958 서 론
유리형 전립선특이항원, 전립선특이항원밀도, 전립선특 이항원속도와 같은 전립선특이항원 (prostate-specific anti- gen; PSA)과 연관된 여러 지표들이 전립선암의 조기 진단에 도움을 주고 있다. 그러나 혈중 PSA는 전립선암뿐만 아니 라 전립선비대증, 전립선염, 경직장초음파 유도 전립선생검 (transrectal ultrasound guided prostate biopsy; TRUS-Bx) 자체 에 의해서도 증가할 수 있다.1
일반적으로 혈중 PSA의 증가나 직장수지검사에서 비정
상적인 소견을 보이는 경우 TRUS-Bx를 시행하고 있다. 그 러나 이러한 적응증을 기준으로 전립선생검을 시행할 때 실제 임상에서 전립선생검 결과 음성소견을 보이는 경우가 많아 전립선암 진단의 특이도를 높이기 위한 노력이 지속 되어 왔다. 이러한 노력에도 불구하고 Catalona 등2이 시행 한 대규모 연구에서 전립선생검의 음성률이 75%에 이를 것 으로 예상하였다. 또한 전립선암이 의심되나 생검에서 음 성일 때 재생검을 고려하게 되나 이는 환자와 비뇨기과 의 사에게 정신적으로 큰 부담을 주고 있어 전립선 재생검 여 부를 결정할 수 있는 유용한 지표가 있다면 임상적으로 매 우 유용할 것이다.
The Significance of Prostate-specific Antigen after Transrectal Prostate Biopsy
Seock Hwan Choi, Eun Sang Yoo1, Youg II Park
From the Department of Urology, Fatima Hospital, 1Kyungpook National Uni- versity School of Medicine, Daegu, Korea
Purpose: The serum prostate-specific antigen (PSA) level is increased after needle biopsy (Bx) of the prostate. This study tested the hypothesis that the prostate that harbors malignant lesions demonstrates less leakage of PSA after transrectal prostate Bx, and this phenomenon can be helpful in discriminating benign protrates from cancer ous prostrates.
Materials and Methods: Eighty three patients were included in this prospective study because they had an increase PSA level (from 4 to 30ng/ml) and/or an abnormal digital rectal examination, and the serum PSA level was checked 60 minutes later after biopsy. We checked the pre-Bx total serum PSA, the post-Bx total serum PSA and the PSA ratio
(post-Bx total serum PSA to pre-Bx total serum PSA), and we analyzed the sensitivity, specificity, positive predictive value, negative predictive value and the statistical differences.
Results: Of the 31 men whose PSA ratio was less than 2.0, 27 (87%) men were proven to have prostate cancer. Of the 52 men whose PSA ratio was greater than 2.0, 49 (94%) were proven to have benign lesions. When setting 2.0 as the cutoff value, the difference was statistically significant (p<0.001); the sensitivity was 90.0%, the specificity 92.4%, the positive predictive value (PPV) 87.0% and the negative predictive value (NPV) 94.2%.
Conclusions: Evaluating the 1-hour PSA ratio might be helpful for clinicians to diagnosis the high risk patients who might have cancer in their prostate glands. Repeat biopsy should be considered for patients who initially had negative biopsy results with a smaller PSA ratio. (Korean J Urol 2006;47:958-962)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Key Words: Prostate cancer, Prostate-specific antigen, Needle biopsy
대한비뇨기과학회지 제 47 권 제 9 호 2006
대구파티마병원 비뇨기과,
1경북대학교 의과대학
비뇨기과학교실
최석환․유은상1․박용일
접수일자:2006년 3월 3일 채택일자:2006년 8월 9일
교신저자: 박용일
대구파티마병원 비뇨기과 대구시 동구 신암동 302-1 ꂕ 701-600
TEL: 053-940-7150 FAX: 053-954-7417 E-mail: uropone@
yahoo.co.kr
최근 Lin 등3은 TRUS-Bx 후 혈중 PSA가 전립선암 환자보 다 전립선비대증 환자에서 크게 상승하는 현상을 보고하였 으며 생검 후 60분 뒤 혈중 PSA를 측정하여 그 의의에 대해 기술하였다.
