https://doi.org/10.14734/PN.2020.31.3.145 pISSN 2508-4887•eISSN 2508-4895
Ranhee Kim, MD1*, Seung Mi Lee, MD, PhD1*, Sohee Kim, MD1, Young Mi Jung, MD1, So Yeon Kim, MD1,
Chan-Wook Park, MD, PhD1, Joong Shin Park, MD, PhD1, Jong Kwan Jun, MD, PhD1,2
1Department of Obstetrics and Gynecology, 2The Institute of Reproductive Medicine and Population, Medical Research Center, Seoul National University College of Medicine, Seoul, Korea
*R. Kim and SM. Lee contributed equally as first authors of this study.
Intrafetal coagulation by a radiofrequency ablation (RFA) device has traditionally been used for selec
tive feticide in complicated monochorionic multiple pregnancies. However, as RFA is not feasible in early pregnancy, intrafetal laser coagulation has recently been suggested as an alternative method in the early midtrimester period. This study aimed to report our experience of utilizing intrafetal laser coagulation for selective feticide in early complicated monochorionic multiple pregnancies. Three monochorionic multiple pregnancies that were treated with intrafetal laser coagulation before 20 weeks were described.
Sonographic findings during pregnancy, antepartum course, and intrafetal laser coagulation procedure were reviewed, along with their perinatal outcomes. Indications were twin reversed arterial perfusion sequence in two cases, and dichorionic triamniotic triplets compli cated with twintotwin transfusion syndrome in one case. Intrafetal laser coagulation was successful in all three cases, with favorable neonatal outcomes.
Key Words: Multiple pregnancy, Complication, Fetoscopic surgical procedure, Laser ablation
Introduction
Monochorionic twin pregnancy occurs when a single fertilized ovum divides after the fourth post-fertilization day, and accounts for 13-14% of twin pregnancies.1 Monochorionic twin pregnancy is associated with high perinatal mortality and morbidity, especially due to vascular anastomosis in the shared placenta. Twin-to-twin transfusion syndrome (TTTS) is a unique complication of monochorionic twin pregnancy because of this vascular anastomosis, and has been a main area of study to improve perinatal outcomes. While advancements such as the development of fetoscopic laser coagulation treatment for vascular anastomosis have been promising, other complications such as twin reverse arterial perfusion (TRAP) sequence and TTTS cases with impending intrauterine compromise have not been heavily researched.
Traditionally, intrafetal radiofrequency ablation (RFA) has been the preferred method to treat vascular anastomosis in TRAP sequence and for selective feticide of a monochorionic twin.
However, its use in the earlier gestational period (i.e., before 16 weeks of gestation) is dis- couraged, because the device requires 14- to 17-gauge needles, which pose a higher risk of amniotic membrane rupture. Therefore, the median gestational age at the time of the proce- dure is 20 weeks.2 Consequently, intrafetal laser coagulation has been developed to allow for ablation at an earlier gestational age. In this report, we describe three cases of pregnancies treated with intrafetal laser coagulation before 20 weeks of gestation.
Case
Received: 19 April 2020 Revised: 11 May 2020 Accepted: 25 May 2020 Correspondence to Jong Kwan Jun, MD, PhD Department of Obstetrics and Gynecology, Seoul National University College of Medicine, 103 Daehakro, Jongnogu, Seoul 03080, Korea
Tel: +82220723744 Fax: +8227623599 E-mail: [email protected]
Copyright© 2020 by The Korean Society of Perinatology
This is an Open Access article distributed under the terms of the Creative Com
mons Attribution NonCommercial License (http://creativecommons.org/
license/bync/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any
Intrafetal Laser Treatment for Selective Feticide
in Monochorionic Multiple Pregnancies
evaluation of TRAP sequence. This pregnancy was achieved by in vitro fertilization. Sonographic evaluation at referral showed monochorionic diamniotic twins complicated by reverse flow in the umbilical artery of the acardiac twin, consistent with TRAP sequence (Fig. 1). The acardiac twin showed a single umbilical vein.
