172
• 교신저자:정승일, 전남대학교 의과대학 비뇨기과학교실 전남 화순군 화순읍 서양로 322 우 519-763
Tel: 061-379-8160, Fax: 061-379-7750, E-mail: [email protected] Received: August 22, 2012
Revised: September 6, 2012 Accepted: October 5, 2012
급성전립선염 환자에서 이전 술기 유무에 따른 임상적 고찰
전남대학교 의과대학 비뇨기과학교실
김광호∙황의창∙김선옥∙정승일∙강택원∙권동득∙박광성
[Abstract]
Clinical Study According to Presence of Prior Manipulation in Patients with Acute Bacterial Prostatitis
Kwang Ho Kim, Eu Chang Hwang, Sun Ouck Kim, Seung Il Jung, Taek Won Kang, Dong Deuk Kwon, Kwang Sung Park
From the Department of Urology, Chonnam National University Medical School, Gwangju, Korea
Purpose: Acute bacterial prostatitis (ABP) is uncommon and proper guidelines concerning antibiotic ad-
ministration for ABP with urologic procedure are unclear. We retrospectively analyzed clinical symptoms and etiologic organism in ABP according to presence of prior urologic manipulation.
Materials and Methods: The clinical records of 65 patients who had been treated for ABP between
January 2007 and December 2011 were reviewed. We analyzed parameters including history taking, phys- ical examination, prior manipulations, antibiotics administration, mean length of treatment, complications, urinalysis, and urine and blood culture. Results were analyzed according to two subgroups; Group 1, those without prior urologic manipulation, and Group 2, those with prior manipulation.
Results: The population of Group 1 was 22 (33.8%) and Group 2 was 43 (66.2%). The mean age of the pa-
tients in both groups were 56.5±15.6 years and 64.0±12.5 years, respectively. Of the clinical symptoms in both
groups, fever was most common (81.8% and 83.7%). The mean pyuria grades were 2.82±0.37 and 3.47±0.25
each in both groups. In group 2, prostatic biopsy (36, 83.7%) was the most frequent manipulation of the
patients. Dysuria and storage symptoms were significantly more frequent in Group 1. The number of diabetes
mellitus patients and the admission rates were higher in Group 2. E. coli was the most frequently isolated
pathogen from urine and blood (23.1% and 24.6%, respectively). Resistance to ciprofloxacin was very high in group 1 (60.0%) and group 2 (83.3%). However, there was no significant difference between the two groups.
Conclusions: Resistance rates to ampicillin and ciprofloxacin in ABP were very high in all patients.
The resistance rates were higher in patients with prior manipulation, but there was no significant difference. When we consider high resistance to ciprofloxacin in ABP, more careful attention should be paid to empirical treatment of ABP patients with prior manipulation. (Korean J UTII 2012;7:172-177)
Key Words: Prostatitis, Prostate, Biopsy, Antimicrobial drug resistance
서 론
급성 전립선염은 실제 전립선의 감염상태를 직접 확인하기 어려워 임상증상에 따라 진단하여 치료방 법을 결정한다.
1이는 전립선염의 5% 정도를 차지하 고 치료하지 않으면 패혈증과 같은 치명적인 결과를 초래할 수 있다.
2급성전립선염의 주된 원인균으로 는 Escherichia coli (E. coli), Enterococcus, Proteus, Pseudomonas, Klebsiella, 및 Serratia 등이 알려져 있 다. 치료로는 요배양 또는 혈액배양 검사결과가 나 오기 전에 전신증상이 있으면 항생제의 경정맥 투여 로 치료를 시작하고 이후 경구용 항생제로 전환한 다. 급성 전립선염의 경우 그간 많은 연구가 있어 왔으나 비뇨기계 술기 이후 발생한 급성전립선염은 상대적으로 보고가 적었다. 최근 비뇨기계 술기 중 에서도 전립선 조직검사가 점차 늘어나는 추세지만 이러한 술기 여부에 따른 항생제의 적절한 선택과 투여 방법 및 투여 기간도 현재까지 정립이 되지 않 은 상태이다.
