-45-
KISEP Original Article J Rhinol 14(1), 2007
하기도 질환이 만성 비부비동염의 중증도에 미치는 영향
성균관대학교 의과대학 이비인후과학교실
소윤경·동헌종·김효열·정승규
The Effect of Lower Airway Disease on the Severity of Chronic Rhinosinusitis
Yoon Kyoung So, MD, Hun-Jong Dhong, MD, Hyo Yeol Kim, MD and Seung Kyu Chung, MD Department of Otorhinolaryngology-Head and Neck Surgery, Samsung Medical Center,
Sungkyunkwan University School of Medicine, Seoul, Korea
ABSTRACT
Background and Objectives:The relationship between the upper airway disease and the lower airway disease has been stu- died for several decades. In this study, we propose to investigate the prevalence of asthma, asymptomatic bronchial hyperrespon- siveness (aBHR) and small airway disease among the chronic rhinosinusitis (CRS) patients and to evaluate their influence on the severity of CRS. Material and Methods:For the evaluation of lower airway diseases, sixty-eight adult patients with CRS underwent skin prick tests, pulmonary function tests with or without bronchodilator tests and methacholine bronchial provoca- tion tests. The severity of CRS was determined in accordance to three factors;subjective symptoms, the degree of nasal polyposis and the extent of disease on the CT scan. Results:Asthma, aBHR and small airway disease were diagnosed among seven (10.3%), five (7.4%) and eleven (16.2%) patients, respectively. The lower airway diseases had no significant influence on the severity of CRS. Conclusion:CRS patients may have various lower airway diseases, symptomatic or asymptomatic, which should be considered when managing CRS patients.
KEY WORDS:Chronic rhinosinusitis·Lower airway disease·Asthma·Asymptomatic bronchial hyperresponsiveness·Small airway disease.
서 론
상기도 질환과 하기도 질환의 관련성은 지난 수십 년 간 연 구되어 왔으며, 최근에는 별개의 질환이 아닌 하나의 연관된 호흡기 질환(united airway disease)으로 인식되고 있다.1)2) 천식의 경우 약 50~70%에서 부비동염이 동반된다고 보고되 어 있다.3-5) 한편, 천식의 증상이 없이도, 기도의 염증과 경한 폐쇄가 있을 수 있는데 이를 무증상 기관지과민성(asymptoma- tic bronchial hyperresponsiveness)이라 한다.6) 무증상 기 관지과민성은 병리학적으로 천식보다는 약한 정도의 기도 염 증과 폐쇄로 인한 상태로서,6-9) 현재까지의 연구에 따르면 무 증상 기관지과민성 환자 중 14~58%가 수 년 내에 천식으
로 발전한다고 보고되어 있다.7-10) 또한 2~3 mm 이하의 소 기도에 염증과 폐쇄를 일컫는 소기도질환(small airway di- sease)은 만성폐쇄성폐질환 또는 천식의 전단계로 알려져 있
으며,11-16) 2004년 Ragab 등17)은 만성 비부비동염 환자의 36%
에서 소기도 질환이 동반되었다고 보고하였다. 이에 본 연구 에서는 만성 비부비동염 환자를 대상으로, 객관적인 검사 방 법을 이용하여 천식과 무증상 기도과민성, 소기도 질환이 만 성 비부비동염의 중증도에 영향을 미치는지 알아보고자 하 였다.
재료 및 방법
2005년 4월부터 2006년 1월까지 삼성서울병원 이비인후 과를 방문한 68명의 만성 비부비동염 환자를 대상으로 하였 다. 이 중 26명이 여성이었고 42명이 남성이었으며, 연령은 14세에서 74세로 평균연령은 44세였다. 본 연구는 임상시험 심사위원회(Institutional review board)의 승인을 받았으며, 논문접수일:2006년 10월 20일 / 심사완료일:2007년 1월 5일
교신저자:동헌종, 135-710 서울 강남구 일원동 50 성균관대학교 의과대학 이비인후과학교실
전화:(02) 3410-3579·전송:(02) 3410-3879 E-mail:[email protected]
46 / J Rhinol 14(1), 2007
연구에 대한 충분한 설명 후 동의한 환자들만을 대상으로 하 였다.
