INTRODUCTION
Point-of-care testing (POCT) allows for laboratory diagnostic tests to be performed at or near the site of clinical care. Real-time measurements of a patient’s status may be quickly obtained, assisting health care providers to address acute patient needs [1,2]. In the last 5 to 10 years, the number of rapid immunoassay applications has risen rapidly with the development of increasingly sensitive and quantitative assay techniques. These advances improve the quality of POCT and allow more
testing in doctors’ offices, emergency units, and other outpatient sites where rapid test turnaround is a greater priority than in hospital settings. Rapid immunoassays are most useful in diagnostic and long-term monitoring applications that could not previously be managed in outpatient settings such as primary care [3]. A rapid increase in the use of POCT has led to concerns about the quality and risks of these methods. Though they seem simple, sometimes POCT devices may not be innocuous [2].
Therefore, consumers and operators of these devices must be aware of the potential risks of POCT, and take steps
Performance Evaluation of the SelexOn Analyser for Seven Biomarkers
Hyun-Young Kim, Soo- Youn Lee, and Hyung- Doo Park
Department of Laboratory Medicine and Genetics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Background: SelexOn (Infopia, Korea) is a novel immunoassay instrument that measures the concentration of α-fetoprotein (AFP), creatine kinase isoenzyme (CK-MB), D-dimer, high-sensitivity C-reactive protein (hs-CRP), myoglobin, prostate-specific antigen (PSA), and thyroid-stimulating hormone (TSH) in whole blood. We evaluated the analytical performance of SelexOn.
Methods: The analytical performance of SelexOn was evaluated for precision and linearity, and compared with the ADVIA Centaur XP Immunoassay System (Siemens, Germany) and the STA-R coagulation analyser (Diagnostica Stago, France).
Results: Within-run CV ranged from 2.9% to 8.9% for all biomarkers. Between-run precision ranged from 1.6% to 11.3% for all biomarkers, except at low levels of D-dimer (16.1%).
Observed linearity ranges were AFP, 8.7 to 47.0 ng/mL; CK-MB, 4.7 to 38.7 ng/mL; D-dimer, 393.2 to 2,760.3 ng/mL; hs-CRP, 2.1 to 9.0 mg/L; myoglobin, 67.2 to 441.5 ng/mL; PSA, 2.6 to 23.7 ng/mL; and TSH, 3.3 to 38.9 mIU/L. Upon comparing SelexOn with the Centaur XP and STA-R systems, values of AFP, CK-MB, hs-CRP, and PSA showed good correlation, with correlation coefficients greater than 0.975. The correlation coefficients of TSH, myoglobin, and D-dimer were 0.9723, 0.9649, and 0.8379, respectively. The concordance was excellent for hs-CRP (kappa [κ]=0.958), PSA (κ=0.854), and TSH (κ=0.810); good for AFP (κ=0.655), CK-MB (κ=0.759), and myoglobin (κ=0.783); and moderate for D-dimer (κ=0.561).
Conclusions: SelexOn demonstrated acceptable precision, linearity, and correlation with the Centaur XP and the STA-R for seven biomarkers. Because of its speed and performance, SelexOn may facilitate the rapid screening of patients for cardiovascular disease, thyroid disease, prostate cancer, and hepatocellular carcinoma.
(J Lab Med Qual Assur 2014;36:30-38)
Key Words : Immunoassay, Cardiovascular diseases, Performance, Tumour markers
Corresponding author:
Hyung-Doo Park Department of Laboratory Medicine and Genetics, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 135-710, Korea
Tel: +82-2-3410-0290 Fax: +82-2-3410-2719 E-mail: [email protected]
pISSN: 1225-097X
eISSN: 2288-7261 Received October 16, 2013, Revision received January 31, 2014, Accepted February 19, 2014
to ensure appropriate test quality. In particular, precision and bias must be measured as a prerequisite for analytical quality management [2,4].
Recently, the SelexOn POCT analyser (Infopia, Anyang, Korea) was developed for the diagnosis, screening, and monitoring of cardiovascular disorders, thyroid disorders, and some cancers. The equipment measures the concentration of α-fetoprotein (AFP), creatine kinase (CK)-MB, D-dimer, high-sensitivity C-reactive protein (hs-CRP), myoglobin, prostate-specific antigen (PSA), and thyroid-stimulating hormone (TSH). This study evaluated the analytical performance and clinical utility of SelexOn.