이에 저자들은 전립선암이 의심되는 환자를 대상으로 TRUS-Bx 후 혈중 PSA의 상승 정도, 기저치와의 비율과 최 종 병리소견을 비교, 분석하여 TRUS-Bx 후 혈중 PSA의 임 상적 의의를 알아보고자 하였다.
대상 및 방법
2004년 6월부터 2005년 5월까지 본원 비뇨기과에 내원한 환자 중 직장수지검사에서 비정상적인 소견을 보이거나 혈 중 PSA가 4.0ng/ml 이상인 환자 150명을 대상으로 TRUS- Bx를 시행하였다. 이 중 혈중 PSA가 4.0-30.0ng/ml인 환자 83명에서 TRUS-Bx 시행 60분 후 혈중 PSA를 측정하였다.
환자의 평균연령은 63.4세 (39-85)였다.
대상 환자들은 조직검사 시행 24시간 전부터 시행 72시 간 후까지 4일간 levofloxacin 경구용 항생제를 투여 받았으 며 생검 30분 전 soap-saline 관장을 실시하였다. 조직검사는 좌측와위 상태에서 경직장초음파 유도로 시행하였다. 경직 장초음파 (ACUSON Sequoia512, Siemens, Germany) 10MHz 탐촉자를 이용하여 타원체 체적공식 (높이x길이x넓이x0.52) 에 의해 전립선 용적을 측정하였고, 경직장초음파 유도하 에 18G 생검침을 이용하여 조직검사를 시행하였다. 기존의 6부위 생검에 2부위의 전립선 이행대를 포함하는 8부위 생 검을 기본으로 하였으며 초음파에서 저반향부위나 직장수 지검사에서 결절이 있는 부위에 대해 생검을 추가하였다.
생검 전의 혈중 PSA는 직장수지검사와 경직장초음파를 시 행하기 전에 시행하였으며 chemiluminescent immunoassay (Immulite2000, Diagnostic Products Corporation, USA) 방법으 로 측정하였다. 생검 후의 혈중 PSA는 마지막 8번째 전립선 조직을 얻은 시점부터 60분 후에 시행하였다.
TRUS-Bx 전후 혈중 PSA값과 PSA 비율 (PSA ratio; post- Bx total serum PSA to pre-Bx total serum PSA)을 구하고 PSA 비율 1.5, 2.0, 2.5, 3.0, 3.5를 결정값 (cutoff value)으로 사용 하여 각각에 따른 민감도, 특이도를 구하였다. 수신기작동 특성 방법 (receiver operating characteristics; ROC)을 이용하 여 가장 효과적인 결정값을 정하고 이제 따른 양성 예측치, 음성 예측치를 구한 후 비교분석하였다.
통계학적인 검증은 Student's t-test, Pearson chi-square test 를 이용하였고, p값이 0.05 미만일 때 통계적으로 의미 있는 것으로 간주하였으며 통계 프로그램은 SPSS (Ver 12.0)를 사용하였다.
결 과
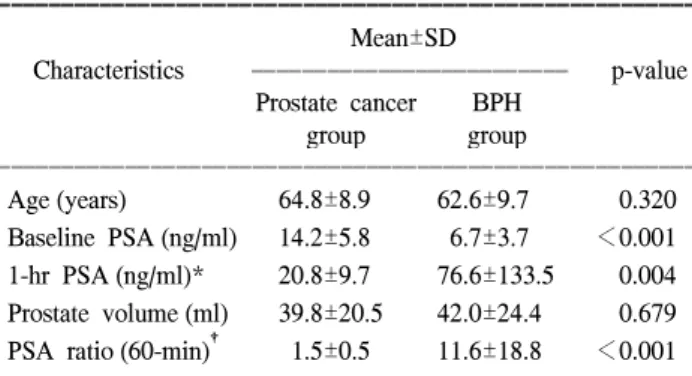
총 83명 환자의 전립선생검 결과 전립선암, 전립선비대 증, 전립선염으로 분류할 수 있었으며, Lin 등3의 연구에서 와 마찬가지로 전립선염 환자군의 혈중 PSA 변화는 전립선 비대증 환자군의 혈중 PSA 변화와 큰 차이가 없었고 기본 적으로 양성원형 (benign prototype)을 따르므로 전립선암, 전립선비대증의 양 군으로만 분류하였다. 전립선암 환자군, 전립선비대증 환자군은 각각 30명 (36%), 53명 (64%)이었으 며 연령분포는 각각 64.8±8.9세, 62.6±9.7세였다. 전립선암 환자군의 생검 전후의 혈중 PSA 평균값은 각각 14.2ng/ml, 20.8ng/ml였고 전립선비대증 환자군의 생검 전후의 혈중 PSA 평균값은 각각 6.7ng/ml, 76.6ng/ml였다. 전립선암 환자 군과 전립선비대증 환자군의 혈중 PSA 비율의 평균값은 각 각 1.5, 11.6이었다. 연령과 전립선용적은 두 군 간에 차이가 없었으나 TRUS-Bx 전후의 혈중 PSA와 PSA 비율은 통계적 으로 유의한 차이가 있었다 (Table 1) (p<0.001, p<0.004).