초진시, 문진과 비내시경 검사를 시행하였으며, Rhinosi- nusitis Task Force의 진단기준18)에 따라, 농성비루 등 비부 비동염의 증상이 3개월 이상 지속되며, 비내시경 검사상 비 용종, 농성 분비물 등 특징적 소견이 관찰되는 경우에 만성 비부비동염으로 진단하였다. 일측성 부비동염, 후비공용종, 낭 포성 섬유증(cystic fibrosis), 원발섬모운동이상증(primary ciliary dyskinesia), 면역결핍증(immunodeficiency) 등이 있 는 환자는 제외되었다. 관련요인이 될 수 있는 알레르기비염 에 대하여는 모든 환자를 대상으로 피부단자시험(skin prick test)을 시행하여 알레르기비염 동반여부를 평가하였고, 흡연 력, 알레르기 또는 천식의 가족력을 조사하였다.
만성 비부비동염의 중증도는 증상, 비내시경 소견, 컴퓨터 단층촬영(CT) 소견의 세 측면에서 평가하였다. 먼저 증상의 중증도는 비폐쇄감, 농성 비루, 후비루, 안면통, 안면충만감 (facial fullness), 후각장애의 만성 비부비동염 주증상 6가지 에 대하여 0점에서 7점까지 환자가 직접 평가하였다(Table 1).
비내시경 검사상 용종의 정도는 이비인후과 의사가 평가하였 으며, 용종이 없는 경우를 0점, 중비도내에 국한된 경우를 1 점, 중비도를 넘어 비강으로 확장된 경우를 2점으로 하였으 며, 양쪽의 점수를 합하여 0점을 1기(stage 1), 1~2점을 2기 (stage 2), 3~4점을 3기(stage 3)로 하였다. CT 소견은 Lund- Mackay scoring system19)에 따라 평가하여, 0~6점을 1기 (stage 1), 7~12점을 2기(stage 2), 13~18점을 3기(stage 3), 19~24점을 4기(stage 4)로 하였다.
한편, 모든 환자를 대상으로 내과의가 호흡곤란, 천명, 기 침, 객담 등에 대한 문진과 신체검사를 시행하였으며, 모든 환자에게 폐기능 검사(pulmonary function test, PFT)를 시 행하였다. 현재 천식 증상이 있거나, 폐기능 검사상 중등도 이상의 기도폐쇄 소견을 보이는 2명에 대해서는 기관지 확장 제 반응검사(bronchodilator test, BDT)를 시행하였으며, 나 머지 66명의 환자에 대해서는 메타콜린 기관지 유발검사(Me-
thacholine bronchial provocation test, MBPT)를 시행하였 다. BDT의 경우 기관제 확장제인 salbutamol 흡입 후 측정 한 1초 노력성 호기량(forced expiratory volume in 1 second, FEV1)이 200 ml 이상 또는 기저치의 12% 이상 증가한 경 우를 양성으로,20) MBPT의 경우 메타콜린 흡입 후 FEV1이 기 저치의 20%만큼 감소할 때의 메타콜린의 농도(PC20)를 측정 하여, PC20가 25 mg/ml 이하인 경우를 양성으로 하였다.21)
호흡곤란, 천명 등 임상 증상의 병력이 있으면서 MBPT 또 는 BDT에서 양성인 경우 천식으로 진단하였으며,22) 임상 증 상이 없는 경우 무증상 기관지과민성으로 진단하였다.6) 다른 호흡기 질환이 없으면서 폐기능 검사에서 FEV1은 정상이고 노력성 호기중간 기류량(forced expiratory flow from 25% to 75% of lung volume, FEF 25~75%)만이 정상 범위 하한값 의 80% 미만으로 감소한 경우를 소기도 질환으로 하였다.23)
각 하기도 질환 군 간의 만성 비부비동염의 중증도 비교는 Kruskal-Wallis test를 이용하였으며, 각 군의 연령분포 비 교는 One-way ANOVA, 성별분포 및 알레르기비염의 동반율 비교에 대해서는 Chi-square test를 이용하였다. SPSS를 이 용하였으며, 모든 경우에서 유의수준은 p<0.05로 하였다.