MATERIALS AND METHODS
1. Test Device
The SelexOn analyser uses lateral flow immunoassays for the quantitative measurement of cardiac markers (CK- MB, myoglobin, D-dimer, and hs-CRP), tumour markers (AFP and PSA), and TSH, in EDTA-treated venous whole blood. The tests involve use of two monoclonal antibodies specific to each biomarker. After an EDTA- treated venous whole-blood specimen is injected into the sensor on a test strip, the erythrocytes are removed and each biomarker is bound by gold nanoparticle-labelled antibodies. When plasma passes through the detection zone, gold nanoparticle-labelled antibody-biomarker complexes are captured by anti-biomarker antibodies that are immobilized on a test line, and positive signals are displayed as red lines. Integrated software converts the signal intensity to a quantitative result. The analysis time for each biomarker is 10 minutes. The ranges specified by the manufacturer are as follows: AFP, 5.0 to 50.0 ng/mL;
CK-MB, 3.0 to 40.0 ng/mL; D-dimer, 100.0 to 3,000.0 ng/
mL; hs-CRP, 0.5 to 10.0 mg/L; myoglobin, 50.0 to 600.0 ng/mL; PSA, 2.0 to 30.0 ng/mL; and TSH, 0.2 to 50.0 mIU/L. The manufacturer’s reference values are: AFP,
≤10 ng/mL; CK-MB, ≤7 ng/mL; D-dimer, ≤500 ng/
mL; hs-CRP, ≤3 mg/L; myoglobin, ≤100 ng/mL; PSA,
≤4 ng/mL; and TSH, 0.5 to 5 mIU/L. This study was approved by the institutional review board of Samsung
Medical Center.
2. Precision
Experiments were performed using low-concentration and high-concentration specimens of EDTA-treated venous whole blood provided by the SelexOn manufacturer for each biomarker. Within-run CV and between-run CV were evaluated by modifying the Clinical and Laboratory Standards Institute (CLSI) guideline EP5-A2 [5]. Within- run precision was determined by replicate measurements (n=20) performed in a single run. Between-run precision was obtained by analysing each specimen twice per day for five consecutive days.
3. Linearity
Low-concentration and high-concentration specimens of EDTA-treated venous whole blood were provided by the SelexOn manufacturer for each biomarker, and three intermediate-concentration specimens were fabricated as 3:1, 2:2, and 1:3 mixtures of low and high concentration specimens, respectively. Four replicates were measured randomly at each of the five levels. Polynomial regression analysis was performed and the deviation from linearity was calculated. Linearity was determined by following CLSI guideline EP6-A [6] and the coefficient of determi- nation ( R
2) was calculated.
4. Method Comparisons
Methods were compared following CLSI guideline
EP9-A2-IR [7]. For all biomarkers except D-dimer, 100
specimens distributed over the analytical measurement
range of SelexOn were tested with both the SelexOn and
the ADVIA Centaur XP Immunoassay (Siemens, Munich,
Germany). For D-dimer, 50 specimens were tested with
both the SelexOn and the STA-R coagulation analyser
(Diagnostica Stago, Asnieres, France). EDTA-treated
venous whole blood, serum, and plasma collected at the
same time were used with the SelexOn, ADVIA Centaur
XP Immunoassay, and STA-R coagulation analyser,
respectively. Values were compared using Passing-Bablok
regression and Bland-Altman plots; kappa (κ) values
were used to estimate the concordance between assays
with a value of >0.81 considered as excellent concordance, 0.80 to 0.61 considered as good concordance, and 0.60 to 0.41 considered as moderate concordance [8].
5. Statistical analysis
Statistical analyses were performed using EP Evaluator Release 10 (David G. Rhoads Assoc., Kennett Square, PA, USA) and IBM SPSS ver. 20.0 (IBM Co., Armonk, NY, USA). For method comparisons, Passing-Bablok regression and Bland-Altman plots were made using MedCalc ver. 12.5.0.0 (MedCalc Software, Mariakerke, Belgium).