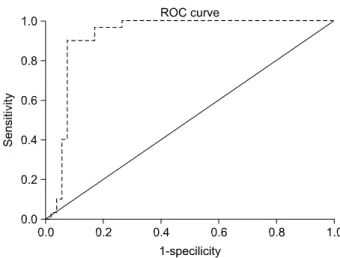
1.5, 2.0, 2.5, 3.0와 3.5를 결정값으로 하였을 때 각각의 PSA 비율에 따른 전립선암과 전립선비대증 두 군의 환자구 성, 민감도, 특이도를 구하였다 (Table 2). 모든 환자의 PSA 비율을 바탕으로 ROC curve를 구하였으며 (Fig. 1), 가장 적 절한 결정값은 2.0이었다.
PSA 비율이 2.0 미만인 31명 중 27명 (87%)에서 전립선암 이 발견되었고, PSA 비율이 2.0 이상인 52명 중 49명 (94%) 이 전립선비대증으로 진단되었다. 결정값을 2.0으로 정의하 였을 때 통계적으로 유의한 차이를 보였으며, 민감도 90.0%, 특이도 92.4%, 양성 예측치 87.0%, 음성 예측치 94.2%였다 (Table 2) (p<0.001).
Table 1. Characteristics of the study groups
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Mean±SD
Characteristics ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ p-value Prostate cancer BPH
group group
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Age (years) 64.8±8.9 62.6±9.7 0.320
Baseline PSA (ng/ml) 14.2±5.8 6.7±3.7 <0.001 1-hr PSA (ng/ml)* 20.8±9.7 76.6±133.5 0.004 Prostate volume (ml) 39.8±20.5 42.0±24.4 0.679 PSA ratio (60-min)† 1.5±0.5 11.6±18.8 <0.001 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ BPH: benign prostatic hyperplasia, PSA: prostate-specific antigen, SD: standard deviation, *: PSA 1 hour after biopsy, †: ratio of PSA change 1 hour after biopsy to baseline PSA
고 찰
전립선암은 미국의 성인 남성에서 발생하는 가장 흔한 악성 종양으로 우리나라 또한 최근 노령 인구의 증가와 함 께 서구식 식생활로 인해 전립선암 발생 빈도가 점차 증가 하는 추세이다.4-7 전립선암의 진단을 위해서는 혈중 PSA 측정, 직장수지검사, 경직장초음파검사 등을 시행하고 있으 며 전립선암의 확진을 위해 전립선생검은 필수적인 검사이 다.8,9
혈중 PSA는 1979년 Wang 등10이 처음으로 전립선에서 추 출한 종양 표식자로 34,000dalton의 저분자량 당단백질로 구성되어 있으며, 전립선에 특이적이지만 전립선암에는 비 특이적이어서 전립선비대증을 비롯한 다양한 양성질환에 서도 증가될 수 있어 상대적으로 특이도가 낮은 편이다.1 전립선암 진단의 특이도를 높이기 위해 총 혈중 PSA 이외 에 연령특이 전립선특이항원, 총 PSA에 대한 유리형 PSA의 비율, 전립선특이항원밀도, 전환대전립선특이항원밀도 및 전립선특이항원속도 등이 연구되어 왔다.