The phenotype of the acardiac twin was ‘acardius acephalus,’
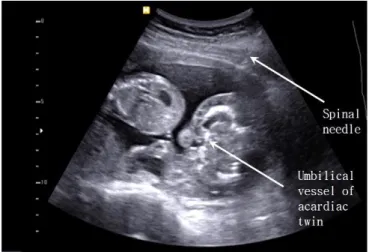
consisting of no cranial or thoracic structures and abnormal lower extremities. Doppler examination of the pump twin showed no end-diastolic flow, no reverse flow in the umbilical artery, and a positive ductus venosus a-wave. The parents were counseled regarding the antepartum course of the pump twin, including the risk of hemodynamic compromise due to the growing acardiac twin, with a perinatal death risk of 55%.3 We monitored the pump twin weekly to detect any sign of heart failure. As the ductus venosus a-wave disappeared at 14 weeks, several diffe rent management options were suggested to the parents, includ- ing observation and intervention to cease blood flow to the acardiac twin. After obtaining informed consent, intrafetal laser coagulation was performed at 16+3 weeks of gestation. Under ultrasonographic guidance, an 18-gauge spinal needle was placed near the acardiac twin’s intraabdominal umbilical vessels, and a laser fiber was inserted through the needle (Fig. 2). The laser power was set at 20 Watts. In addition to normal fetal movement and heartbeat of the pump twin, no blood flow to the acardiac twin was observed after the procedure (Fig. 3).
The subsequent prenatal course was uncomplicated. At 39+2
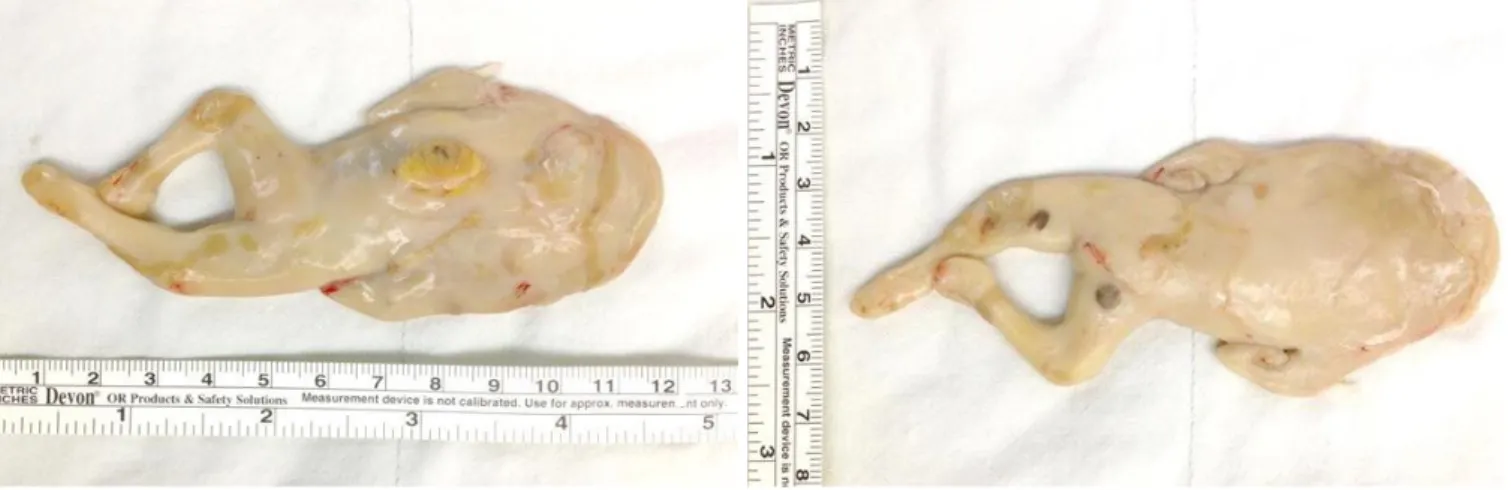
gestational weeks, the patient presented with labor pain and proceeded to deliver a healthy female weighing 2,800 g vagin- ally, with a 1/5 min Apgar score of 8/9. The acardiac twin was spontaneously removed with the placenta; its size was 9.9×4.2×
0.5 cm (Fig. 4). At one month postpartum follow up, she reported that the infant was in healthy state.