RESULTS
1. Precision
Within-run CV were 4.4% to 8.2% for AFP, 4.6% to 8.9% for CK-MB, 3.9% to 8.4% for D-dimer, 6.5% to 7.1%
for hs-CRP, 2.9% to 4.2% for myoglobin, 7.3% to 8.2% for PSA, and 4.9% to 8.4% for TSH. Between-run CVs were 1.6% to 6.7% for AFP, 6.5% to 10.5% for CK-MB, 8.1%
to 16.1% for D-dimer, 2.2% to 9.1% for hs-CRP, 2.3% to 4.7% for myoglobin, 9.6% to 11.3% for PSA, and 2.4% to 6.0% for TSH (Table 1) [9].
2. Linearity
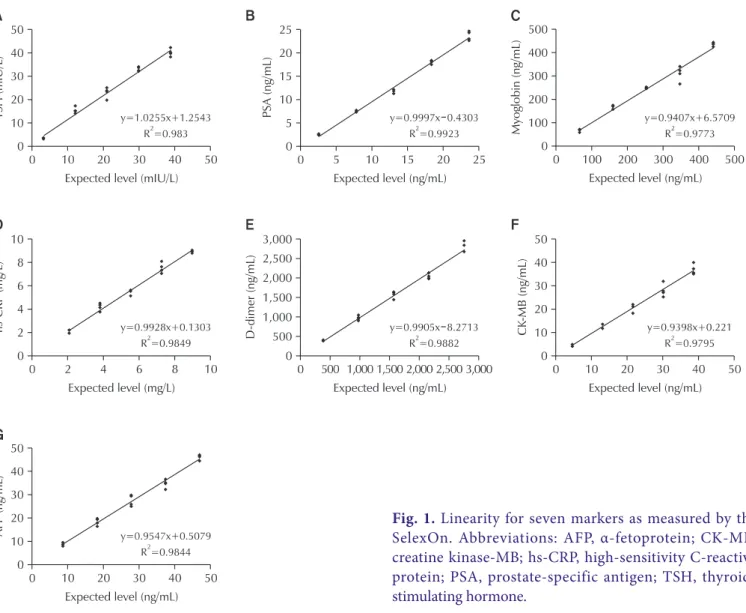
All biomarkers demonstrated acceptable linearity in their respective test ranges and the R
2-values were all greater than 0.975 (Fig. 1). The observed linearity ranges were 8.7 to 47.0 ng/mL for AFP, 4.7 to 38.7 ng/mL for CK-MB, 393.2 to 2,760.3 ng/mL for D-dimer, 2.1 to 9.0 mg/L for hs-CRP, 67.2 to 441.5 ng/mL for myoglobin, 2.6 to 23.7 ng/mL for PSA, and 3.3 to 38.9 mIU/L for TSH (Table 2).
3. Comparisons
Correlation coefficients and r-values were greater than 0.9750 for AFP, CK-MB, hs-CRP, and PSA, and were 0.9723 for TSH, 0.9649 for myoglobin, and 0.8379 for D-dimer (Fig. 2). Passing-Bablok regression analysis resulted in variable slopes ranging from 0.777 to 1.205 for all of the biomarkers. Average bias for each marker (with
Table 1. Within-run and between-run precision of SelexOn at two concentrations of each of seven markers
Biomarker Within-run precision Between-run precision CVw
(%) Desirable imprecision (%)
Mean±SD CV (%) Mean±SD CV (%)
α-Fetoprotein (ng/mL) Low 8.78±0.72 8.2 8.76±0.59 6.7 12.2 6.1
High 28.84±1.28 4.4 37.57±0.60 1.6
Creatine kinase-MB (ng/mL) Low 4.30±0.20 4.6 4.66±0.30 6.5 18.4 9.2
High 24.20±2.15 8.9 32.88±3.45 10.5
D-dimer (ng/mL) Low 494.76±41.39 8.4 441.90±71.03 16.1 NA NA
High 2,102.72±81.42 3.9 2,447.73±199.22 8.1
High-sensitivity C-reactive protein (mg/L) Low 1.09±0.08 7.1 1.41±0.13 9.1 NA NA
High 6.43±0.42 6.5 8.02±0.18 2.2
Myoglobin (ng/mL) Low 80.76±3.41 4.2 74.88±1.71 2.3 13.9 7.0
High 307.14±8.97 2.9 412.78±19.43 4.7
Prostate-specific antigen (ng/mL) Low 3.26±0.27 8.2 3.37±0.38 11.3 18.1 9.1
High 14.70±1.08 7.3 16.75±1.60 9.6
Thyroid-stimulating hormone (mIU/L) Low 3.63±0.30 8.4 6.14±0.37 6.0 19.3 9.7
High 39.36±1.94 4.9 41.02±0.97 2.4
CVw (within-subject biological variation) and desirable imprecision are from Ricos C, et al. Scand J Clin Lab Invest 1999;59:491-500, with permission from Informa Healthcare [9] and the desirable biological variation database specifications from Westgard (http://www.westgard.
com/biodatabase1.htm).