Catalona 등11은 혈중 PSA 4-10ng/ml의 환자들에서 전립선 특이항원밀도의 결정값을 0.15로 하여 조직검사를 시행하 였을 때 약 50%의 전립선암 진단 위음성률을 보고하였다.
국내 연구의 경우 Lee 등12은 전립선암군과 비전립선암군에 서 전립선특이항원밀도는 통계적 유의성을 보였고 이는 서
양인을 대상으로 한 기존의 연구 결과와 같이 전립선특이 항원밀도는 전립선암의 예측에 있어서 인종적 차이가 없는 것으로 생각하였으나 진단적 검사라는 측면에서는 아직 미 흡하다고 보고하였다. Carter 등13은 전립선특이항원속도 결 정값을 0.75ng/ml/year로 하였을 때 특이도는 혈중 PSA 4-10ng/ml과 혈중 PSA 4ng/ml 미만에서 모두 90% 이상으로 보고하였으며, 민감도는 혈중 PSA 4-10ng/ml는 79%, 혈중 PSA 4ng/ml 미만에서는 11%로 보고하였다. 국내 연구에서 Lee 등12은 전립선특이항원속도가 혈중 PSA 4-10ng/ml에서 전립선암군과 비전립선암군에서 통계적 유의성을 보였고 이는 국외의 연구 결과와 비교하였을 때 서양인과 한국인 사이의 인종적 차이가 없는 것으로 생각된다고 보고하였 다. 일반적으로 양성 전립선질환의 환자보다 전립선암으로 진단된 환자에서 총 PSA에 대한 유리형 PSA의 비율이 더
낮고,14,15 총 PSA에 대한 유리형 PSA의 비율은 전립선특이
항원 단독과 비교하였을 때 양성 예측률을 의미 있게 향상 시킨다.15 서구의 여러 연구에서 총 PSA에 대한 유리형 PSA 의 비율의 중요성에 대해 언급되고 있으며 혈중 PSA 농도 가 4-10ng/ml 사이의 값을 나타낼 때 전립선암 예측의 가장 유용한 인자로 받아들여지고 있다.2,14 국내 연구의 경우 Im 등15은 전립선암 환자군과 전립선비대증 환자군을 비교했 을 때, 총 PSA에 대한 유리형 PSA의 비율만이 의미 있게 차이가 있는 것으로 나타났고, 혈중 PSA의 범위를 10ng/ml 이하인 경우와 10ng/ml보다 높은 경우로 나누어 두 환자군 을 비교했을 때 총 PSA에 대한 유리형 PSA의 비율이 역시 의미 있게 차이가 있었다고 보고하였다. 그러나 Lee 등12의 연구에서는 혈중 PSA 4-10ng/ml을 나타내는 환자에서 총 PSA에 대한 유리형 PSA의 비율은 통계적 유의성이 없었고 Table 2. Results of using multiple cutoff values of the PSA ratio
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ No. of No. of
Sensitivity (%)/
prostate BPH
specificity (%) cancer group group
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Cutoff value 1.5 66.6/92.4
PSA ratio <1.5 20 4
PSA ratio ≥1.5 10 49
Cutoff value 2.0 90.0/92.4
PSA ratio <2.0 27 4
PSA ratio ≥2.0 3 49
Cutoff value 2.5 96.6/81.1
PSA ratio <2.5 29 10
PSA ratio ≥2.5 1 43
Cutoff value 3.0 100/71.6
PSA ratio <3.0 30 15
PSA ratio ≥3.0 0 38
Cutoff value 3.5 100/58.4
PSA ratio <3.5 30 22
PSA ratio ≥3.5 0 31
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ BPH: benign prostatic hyperplasia, PSA: prostate-specific antigen
Fig. 1. Receiver operating characteristics (ROC) curve using multi- ple cutoff values of the prostate-specific antigen (PSA) ratio, in- cluding 1.5, 2.0, 2.5, 3.0 and 3.5.