이에 저자들은 급성전립선염의 적절한 치료를 위해 비뇨기과 술기 여부에 따라서 발생하는 전립 선염과 일반 전립선염과의 차이를 비교하였고 향 후 진료지침을 위한 기초자료로 삼고자 하였다.
대상 및 방법
2007년 1월부터 2011년 12월까지 본원에 내원한 환자 중 급성전립선염으로 치료받은 환자 65명의 의무기록을 후향적으로 조사하였다. 급성 전립선염
은 임상증상 (발열, 하부요로증상)과 혈액검사 결과 (백혈구증가증)에 근거하여 진단하였다. 환자는 비 뇨기과 시술을 받았던 군과 받지 않은 두 군으로 나누었고 전립선염과 직접적 연관이 없다고 알려 진 만성질환 (고혈압, 당뇨)이 있는 환자의 경우도 포함시켰다.
3환자의 임상증상, 배양균, 투여항생제 종류, 배양균의 항생제 내성 등을 조사하였고 배뇨 증상 및 방광저장증상도 분석하였다. 급성요폐는 잔뇨가 400ml 이상으로 정의하였으며 발열은 37.5 도 이상으로 정의하였다. 농뇨는 요검사상 현미경 하 백혈구가 4개 이상인 것으로 정의하였으며 요검 사상 백혈구에 따라서 5개의 grade로 구분하였다.
요검사에서 백혈구 0-2를 grade 1, 백혈구 3-5를 grade 2, 백혈구 6-10을 grade 3, 백혈구 11-20을 grade 4, 그 이상의 백혈구를 grade 5로 정의하였고 각 군의 평균 grade를 비교하였다.
통계학적인 검증은 chi-square test, student's T-test 를 이용하였으며, p value가 0.05 미만일 때 통계학 적으로 유의한 것으로 판정하였다.
결 과
1군은 22명 (33.8%), 2군은 43 (66.2%)으로 처치는
전립선 조직검사가 36명 (83.7%)으로 가장 많았다
(Table 1). 각 군의 평균 나이는 1군이 56.5±15.6, 2군
이 64.0±12.5이었다. 임상증상은 두 군 모두 발열이
각각 81.8%, 83.7%로 가장 흔했으며, 배뇨통과 방광
저장증상이 비처치군에서 유의하게 많았다 (p-val-
ue<0.05) (Table 2). 만성질환에서도 당뇨병을 가지고
있는 환자가 각각 13.6%, 55.8%로 처치군에서 유의
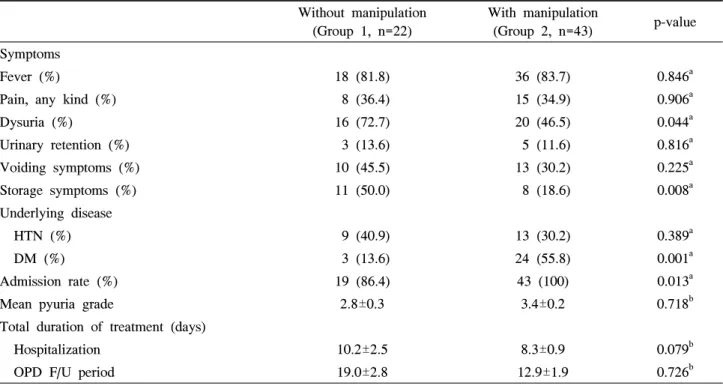
Table 2. Characteristics of the disease of 65 patients with acute bacterial prostatitis Without manipulation
(Group 1, n=22)
With manipulation
(Group 2, n=43) p-value Symptoms
Fever (%) 18 (81.8) 36 (83.7) 0.846a
Pain, any kind (%) 8 (36.4) 15 (34.9) 0.906a
Dysuria (%) 16 (72.7) 20 (46.5) 0.044a
Urinary retention (%) 3 (13.6) 5 (11.6) 0.816a
Voiding symptoms (%) 10 (45.5) 13 (30.2) 0.225a
Storage symptoms (%) 11 (50.0) 8 (18.6) 0.008a
Underlying disease
HTN (%) 9 (40.9) 13 (30.2) 0.389a
DM (%) 3 (13.6) 24 (55.8) 0.001a
Admission rate (%) 19 (86.4) 43 (100) 0.013a
Mean pyuria grade 2.8±0.3 3.4±0.2 0.718b
Total duration of treatment (days)
Hospitalization 10.2±2.5 8.3±0.9 0.079b
OPD F/U period 19.0±2.8 12.9±1.9 0.726b
a: Chi-square test, b: Student's t-test
HTN: Hypertension, DM: Diabetes mellitus, OPD: Out patient department, F/U: follow up Table 1. Urologic procedures in acute prostatitis
patients with manipulation
Procedure Number of patients (%)
Sono guided prostate biopsy 36 (83.7)
Foley catheterization 5 (11.6)
Urodynamic study 1 (2.3)
Internal urethrotomy 1 (2.3)
Total 43
Table 3. Distribution of antimicrobial agents in patients Antimicrobial agent Group 1