Abbreviation: NA, not applicable.
95% confidence intervals in parentheses) as evident from Bland-Altman plots is as follows: AFP, -0.5% (-2.95% to 1.88%); CK-MB, -8.7% (-12.00% to -5.42%); D-dimer,
-10.8% (-23.00% to 1.48%); hs-CRP, -3.4% (-5.74% to -0.97%); myoglobin, -5.7% (-9.45% to -1.99%); PSA, -4.1% (-7.52% to -0.62%); TSH, -6.1% (-10.63% to Fig. 1. Linearity for seven markers as measured by the SelexOn. Abbreviations: AFP, α-fetoprotein; CK-MB, creatine kinase-MB; hs-CRP, high-sensitivity C-reactive protein; PSA, prostate-specific antigen; TSH, thyroid- stimulating hormone.
Table 2. Linearity for seven markers measured by SelexOn
Biomarker Test range Observed
linear range Linear range specified by
the manufacturer Slope Intercept R2
α-Fetoprotein (ng/m) 8.7–47.0 8.7–47.0 5.0–50.0 0.955 0.508 0.9844
Creatine kinase-MB (ng/mL) 4.7–38.7 4.7–38.7 3.0–40.0 0.940 0.221 0.9795
D-dimer (ng/mL) 393.2–2,760.3 393.2–2,760.3 100.0–3,000.0 0.991 -8.271 0.9882
High-sensitivity C-reactive protein (mg/L) 2.1–9.0 2.1–9.0 0.5–10.0 0.993 0.130 0.9849
Myoglobin (ng/mL) 67.2–441.5 67.2–441.5 50.0–600.0 0.941 6.571 0.9773
Prostate-specific antigen (ng/mL) 2.60–23.70 2.60–23.70 2.0–30.0 0.999 -0.430 0.9923 Thyroid-stimulating hormone (mIU/L) 3.30–38.90 3.30–38.90 0.2–50.0 1.026 1.254 0.9830 Abbreviation: R2, coefficient of determination.
-1.47%) (Fig. 3). Values for
κ were excellent for hs-CRP,PSA, and TSH, good for AFP, CK-MB, and myoglobin, and moderate for D-dimer (Table 3).
DISCUSSION
In this study, we evaluated the linearity and precision of SelexOn and compared the SelexOn with the Centaur XP and STA-R analysers, and found that the analytical performance of SelexOn gave acceptable results. The
widely accepted quality specification for precision, also known as desirable imprecision, is analytical variation of less than one half of the average within-subject biological variation [4]. Based on this specification, the within-run CV of AFP, CK-MB, myoglobin, PSA, and TSH met the acceptance criteria for precision, except at low levels of AFP (Table 1). The within-run CV for low levels of AFP was slightly higher than the desirable imprecision, indicating that SelexOn does not have good precision at low AFP levels. However, considering that Fig. 2. Comparison of the concentrations of seven markers as measured by the ADVIA Centaur XP Immunoassay (or STA-R for D-dimer) and SelexOn. Comparisons using Passing-Bablok regression plots. Thick solid line, linear regression;
dashed lines, 95% confidence interval for the regression line; thin dotted line, theoretical line with a slope of 1.0 and a Y intercept of 0. Abbreviations: AFP, α-fetoprotein; CK-MB, creatine kinase-MB; hs-CRP, high-sensitivity C-reactive protein;
PSA, prostate-specific antigen; TSH, thyroid-stimulating hormone; CI, confidence interval.
most of the POCT immunoassays showed CVs greater than 10% [10], the within-run CV of AFP at low levels was less than 10%. The linearity for all biomarkers was acceptable within their respective test ranges (Table 2), but the tested ranges for linearity were not broad enough to confirm the manufacturer’s claims. Because the specification of SelexOn was displayed as being either over or under the detection limit when the specimen’s concentration was outside of the measurable range, we could not evaluate a sufficiently wide range of linearity.