또한 ROC curve에서도 혈중 PSA 단독 검사보다 민감도나 특이도가 낮았다고 보고하였다. 연령특이 전립선특이항원 의 경우 인종마다 차이가 있으며, 특이도를 미미하게 향상 시키는 반면, 민감도에서는 다른 검사방법과 비교해 상대 적으로 낮은 것으로 나타나고 있다.16
Charrie 등17은 전립선생검 후 전립선 산성인산분해효소 와 혈중 PSA가 유의하게 상승하는 현상에 대해 처음으로 기술하였으며, 전립선암 환자보다 전립선비대증 환자에서 혈중 PSA가 크게 상승한다고 하였다. Lechevallier 등18은 전 립선생검 후 PSA kinetic profile을 작성하였으며, 그 결과 전 립선생검 후 60분에 혈중 PSA가 최대로 상승하고 30일에 기저치로 돌아온다고 하였다. 전립선생검 이후 전립선비대 증 조직보다 전립선암 조직에서 PSA가 혈청으로 적게 유리 되는 현상에 대해 아직까지 정확하게 알려진 것은 없으나 Lin 등3이 암조직의 경우 지속적으로 PSA를 누출시키고 있 어 청소와 접합의 작용 (clearance and conjugating mecha- nism)이 각성되어 있지만 양성조직의 경우 PSA가 누출되면 청소되는 데 더 많은 시간이 필요하여, 단위 조직당 생성되 는 PSA가 양성조직에서 더 많다고 주장하였다.
혈중 PSA 상승이 경도에서 중등도인 환자에서 PSA 비율 의 증가가 전립선암의 위험도를 결정하는 데 도움을 주기 때문에 혈중 PSA가 30.0ng/ml 미만인 환자만을 연구에 포함 하였다. Lin 등3은 TRUS-Bx 전후의 혈중 PSA 비율의 결정 값을 수신기작동특성 방법 (ROC)을 이용하여 2.0으로 정의 하였으며, 결정값을 2.0으로 하였을 때 민감도 78.1%, 특이 도 94.1%, 양성 예측치 92.5%, 음성 예측치 82.1%의 결과를 보고하였다. 최근 연구에서 작은 용적의 전립선생검이나 첫 번째 TRUS-Bx에서 음성으로 진단된 환자의 재생검 시 전립선이행대의 생검조직수가 많을수록 전립선암 진단율 이 높다고 보고하였으며 본 연구에서 결정값을 2.0으로 정 의하였을 때 민감도 90.0%, 특이도 92.4%, 양성 예측치 87.0%, 음성 예측치 94.2%로 Lin 등3의 연구보다 민감도와 음성예측치가 높은 것은 TRUS-Bx 시행 시 전립선이행대의 조직을 2부위 이상 포함하였기 때문인 것으로 생각된다.19,20 본 연구의 결과를 볼 때 전립선생검 60분 후 PSA를 측정 하여 PSA 비율을 전립선암의 진단에 사용하는 것이 의의가 있으며 이를 이용하여 PSA 비율이 2.0 미만일 때 재생검을 시행하는 것이 바람직하다고 생각한다. 그러나 PSA 비율이 2.0 이상으로 높은 것이 반드시 양성 전립선질환임을 보장 할 수 없으므로 임상적으로 고위험군에서는 추적관찰이 필 요하다. 다만 본 연구에서는 전립선 재생검을 시행한 증례 와 전립선비대증이 의심되는 환자군에서 경요도전립선절 제술을 시행하여 발견된 전립선암의 진단율이 추가되지 않 아 향후 충분한 경과관찰 기간을 거쳐 추가적인 연구가 필
요할 것으로 생각한다.
결 론
본 연구의 결과로 미루어 TRUS-Bx 후 PSA 비율은 총 PSA, PSA의 연령별 참조범위, 전립선특이항원밀도, 총 PSA에 대한 유리형 PSA의 비율, 전환대전립선특이항원밀 도 및 전립선특이항원속도와 더불어 전립선암을 진단하는 데 효과적인 도구가 될 수 있을 것으로 생각한다. 그러므로 전립선생검 60분 후 PSA 측정을 추천하며 전립선생검 전후 PSA 비율이 2.0 미만일 때 재생검의 적응증이 될 수 있다고 생각한다. 반대로 PSA 비율이 높은 경우 양성질환임을 완 전히 보장할 수 없으므로 임상적으로 고위험군인 경우 주 의 깊게 경과관찰을 해야할 것으로 생각한다.
