostate biopsy: outcome of the Global Prevalence Study of Infections in Urology (GPIU) 2010 and 2011, a prospective multinational multicentre prostate biopsy study. Eur Urol 2013;63:521-7.
11. Simsir A, Kismali E, Mammadov R, Gunaydin G, Cal C. Is it possible to predict sepsis, the most serious complication in prostate biopsy? Urol Int 2010;84:395-9.
12. de Jesus CM, Corrêa LA, Padovani CR. Complications and risk factors in transrectal ultrasound-guided prostate biopsies. Sao Paulo Med J 2006;124:198-202.
13. Zaytoun OM, Vargo EH, Rajan R, Berglund R, Gordon S, Jones JS. Emergence of fluoroquinolone-resistant Escherichia coli as cause of postprostate biopsy infection: implications for pro- phylaxis and treatment. Urology 2011;77:1035-41.
14. Shigemura K, Matsumoto M, Tanaka K, Yamashita M, Arakawa S, Fujisawa M. Efficacy of combination use of Beta-lactamase inhibitor with penicillin and fluoroquinolones for antibiotic
prophylaxis in transrectal prostate biopsy. Korean J Urol 2011;
52:289-92.
15. Raheem OA, Casey RG, Galvin DJ, Manecksha RP, Varadaraj H, McDermott T, et al. Discontinuation of anticoagulant or anti- platelet therapy for transrectal ultrasound-guided prostate bio- psies: a single-center experience. Korean J Urol 2012;53:234-9.
16. Nam RK, Saskin R, Lee Y, Liu Y, Law C, Klotz LH, et al. Increasing hospital admission rates for urological complications after transrectal ultrasound guided prostate biopsy. J Urol 2013;
189(1 Suppl):S12-7; discussion S17-8.
17. Carignan A, Roussy JF, Lapointe V, Valiquette L, Sabbagh R, Pépin J. Increasing risk of infectious complications after trans- rectal ultrasound-guided prostate biopsies: time to reassess antimicrobial prophylaxis? Eur Urol 2012;62:453-9.
18. Tal R, Livne PM, Lask DM, Baniel J. Empirical management of urinary tract infections complicating transrectal ultrasound guided prostate biopsy. J Urol 2003;169:1762-5.
19. Suzuki M, Kawakami S, Asano T, Masuda H, Saito K, Koga F, et al. Safety of transperineal 14-core systematic prostate biopsy in diabetic men. Int J Urol 2009;16:930-5.
20. Jeon SS, Woo SH, Hyun JH, Choi HY, Chai SE. Bisacodyl rectal preparation can decrease infectious complications of trans- rectal ultrasound-guided prostate biopsy. Urology 2003;62:
461-6.
21. Utrera NM, Álvarez MB, Polo JM, Sánchez AT, Martínez JP, González RD. Infectious complications after transrectal ultra- sound-guided prostatic biopsy. Analysis of our experience.
Arch Esp Urol 2011;64:605-10.
22. Pal RP, Elmussareh M, Chanawani M, Khan MA. The role of a standardized 36 core template-assisted transperineal prostate biopsy technique in patients with previously negative transrec- tal ultrasonography-guided prostate biopsies. BJU Int 2012;
109:367-71.
23. Loeb S, Carter HB, Berndt SI, Ricker W, Schaeffer EM. Is repeat prostate biopsy associated with a greater risk of hospitali- zation? Data from SEER-Medicare. J Urol 2013;189:867-70.
24. Pinkhasov GI, Lin YK, Palmerola R, Smith P, Mahon F, Kaag MG,
et al. Complications following prostate needle biopsy requiring hospital admission or emergency department visits: experi- ence from 1000 consecutive cases. BJU Int 2012;110:369-74.
25. Lee SH, Chen SM, Ho CR, Chang PL, Chen CL, Tsui KH. Risk factors associated with transrectal ultrasound guided prostate needle biopsy in patients with prostate cancer. Chang Gung Med J 2009;32:623-7.
26. Zaytoun OM, Anil T, Moussa AS, Jianbo L, Fareed K, Jones JS.
Morbidity of prostate biopsy after simplified versus complex preparation protocols: assessment of risk factors. Urology 2011;77:910-4.
27. de la Taille A, Antiphon P, Salomon L, Cherfan M, Porcher R, Hoznek A, et al. Prospective evaluation of a 21-sample needle biopsy procedure designed to improve the prostate cancer detection rate. Urology 2003;61:1181-6.
28. Berger AP, Gozzi C, Steiner H, Frauscher F, Varkarakis J, Rogatsch H, et al. Complication rate of transrectal ultrasound guided prostate biopsy: a comparison among 3 protocols with 6, 10 and 15 cores. J Urol 2004;171:1478-80; discussion 1480-1.
29. Argyropoulos AN, Doumas K, Farmakis A, Liakatas I, Gkialas I, Lykourinas M. Time of administration of a single dose of oral levofloxacin and its effect in infectious complications from transrectal prostate biopsy. Int Urol Nephrol 2007;39:897- 903.
30. Li H, Yan W, Zhou Y, Ji Z, Chen J. Transperineal ultrasound- guided saturation biopsies using 11-region template of pros- tate: report of 303 cases. Urology 2007;70:1157-61.
31. Raaijmakers R, Kirkels WJ, Roobol MJ, Wildhagen MF, Schrder FH. Complication rates and risk factors of 5802 transrectal ultrasound-guided sextant biopsies of the prostate within a population-based screening program. Urology 2002;60:826- 30.
32. Chiang IN, Chang SJ, Pu YS, Huang KH, Yu HJ, Huang CY. Major complications and associated risk factors of transrectal ultra- sound guided prostate needle biopsy: a retrospective study of 1875 cases in taiwan. J Formos Med Assoc 2007;106:929-34.