AFP and PSA, as tumour markers, are used for the screening, diagnosis, treatment monitoring, and detection of relapses of hepatocellular carcinoma and prostate Fig. 3. Bland-Altman plots with limits of agreement for seven markers between the ADVIA Centaur XP Immunoassay (or STA-R for D-dimer) and SelexOn. Solid line, mean of concentration differences; dashed lines, limits of agreement (means of concentration differences between two assays±1.96 SD). Abbreviations: AFP, α-fetoprotein;
CK-MB, creatine kinase-MB; hs-CRP, high-sensitivity C-reactive protein; PSA, prostate-specific antigen; TSH, thyroid-stimulating hormone.
Table 3. Agreement of results for seven biomarkers mea- sured by ADVIA Centaur XP Immunoassay (or STA-R for D-dimer) and SelexOn according to the cut offs for each assay
Test items Kappa
value 95% confidence interval
α-fetoprotein 0.655 0.504–0.806
Creatine kinase-MB 0.759 0.620–0.898
D-dimer 0.561 0.329–0.794
High-sensitivity C-reactive protein 0.958 0.900–1.000
Myoglobin 0.783 0.658–0.907
Prostate-specific antigen 0.854 0.749–0.958 Thyroid-stimulating hormone 0.810 0.692–0.928
cancer, respectively [11,12]. SelexOn showed a strong correlation with Centaur XP for both AFP ( r=0.9889) and PSA ( r=0.9828), with a low average bias of -0.5% for AFP and -4.1% for PSA. PSA demonstrated a highly positive agreement (0.942) with excellent concordance (
κ=0.854).We therefore conclude that medical practitioners could use SelexOn to screen for hepatocellular carcinoma or prostatic cancer.
Cardiac markers such as troponin I, CK-MB, and myoglobin are important for the evaluation, diagnosis, and triage of patients with chest pain [13]. Although troponin I is generally known to be the most sensitive and specific marker for myocardial infarction [14], the other two cardiac markers, CK-MB and myoglobin, are useful as supportive diagnostic biomarkers. In this study, we evaluated CK-MB and myoglobin, and the comparison between SelexOn and Centaur XP showed a strong correlation for CK-MB ( r=0.9771) and myoglobin ( r=0.9649), with positive agreements of 0.930 for CK-MB and 0.923 for myoglobin. The addition of troponin to the SelexOn biomarkers may increase its clinical usefulness in the laboratory diagnosis of cardiac markers.
Increased concentrations of hs-CRP, a marker of systemic inflammation, are associated with increased risk of coronary heart disease [15]. Patients with baseline CRP concentrations in the highest quartile have two to four times the risk of future myocardial infarction, ischemic stroke, peripheral arterial disease, or sudden cardiac death compared with patients with a CRP value in the lowest quartile [16]. The United States Centers for Disease Control and Prevention and the American Heart Association have issued guidelines for using hs- CRP for primary prevention and for patients with stable coronary disease or acute coronary syndromes [17]. These guidelines included specific recommendations regarding the laboratory testing of CRP and defined cut points for clinical interpretation. Specifically, CRP <1 mg/L is considered relatively low risk, 1 to 3 mg/L is considered average, and >3 mg/L is considered relatively high risk.
Imprecision in the hs-CRP assay should be less than 10%
across the linear range of the assay [16,18]. In this study, we observed CV values lower than 10% at 1.09 mg/
L and 1.41 mg/L of hs-CRP concentrations. The kappa value (0.958) was excellent in the quantifiable range.
Unfortunately, we could not determine the precision of samples with less than 1 mg/L of hs-CRP for relatively low risk populations, because we did not have appropriate specimens with such low levels of hs-CRP.
D-dimer is increasingly used in the workup of pa- tients with suspected venous thromboembolism [19].
Commercially available D-dimer assays vary in sen- sitivity, specificity, and methodology. Sidelmann et al.