2. Case 2
A 26-year-old woman, gravida 1, para 0, was referred to our clinic due to sonographic abnormalities at 14+6 weeks of ges- tation, with the diagnosis of an acardiac twin first detected at 13+6 gestational weeks. The patient’s pregnancy was achieved naturally. Sonographic evaluation indicated a mass exhibiting an edematous trunk-like structure with lower extremities and re-
Fig. 1. Reverse flow in the umbilical artery of the acardiac twin. UA, umbilical artery.
Fig. 2. Intraprocedural image of intrafetal laser coagulation of the acardiac twin.
Fig. 3. Occlusion of the feeding vessel to the acardiac twin, leading to a lack of blood flow.
3. Case 3
A 34-year-old woman, gravida 1, para 0, was referred to our clinic due to a triplet pregnancy complicated by discordant growth at 18+2 weeks of gestation. According to her history, two fertilized embryos were transferred at the eight-cell stage.
Sonographic evaluation on referral day demonstrated dicho- rionic tri-amniotic triplets. The smaller fetus of monochorionic placentation had no visible bladder and the maximal vertical pocket (MVP) was 1.10 cm deep, consistent with oligohydram- nios (Fig. 7) and the other monochorionic fetus showed polyhy- dramnios (MVP=7.43 cm). Both fetuses showed normal Doppler profiles in the umbilical artery and ductus venosus. Therefore, we considered this pregnancy as impending TTTS. The patient was then admitted for fetal surveillance. The next day, a sono- graphic evaluation showed further increase in amniotic fluid (MVP=9.74 cm) in the larger monochorionic fetus. The parents were counseled regarding the antepartum course of TTTS and had several management options explained to them, including expectant management, selective fetal reduction, and fetoscopic laser ablation of anastomoses vessels. The patient chose to proceed with selective feticide of the smaller monochorionic fetus.
At 18+3 gestational weeks, intrafetal laser coagulation of the perivesical umbilical vessels of the smaller fetus was performed using an 18-gauge spinal needle under local anesthesia (Fig. 8).
After removal of the spinal needle, the umbilical vein flow of the sacrificed fetus was not detected, but an umbilical artery pulse of 40-50/min and fetal movement were still seen. There- fore, the procedure was repeated using the same method.
Due to potential uterine contractions after the procedure, rito- verse flow from the other fetus, consistent with TRAP sequence
(Fig. 5).
Intrafetal laser coagulation was conducted at 15+2 gestational weeks. The same procedure as the above cases was performed on the intraabdominal umbilical vessels of the acardiac fetus.
The procedure ended after no Doppler flow to the acardiac fetus was confirmed (Fig. 6). The patient was discharged the day after the procedure, and subsequent sonographic evaluation showed normal growth until 22+6 weeks of gestation. The patient was referred to the local obstetric clinic for routine antepartum ma- nagement. She delivered a 3,200 g full term baby vaginally without any complication. At one-year follow-up, the infant showed normal development without any neurologic deficit.
Fig. 5. Image of the acardiac twin with reverse flow from the pump twin.
Fig. 4. Acardiac twin delivered.
drine was administered for one day. Sonographic evaluation on the day after the procedure showed no cardiac activity of the sacrificed fetus. The patient was discharged on the second day after the procedure. Subsequent ultrasound examinations showed normal growth of the remaining fetuses. At 35+3 weeks of gestation, the patient was admitted due to premature preterm rupture of membranes. Labor was induced at 36+1 gestational weeks after expectancy management, and two healthy babies, one male and the other female, were delivered. The sacrificed fetus was delivered as well. The weights of the surviving babies were 2,595 g and 2,365 g, with 1/5 minute Apgar score of 7/7 and 8/9, respectively. The two surviving babies were discharged after routine neonatal care. At one year of age, the infants exhi- bited normal development without any neurologic deficit.
Fig. 8. Intraprocedural image of intrafetal laser coagulation of the donor twin.