(n=22)
Group 2 (n=43)
Quinolone 9 (40.9%) 8 (18.6%)
3rd generation cephalosporin 7 (31.8%) 26 (60.5%)
Carbapenem 1 (4.5%) 8 (18.6%)
Clindamycin 2 (9.1%) 0
Vancomycin 1 (4.5%) 0
Piperacillin 2 (9.1%) 1 (2.3%)
하게 많았으며 (p-value<0.05), 입원 치료에 있어서도 입원율이 각각 19명 (86.4%), 43명 (100%)으로 유의 하게 더 높았으나 (p-value<0.05) (Table 2) 치료기간 에 있어서는 입원치료 10.23±2.5일, 8.33±0.9일 및 퇴 원치료 19.09±2.9일, 12.93±1.9일로 통계적인 차이는 없었다. 항생제 처방은 1군에서는 quinolone 9명 (40.9%), 3세대 cephalosporin 7명 (31.8%)이 대부분을 차지하였고 2군에서는 3세대 cephalosporin이 26명 (60.5%), carbapenem 8명 (18.6%)이 대부분을 차지하
였다 (Table 3).
요배양검사에서 양성인 환자가 1군이 7명 (31.8%), 2군이 15명 (34.9%)로 두 군 간에 비슷한 양상을 보 였다. 배양균주로 E. coli가 각각 4명 (18.2%), 11명 (25.6%)으로 가장 많았다 (Table 4). 혈액배양검사에 서 양성인 환자는 1군에서 4명 (18.2%), 2군에서 14 명 (32.6%)으로 2군에서 높은 비율을 보였으나 통계 적으로 유의하지는 않았다 (p-value=0.22) (Table 4).
배양균주는 E. coli가 각각 2 (9.1%), 14 (32.6%)로 가
Table 5. Antibiotic resistant of pathogens in patients with culture positivity
Antimicrobial agent Group 1 (%) Group 2 (%) p-value
Ampicillin 6 (60.0) 18 (75.0) 0.382
1st generation cephalosporin 5 (50.0) 9 (37.5) 0.500
3rd generation cephalosporin 3 (30.0) 4 (16.7) 0.381
Ciprofloxacin 6 (60.0) 20 (83.3) 0.144
Amikacin 0 1 (4.2) 0.512
Clindamycin 2 (20.0) 1 (4.2) 0.138
Gentamicin 3 (30.0) 10 (41.7) 0.524
Imipenem 0 1 (4.2) 0.512
Vancomycin 0 0
: Chi-square test
Table 4. Microbiological spectrum from urine & blood culture of patients
Group 1 (%) Group 2 (%) Total (%) p-value
Urine culture positive 7 (31.8) 15 (34.9) 22 (33.8) 0.805
E. coli 4 (18.2) 11 (25.6) 15 (23.1)
P. aeruginosa 0 3 (7.0) 3 (4.6)
S.aureus 1 (4.5) 0 1 (1.5)
Klebsiella pneumoniae 1 (4.5) 0 1 (1.5)
P. fluorescens 0 1 (2.3) 1 (1.5)
Enterococcus faecalis 1 (4.5) 0 1 (1.5)
Blood culture positive 4 (18.2) 14 (32.6) 18 (27.7) 0.220
E. coli 2 (9.1) 14 (32.6) 16 (24.6)
Enterobacter cloacae 1 (4.5) 0 1 (1.5)
Corynebacterium 1 (4.5) 0 1 (1.5)
Urine & Blood culture positive 1 (4.5) 5 (11.6) 6 (9.2) 0.351
Urine or Blood culture positive 10 (45.5) 24 (55.8) 34 (52.3) 0.429
: Chi-square test
장 많았다. 요배양검사와 혈액배양검사에서 모두 양 성인 환자는 1군이 1명 (4.5%), 2군이 5명 (11.6%)이 였으며 요배양검사 또는 혈액배양검사에서 양성인 환자는 1군이 10명 (45.5%), 2군이 24명 (55.8%)으로 모두 처치군이 더 높은 비율을 보였으나 통계적인 차이는 없었다 (Table 4).