[20] demonstrated that AxSYM D-Dimer (Axis-Shield, Dundee, UK) showed an imprecision of 3.0% for within- run CV and 9.8% for between-run CV at 500 ng/mL of D-dimer, and 4.2% for within-run CV and 12.8% for between-run CV at 4,100 ng/mL of D-dimer. Although the between-run precision at low levels of D-dimer with SelexOn was higher than 10%, its high-level imprecision was better than that of the AxSYM D-dimer test. In addition, the SelexOn results for D-dimer showed a moderate correlation with STA-R results ( r=0.8379) (Fig. 2). However, the SelexOn findings were higher than STA-R around the reference value (500 ng/mL) (Fig. 3), which may explain the relatively low positive agreement (0.848) and kappa value (0.561) obtained. Similar results were observed when other D-dimer assays used in a previous study were used for comparisons [21].
The measurement of TSH is the most common test for the diagnosis and monitoring of thyroid diseases [22].
When compared with the Centaur XP tests, the SelexOn TSH tests showed a negative bias of 6.1% with good correlation ( r=0.9723), positive agreement (0.927), and kappa value (0.810). Thus, TSH testing by SelexOn may be useful for screening thyroid diseases.
In summary, SelexOn demonstrated relatively good analytical performance for AFP, CK-MB, D-dimer, hs- CRP, myoglobin, PSA, and TSH, despite some limitations.
Because of its rapid results, SelexOn may be helpful in
quick screening of patients for cardiovascular disease,
thyroid disease, prostate cancer, and hepatocellular
carcinoma.
REFERENCES
1. Gregory AH, Katherine IS. Point-of-care and physician office laboratories. In: Henry JB, McPherson RA, Pincus MR, editor. Henry’s clinical diagnosis and management by laboratory methods. 22nd ed. Philadelphia (PA):
Elsevier/Saunders, 2011: 87-93.
2. Nichols JH. Point of care testing. Clin Lab Med 2007;27:
893-908, viii.
3. Von Lode P. Point-of-care immunotesting: approaching the analytical performance of central laboratory methods.
Clin Biochem 2005;38:591-606.
4. Fraser CG. Optimal analytical performance for point of care testing. Clin Chim Acta 2001;307:37-43.
5. Clinical and Laboratory Standards Institute. Evaluation of precision performance of quantitative measurement methods: approved guideline-second edition. Wayne (PA): Clinical and Laboratory Standards Institute, 2004.
6. Clinical and Laboratory Standards Institute. Evaluation of the linearity of quantitative measurement procedure:
a statistical approach: approved guideline. Wayne (PA):
Clinical and Laboratory Standards Institute, 2003.
7. Clinical and Laboratory Standards Institute. Method comparison and bias estimation using patient samples:
approved guidelines. 2nd ed. Wayne (PA): Clinical and Laboratory Standards Institute, 2010.
8. Altman DG. Practical statistics for medical research.
Boca Raton (FL): Chapman and Hall, 1999.
9. Ricos C, Alvarez V, Cava F, Garcia-Lario JV, Hernandez A, Jimenez CV, et al. Current databases on biological variation: pros, cons and progress. Scand J Clin Lab Invest 1999;59:491-500.
10. Yang J, Chae H, Lee J, Kim Y, Kim SY, Lee HK, et al.
Evaluation of HUBI-QUANPRO point-of-care testing for cardiac markers. J Lab Med Qual Assur 2011;33:75-82.
11. Sturgeon CM, Duffy MJ, Hofmann BR, Lamerz R, Fritsche HA, Gaarenstroom K, et al. National Academy of Clinical Biochemistry Laboratory Medicine Practice Guidelines for use of tumor markers in liver, bladder, cervical, and gastric cancers. Clin Chem 2010;56:e1-48.
12. Sturgeon CM, Duffy MJ, Stenman UH, Lilja H, Brunner N, Chan DW, et al. National Academy of Clinical
Biochemistry laboratory medicine practice guidelines for use of tumor markers in testicular, prostate, colorectal, breast, and ovarian cancers. Clin Chem 2008;54:e11-79.
13. Lewandrowski K, Chen A, Januzzi J. Cardiac markers for myocardial infarction: a brief review. Am J Clin Pathol 2002;118 Suppl:S93-9.
14. Panteghini M, Pagani F, Yeo KT, Apple FS, Christenson RH, Dati F, et al. Evaluation of imprecision for cardiac troponin assays at low-range concentrations. Clin Chem 2004;50:327-32.
15. Ockene IS, Matthews CE, Rifai N, Ridker PM, Reed G, Stanek E. Variability and classification accuracy of serial high-sensitivity C-reactive protein measurements in healthy adults. Clin Chem 2001;47:444-50.