REFERENCES
1. Oesterling JE. prostate-specific antigen: a critical assessment of the most useful tumor marker for adenocarcinoma of the prostate. J Urol 1991;145:907-23
2. Catalona WJ, Partin AW, Slawin KM, Brawer MK, Flanigan RC, Patel A, et al. Use of the percentage of free prostate- specific antigen to enhance differentiation of prostate cancer from benign prostatic disease: a prospective multicenter clini- cal trial. JAMA 1998;279:1542-7
3. Lin TP, Huang WJ, Chen KK. Differentiation of benign prostatic hyperplasia from prostate cancer using prostate- specificfic antigen dynamic profile after transrectal prostate biopsy. J Urol 2004;171:2226-9
4. Boring CC, Squires TS, Tong T, Montgomery S. Cancer sta- tistics, 1994. CA Cancer J Clin 1994;44:7-26
5. Carter HB, Coffey DS. The prostate: an increasing medical problem. Prostate 1990;16:39-48
6. Wingo PA, Tong T, Bolden S. Cancer statistics, 1995. CA Cancer J Clin 1995;45:8-30
7. Cho IR, Chang YS, Roh JS, Jeon JS, Park SS. Change of PSA and PSAD after antibiotic treatment in patients with prostatitis.
Korean J Androl 2002;20:100-5
8. Abe M, Hashimoto T, Matsuda T, Saitoh M, Watanabe H.
Prostatic biopsy guided by transrectal ultrasonography using real-time linear scanner. Urology 1987;29:567-9
9. Devonec M, Fendler JP, Monsallier M, Mouriquand P, Mestas JL, Dutrieux-Berger N, et al. Prostatic cancer diagnosis with ultrasonically guided prostatic biopsy: results in 226 cases.
Prog Clin Biol Res 1989;303:35-40
10. Wang MC, Valenzuela LA, Murphy GP, Chu TM. Purification of a human prostate-specific antigen. Invest Urol 1979;17:159- 63
11. Catalona WJ, Richie JP, Ahmann FR, Hudson MA, Scardino
PT, Flanigan RC, et al. Comparison of digital rectal examina- tion and serum prostate-specific antigen in the early detection of prostate cancer: results of a multicenter clinical trial of 6,630 men. J Urol 1994;151:1283-90
12. Lee SC, Lee SC, Kim WJ. Value of PSA density, PSA velo- city and percent free PSA for detection of prostate cancer in patients with serum PSA 4-10ng/ml patients. Korean J Urol 2004;45:747-52
13. Carter HB, Pearson JD, Metter EJ, Chan DW, Andres R, Fozard JL, et al. Longitudinal evaluation of serum androgen levels in men with and without prostate cancer. Prostate 1995;27:25-31
14. Stenman UH, Hakama M, Knekt P, Aromaa A, Teppo L, Leinonen J. Serum concentrations of prostate-specific antigen and its complex with a1-antichymotrypsin before diagnosis of prostate cancer. Lancet 1994;344:1594-8
15. Im YJ, Hong SJ, Chung BH. Clinical application of free to total PSA ratio in detection of prostate cancer in Korean men:
lower cut-off value. Korean J Urol 2004;45:753-7
16. Mettlin C, Murphy GP, Lee F, Littrup PJ, Chesley A, Babaian
R, et al. Characteristics of prostate cancer detected in the American Cancer Society-National Prostate Cancer Detection Project. J Urol 1994;152:1737-40
17. Charrie A, Fleury-Goyon MC, Dutey P, Perrin P. The effect of prostate aspiration biopsy on serum levels of prostatic acid phosphatase and prostate-specific antigen. JAMA 1986;256:
474
18. Lechevallier E, Echazarian C, Ortega JC, Daniel L, Roux F, Thirion X, et al. Kinetics of postbiopsy levels of serum free prostate-specific antigen and percent free prostate-specific antigen. Urology 1999;53:731-5
19. Mai KT, Moazin M, Morash C, Collins JP. Transitional zone and anterior peripheral zone of the prostate. A correlation of small-volume cancer in the biopsy cores and high psa with positive anterior margins in radical prostatectomy specimens.
Urol Int 2001;66:191-6
20. Deliveliotis C, Varkarakis J, Albanis S, Argyropoulos V, Skolarikos A. Biopsies of the transitional zone of the prostate.
Should it be done on a routine basis, when and why? Urol Int 2002;68:113-7