요 또는 혈액에서 배양된 균들의 항생제 내성검 사에서 ciprofloxacin이 1군에서 6명 (60.0%), 2군에 서 20명 (83.3%)으로 가장 높은 내성율을 보였고 다음으로 ampicillin이 각각 6명 (60.0%), 18명 (75.0%)으로 높았다. 1세대 cephalosporin의 내성율 은 각각 5명 (50.0%), 9명 (37.5%)이었고 3세대 cephalosporin의 내성율은 3명 (30.0%), 4명 (16.7%)
이었으며 모든 항생제 내성비율은 두 군 간에 통계 적인 차이는 없었다 (Table 5). 2군에서 amikacin, imipenem 내성균이 각각 1개씩 검출 되었고 vanco- mycin 내성균은 두 군 모두 없었다 (Table 5). 2군 환자 중 전립선 조직검사를 시행 받은 환자 1명의 요검사 및 혈액검사에서 ciprofloxacin과 ampicillin에 모두 내성이 있는 E. coli가 동정 되었고 환자는 패 혈증으로 인하여 사망하였다.
고 찰
급성전립선염은 임상증상 및 요배양검사로 진단
되며 패혈증과 같은 심각한 감염을 유발할 수 있
다. 임상증상으로는 갑작스러운 고열과 오한, 하부 요통, 회음부통증, 빈뇨, 요급박, 야간뇨, 배뇨통, 배 뇨곤란 등이 발생하고 소변에서는 농뇨, 현미경적 혈뇨, 세균뇨 등이 관찰된다. 근육통, 관절통 등도 흔한 증상으로 알려져 있다.
4,5본 연구에서는 고열 이 약 80% 이상으로 주된 증상이었고 배뇨통, 배뇨 곤란 증상이 비처치군에서 유의하게 더 높은 비율 을 보였다. 처치군 에서 입원율이 100%로 비처치 군과 유의한 차이를 보였는데 이는 대부분의 처치 가 전립선 조직검사였고 조직검사를 입원하여 시 행하였기 때문으로 생각된다.
당뇨병은 전립선 생검 후 감염 합병증 발생의 위 험인자라는 보고가 있다.
6본 연구에서도 2군에서 당뇨병 환자가 유의하게 더 많았는데 이는 전립선 조직검사 후에 발생한 급성전립선염의 위험인자로 당뇨병이 영향을 끼쳤을 것으로 생각한다.
급성 전립선염의 일반적 치료는 소변과 혈액의 배양검체를 얻은 후 즉시 경험적 항생제 치료를 시 도한다. 급성전립선염의 치료 항생제로는 광범위한 항균력을 가진 3세대 cephalosporin 계열을 amino- glycoside와 병행하여 사용할 수 있고 qinolone을 단 독으로 사용할 수 있다.
7본 연구에서도 1군에서는 주로 3세대 cephalosporin (31.8%)과 quinolone (40.9%)을 사용하였는데 2군에서는 주로 quinolone (18.6%) 보다는 3세대 cephalosporin (60.5%)과 car- papenem (18.6%)을 사용하였다. 배양검사가 나오지 않은 경우에는 경험적 항생제가 사용되었고 배양 결과 균이 검출된 경우에는 배양 검사 결과에 따라 서 항생제가 사용되었다. 따라서 항생제 내성정도 에서 2군에서 더 높은 경향을 보였으며 이에 따른 항생제의 사용의 차이가 있었다고 생각한다.