Fig. 6. Intraprocedural and post-procedural images of intrafetal laser coagulation.
Fig. 7. No visible bladder and oligohydramnios features of the donor twin.
Discussion
In TRAP sequence, artery-to-artery anastomosis between pump twin and acardiac co-twin is developed through the shared placenta, with the pump twin supplying blood to the acardiac twin. If untreated, about 55% of pump twins in TRAP sequence experience unfavorable perinatal outcomes due to cardiac failure or polyhydramnios.3 In a pregnancy complicated with TTTS in the earlier gestational period or that with impending intrauterine compromise, which are not feasible for fetoscopic laser coagu- lation, selective feticide through occlusion of the umbilical vein or umbilical cord may be considered.
Several intervention techniques have been proposed to cease vascular anastomosis safely between the twins. These techniques include fetoscopic cord coagulation,4,5 fetoscopic cord ligation,6,7 fetoscopic photocoagulation of the anastomoses,8,9 intrafetal RFA,2,10,11 and intrafetal laser coagulation.12,13
In a study by Tan and Sepulveda14 comparing intrafetal abla- tion and cord occlusion in TRAP sequence, intrafetal ablation was considered as the best option because of its association with a lower failure rate and higher pump twin survival rate.
As targe ting the floating umbilical vessel within the umbilical cord is diffi cult, targeting of the intraabdominal umbilical vessel has been identified as a more successful method.15 Intrafetal ablation using an Nd:YAG laser (1,064 nm wavelength) is opti- mal due to its greater coagulation effect; the laser’s shorter diameter (400 µm, 18- to 20-gauge) compared with the RFA device (3 mm, 14-gauge) also allows the procedure to be per- formed in earlier gestational weeks.11,12 Moreover, the tech- ni ques required to perform intrafetal laser coagulation are relatively easier and widely usable, since the procedure re- quires similar training to amniocentesis using 18- and 20- gauge needles.16
The best time for intrafetal laser coagulation was previously considered after 16-18 weeks of gestation. This was recom- mended because the completion of coelomic cavity obliteration is associated with lower procedure-related complications, such as premature rupture of the membrane within two weeks post- procedure.17 Considering that earlier diagnosis of TRAP se- quence has become possible with increased ultrasonographic resolution, and the shorter interval between diagnosis and inter- vention improves prognosis, interruption of the blood supply
from the pump twin to the acardiac twin is recommended as soon as possible, once diagnosis has been established.17-20
The median age at the time of the procedure was 16+3 weeks (range: 15+2, 18+3). According to our results, intrafetal laser coagulation is feasible as early as 15 weeks with favorable neo- natal outcomes. Further study is required to conclude whether earlier invasive management is preferable to the conventional treatment period. For this purpose, the TRAP Intervention STudy (TRAPIST) trial has been ongoing since 2016. This multicen- ter randomized controlled trial was designed to compare the outcome of early intervention (12+0-14+0 weeks) (study group) with that of late intervention (16+0-19+0 weeks) (control group) among cases of TRAP sequence diagnosed between 12+0 and 13+6 weeks.
This case series is the first of its kind to report on intrafetal laser coagulation in Korea and shows a high success rate of the procedure. Since this report is composed of only three cases from one center, further studies are needed. The results of the TRAPIST trial are expected to indicate the best timing for in- trafetal laser coagulation. Intrafetal laser coagulation to treat TRAP sequence or selective feticide in TTTS showed favorable outcomes.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This work was supported by a grant 0320190410 from the Seoul National University Hospital research fund.
References
1) McNamara HC, Kane SC, Craig JM, Short RV, Umstad MP. A review of the mechanisms and evidence for typical and atypical twinning. Am J Obstet Gynecol 2016;214:172-91.
2) Lee H, Bebbington M, Crombleholme TM; North American Fetal Therapy Network. The North American Fetal Therapy Network Registry data on
outcomes of radiofrequency ablation for twin-reversed arterial perfusion sequence. Fetal Diagn Ther 2013;33:224-9.
3) Moore TR, Gale S, Benirschke K. Perinatal outcome of forty-nine preg- nancies complicated by acardiac twinning. Am J Obstet Gynecol 1990;
163:907-12.