16. Ledue TB, Rifai N. Preanalytic and analytic sources of variations in C-reactive protein measurement:
implications for cardiovascular disease risk assessment.
Clin Chem 2003;49:1258-71.
17. Pearson TA, Mensah GA, Alexander RW, Anderson JL, Cannon RO 3rd, Criqui M, et al. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation 2003;107:499-511.
18. Roberts WL, Sedrick R, Moulton L, Spencer A, Rifai N. Evaluation of four automated high-sensitivity C-reactive protein methods: implications for clinical and epidemiological applications. Clin Chem 2000;46:461-8.
19. Di Nisio M, Squizzato A, Rutjes AW, Buller HR, Zwinderman AH, Bossuyt PM. Diagnostic accuracy of D-dimer test for exclusion of venous thromboembolism:
a systematic review. J Thromb Haemost 2007;5:296-304.
20. Sidelmann JJ, Gram J, Larsen A, Overgaard K, Jespersen J. Analytical and clinical validation of a new point-of-care testing system for determination of D-Dimer in human blood. Thromb Res 2010;126:524-30.
21. Elf JL, Strandberg K, Svensson PJ. Performance of two relatively new quantitative D-dimer assays (Innovance D-dimer and AxSYM D-dimer) for the exclusion of deep vein thrombosis. Thromb Res 2009;124:701-5.
22. Reix N, Massart C, d’Herbomez M, Gasser F, Heurtault
B, Agin A. Thyroid-stimulating hormone and free thyroxine on the ADVIA Centaur immunoassay system:
a multicenter assessment of analytical performance. Clin Biochem 2013;46:1305-8.
7종 바이오마커에 대한 셀렉스온 장비 성능 평가
김현영 • 이수연 • 박형두
성균관대학교 의과대학 삼성서울병원 진단검사의학과
배경: 새로 개발된 면역측정기 SelexOn (Infopia, Korea)은 전혈에서 α-fetoprotein (AFP), creatin kinase (CK)-MB, D-dimer, high-sensitivity C-reactive protein (hs-CRP), myoglobin, prostate specific antigen (PSA), thyroid-stimulating hormone (TSH) 등을 측정한다. 본 연구에 서는 SelexOn 장비의 분석적 검사수행능을 평가하였다.
방법: SelexOn 장비의 정밀도, 직선성을 평가하고 ADVIA Centaur XP Immunoassay (Siemens, Germany)와 STA-R coagulation analyzer (Diagnostica Stago, France) 장비와의 상관성 분석을 시행하였다.
결과: SelexOn 장비의 검사차례 내 변이계수는 모든 표지자에서 2.9-8.9%이었으며, 검사 간 변이 계수는 저농도의 D-dimer (16.1%)를 제외한 모든 표지자에서 1.6-11.3%이었다. 직선성 범위는 각각 AFP, 8.7-47.0 ng/mL; CK-MB, 4.7-38.7 ng/mL; D-dimer, 393.2-2,760.3 ng/mL;
hs-CRP, 2.1-9.0 mg/L; myoglobin, 67.2-441.5 ng/mL; PSA, 2.6-23.7 ng/mL; TSH 3.3- 38.9 mIU/L이었다. Centaur XP 및 STA-R 장비와의 비교분석에서 AFP, CK-MB, hs-CRP, PSA 는 상관계수가 0.975 이상으로 밀접한 상관관계를 보였으며; TSH, myoglobin, D-dimer의 상관계 수는 각각 0.9723, 0.9649, 0.8379이었다.
결론: SelexOn 장비는 정밀도, 직선성, Centaur XP 및 STA-R 장비와의 비교분석에서 만족할만한 검사 수행능을 보였다. 검사의 신속성과 적합한 분석능에 기반하여, SelexOn 장비는 심혈관질환, 갑 상선 질환, 전립선암 및 간암에 대한 선별검사로서 유용할 것으로 판단된다.
(J Lab Med Qual Assur 2014;36:30-38)
교신저자: 박형두
우)135-710 서울시 강남구 일원로 81, 성균관대학교 의과대학 삼성서울병원 진단검사의학과 Tel: 02)3410-0290 Fax: 02)3410-2719 E-mail: [email protected]