결 과
68명의 환자 중, 천식 환자가 7명(10.3%), 무증상 기관지 과민성 환자가 5명(7.4%), 소기도 질환이 동반된 환자가 11명 (16.2%)이었다.
전체환자 68명을 하기도 질환이 동반되지 않은 45명의 환 자 군과, 천식이 동반된 환자 군, 무증상 기관지과민성이 동 반된 환자 군, 소기도 질환이 동반된 환자 군의 네 군으로 나 누어 연령 및 성별, 알레르기 비염의 동반 여부 등 관련요인 을 비교하여 보았을 때 유의한 차이는 없었다(p>0.05, Table 2).
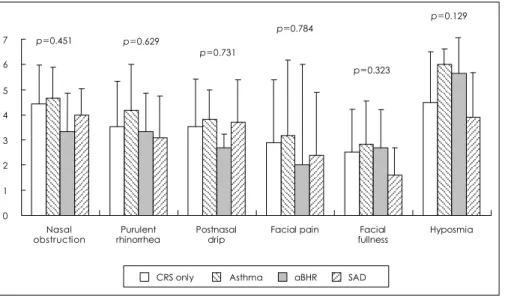
또한 네 군의 만성 비부비동염의 중증도를 비교하였을 때, 증 상의 중증도, 비내시경 검사상 비용종의 정도, Lund-Mackay
Tabe 1. Questionnaire on symptoms of CRS 증상의 정도 1 이런 증상이 없다
2 1과 3사이의 증상이다
3 약하게 지속적으로 있으나, 쉽게 참을 만하다 4 3과 5사이의 증상이다
5 상당히 불편하고 참기 어렵다, 일상생활이나 수면에 방해를 받는 경우도 있다
6 5와 7사이의 증상이다
7 증상이 심하여 신체적으로 고통이 크고 일을 못 할 정도이다
Table 2. Associating factors
CRS only Asthma aBHR SAD p value
Age (mean) 420. 410. 45 530. 0.193
M:F 26:19 4:3 3:2 9:2 0.523
Allergic rhinitis (%) 20.4 33.3 20 18.2 0.895 FHx of asthma (%) 11.1 42.9 00 09.1 0.282 FHx of allergy (%) 200. 42.9 00 27.2 0.617
Smoking (%) 25.6 28.6 00 36.4 0.492
There was no significant difference in associating factors among four patients’ groups. CRS:chronic rhinosinutis, aBHR:asymp- tomatic bronchial hyperresponsiveness, SAD:small airway di- sease, FHx:family history
소윤경 등:만성 부비동염과 하기도 질환 / 47
score 등 세 측면 모두에서 유의한 차이는 없었다(p>0.05, Fig. 1, 2).
고 찰
2001년 Kim 등24)이 서울에 거주하는 성인 718명을 대상으 로 본 연구와 같은 방법을 이용하여 조사한 바에 따르면 한 국 성인에서 천식과 무증상 기관지과민성의 유병율은 각각 3.4%, 3.8%였다. 본 연구의 결과 만성 비부비동염 환자에서 천식의 유병율은 10.3%, 무증상 기관지과민성의 유병율은 7.4%
로, 만성 비부비동염 환자에서 천식 및 무증상 기관지과민성 의 유병율이 높은 것을 알 수 있었다. 소기도 질환도 본 연 구에서 16.2%의 높은 유병율을 보였다.