4) Ville Y, Hyett JA, Vandenbussche F, Nicolaides KH. Endoscopic laser coa- gulation of umbilical cord vessels in twin reversed arterial perfusion sequence. Ultrasound Obstet Gynecol 1994;4:396-8.
5) Arias F, Sunderji S, Gimpelson R, Colton E. Treatment of acardiac twinning.
Obstet Gynecol 1998;91(5 Pt 2):818-21.
6) Quintero RA, Reich H, Puder KS, Bardicef M, Evans MI, Cotton DB, et al.
Brief report: umbilical-cord ligation of an acardiac twin by fetoscopy at 19 weeks of gestation. N Engl J Med 1994;330:469-71.
7) Deprest JA, Evrard VA, Schoubroeck D, Vandenberghe K. Endoscopic cord ligation in selective feticide. Lancet 1996;348:890-1.
8) Takano M, Murata S, Fujiwara M, Hirata H, Nakata M. Experience of feto- scopic laser photocoagulation and cord transection for twin‐reversed arterial perfusion sequence. J Obstet Gynaecol Res 2015;41:1326-9.
9) Hecher K, Lewi L, Gratacos E, Huber A, Ville Y, Deprest J. Twin reversed arterial perfusion: fetoscopic laser coagulation of placental anastomoses or the umbilical cord. Ultrasound Obstet Gynecol 2006;28:688-91.
10) Tsao K, Feldstein VA, Albanese CT, Sandberg PL, Lee H, Harrison MR, et al. Selective reduction of acardiac twin by radiofrequency ablation. Am J Obstet Gynecol 2002;187:635-40.
11) Lee MY, Won HS, Lee KA, Kyeong KS, Jeon EJ, Shim JY, et al. Perinatal outcome of twin reversed arterial perfusion sequence: a single center's experience. Korean J Obstet Gynecol 2012;55:552-8.
12) Jolly M, Taylor M, Rose G, Govender L, Fisk NM. Interstitial laser: a new
surgical technique for twin reversed arterial perfusion sequence in early pregnancy. BJOG 2001;108:1098-102.
13) Pagani G, D'Antonio F, Khalil A, Papageorghiou A, Bhide A, Thilaganathan B. Intrafetal laser treatment for twin reversed arterial perfusion sequence:
cohort study and meta‐analysis. Ultrasound Obstet Gynecol 2013;42:6- 14.
14) Tan TY, Sepulveda W. Acardiac twin: a systematic review of minimally invasive treatment modalities. Ultrasound Obstet Gynecol 2003;22:409- 19.
15) Sepulveda W, Bower S, Hassan J, Fisk NM. Ablation of acardiac twin by alcohol injection into the intra-abdominal umbilical artery. Obstet Gynecol 1995;86:680-1.
16) Chaveeva P, Poon LC, Sotiriadis A, Kosinski P, Nicolaides KH. Optimal method and timing of intrauterine intervention in twin reversed arterial perfusion sequence: case study and meta-analysis. Fetal Diagn Ther 2014;35:267-79.
17) Lewi L, Valencia C, Gonzalez E, Deprest J, Nicolaides KH. The outcome of twin reversed arterial perfusion sequence diagnosed in the first trime- ster. Am J Obstet Gynecol 2010;203:213.e1-4.
18) Berg C, Holst D, Mallmann MR, Gottschalk I, Gembruch U, Geipel A. Early vs late intervention in twin reversed arterial perfusion sequence. Ultra- sound Obstet Gynecol 2014;43:60-4.
19) Roethlisberger M, Strizek B, Gottschalk I, Mallmann M, Geipel A, Gem- bruch U, et al. First‐trimester intervention in twin reversed arterial perfu- sion sequence: does size matter? Ultrasound Obstet Gynecol 2017;50:
40-4.
20) Tavares de Sousa M, Glosemeyer P, Diemert A, Bamberg C, Hecher K.
First-trimester intervention in twin reversed arterial perfusion sequence.
Ultrasound Obstet Gynecol 2020;55:47-9.