급성 전립선염의 원인균으로는 E. coli가 28%로 알려져 있는데 본 연구에서도 E. coli가 요 및 혈액 배양 검사에서 각각 23.1%, 24.6%로 가장 높은 양 성률을 보였다.
7전립선 조직검사 후 합병증을 줄이는 것으로 잘 알려진 quinolone이 조직검사 전 예방적 항생제로 추천되어 널리 사용되었지만
8,9최근 여러 연구에서 전립선 조직검사 후 quinolone 내성균의 검출이 상 승되고 있다고 보고하고 있다.
10-13Park 등의 국내연구에서도 급성신우신염이나 복잡 성 요로감염 환자에서 E. coli가 ciprofloxacin에 대한 높은 내성율이 높다는 것과 ertapenem 및 ceftriaxone 이 항균 효과가 높다는 것을 보고 하였고 이런 환자 의 치료 항생제로 ertapenem을 사용하자고 주장하였 다.
14Shin 등의 국내연구에서 quinolone을 전립선 조 검검사의 예방적 항생제로 사용 후, 균혈증 발생 시 quinolone 내성이 높아 3세대 cephalosporin을 증상 발생시 즉각적으로 사용할 것을 권장하였다.
13본 연구에서도 1군과 2군 모두에서 ciprofloxacin 내성균이 각각 6명 (60.0%), 20명 (83.3%)로 검출 되 었으며 이는 과도한 quinolone 계열의 항생제 사용이 원인일 것으로 생각된다. 특히 1군과 비교하여 2군 에서 ciprofloxacin의 내성율이 더 높았고 imipenem에 내성인 균도 동정된 것을 볼 때 급성 전립선염 환자 에 있어서 항생제 배양결과가 나오기 전까지 사용되 는 경험적 치료항생제 선택에 있어서 이전 술기 여 부에 따라 다른 내성 패턴을 고려해야 할 것으로 생 각된다. 최근 quinolone 내성이 전 세계적으로 증가 되는 추세이고 이로 인해서 환자의 직장에 존재하는 내성균이 많게는 22%까지 보고되고 있다.
15전립선 생검 후 전립선염 발생과 같은 감염 합병 증도 증가 추세이며 이러한 원인은 quinolone 내성 으로 해석되고 있으며,
16본 연구에서 발병전 전립 선 생검이 많았기에 이처럼 높은 quinolone 내성을 보였다고 볼 수 있겠다.
본 연구의 1군과 2군 간의 비교에서 2군에서 항 생제 내성이 높은 경향을 보였으나 항생제 내성균 에서 통계적인 차이가 거의 없다는 것은 대상 환자 수가 적은 것으로 인한 한계점으로 생각되며 향후 보완해야 하겠다. 향후 비뇨기과적인 시술을 받은 환자에서 내성균에 의한 요로 감염의 가능성이 높 다는 점을 고려하여 치료 항생제를 선택한다면 향 후 급성전립선염 환자의 효과적인 치료에 도움이 될 것으로 생각한다.
결 론
급성전립선염의 비뇨기과적인 술기를 받은 환자
에 있어서 시술을 받지 않은 환자보다 동반 질환으
로 당뇨가 많았으며, 증상에 있어서는 배뇨통, 저장 증상이 더 많았으나 세균뇨나 균혈증의 비율은 큰 차이가 없었다. 요 및 혈액배양 검사에서 대부분 E.
coli가 동정되었으며 ampicillin과 ciprofloxacin에 높 은 내성을 보였다. 두 군 간의 통계적인 차이는 없 었으나 발병전 비뇨기과 시술을 받은 환자에서 항 생제 내성이 높은 경향을 보였다. 특히 급성전립선 염의 항생제 치료에 있어서 ciprofloxacin 내성률이 높다는 것을 고려하여 경험적인 항생제를 선택한다 면 효과적인 치료를 할 수 있을 것으로 생각된다.
REFERENCES