본 연구의 결과 천식, 무증상 기관지과민성, 소기도 질환이 동반되더라도 만성 비부비동염의 중증도에는 영향이 없는 것
으로 나타났다. 하지만 천식의 경우 이에 대해서는 현재까지 논란의 여지가 있다. Dejima,25) Dinis26) 등은 만성 비부비동 염 환자를 대상으로 천식군과 비천식군 사이에 비용종(poly- posis)및 CT상 질환의 범위에 있어 유의한 차이가 없는 것 으로 보고 한 반면, Newman,27) Bresciani28) 등 여러 연구자 들은 천식이 동반된 경우 CT상 비부비동염의 중증도가 증 가하는 것으로 보고하였다. 물론 본 연구를 비롯하여 여러 연 구들에서 대상 환자의 수가 적었으므로 아직 결론을 얻기는 힘들다. 또한 잘 조절되고(well-managed) 있는 천식 환자를 대상으로 하느냐, 조절되지 않는 중증의 천식 환자를 대상으 로 하느냐에 따라서도 결과가 달라질 수 있다. 본 연구에서 는 천식 환자군 7명 중 6명이 이미 약으로 잘 조절되고 있었 으며 연구 당시에 천식의 증상이 없었기 때문에 결과에 어느 정도 영향을 주었을 수 있다.
하지만 다른 각도로 생각해보면, 일반적으로 비부비동염이 심한 경우에만 천식 등 하기도 질환의 동반 여부를 고려하게 되는데, 본 연구에 따르면 만성 비부비동염의 중증도와 상관 없이 하기도 질환이 동반될 수 있다는 것을 알 수 있다. 이 는 만성 비부비동염 환자 진료 시, 특히 부비동 내시경 수술 전에 반드시 고려되어야 할 것이다. 또한, 앞서 고찰해 본 바 와 같이 추후 대규모 환자군을 대상으로 한 연구도 필요할 것 이고, 천식 및 하기도 질환의 중증도와 만성 비부비동염의 중 증도의 관련성에 대한 연구, 그리고 하기도 질환이 만성 비 부비동염의 수술 후 예후에 미치는 영향에 대한 연구 등이 필 요할 것으로 생각된다.
결 론
본 연구의 결과 하기도 질환이 동반되더라도 비부비동염의
0 1 2 3 4 5 6 7
Nasal
obstruction Purulent
rhinorrhea Postnasal
drip Facial pain Facial
fullness Hyposmia
CRS only Asthma aBHR SAD
p=0.451 p=0.629
p=0.731
p=0.784
p=0.323
p=0.129
Fig. 1. Symptom scores. There was no significant difference in symptom sco- res of CRS among four patients’ groups.
CRS:chronic rhinosinutis, aBHR:asymp- tomatic bronchial hyperresponsiveness, SAD:small airway disease.
0 1 2 3 4
Polyp score CT score
CRS only Asthma aBHR SAD
p=0.903
p=0.192
Fig. 2. Degree of polyposis and extent of disease on CT scan.
There was no significant difference in extent of CRS among four patients’ groups. CRS:chronic rhinosinutis, aBHR:asymptoma- tic bronchial hyperresponsiveness, SAD:small airway disease.
48 / J Rhinol 14(1), 2007
중증도에는 영향이 없었다. 따라서 만성 비부비동염의 중증 도가 낮은 경우에도 하기도 질환이 동반될 수 있고, 이는 만 성 비부비동염 환자 진료 시 반드시 고려되어야 하며, 추후 좀더 심도 있는 연구가 필요할 것으로 생각된다.
중심 단어:만성비부비동염·하기도질환·천식·무증상 기 관지과민증·소기도질환.
REFERENCES
1) de Benedictis FM, del Giudice MM, Severini S, Bonifazi F. Rhini- tis, sinusitis and asthma: one linked airway disease. Paediatr Respir Rev 2001;2:358-64.
2) Passalacqua G, Ciprandi G, Canonica GW. The nose-lung interac- tion in allergic rhinitis and asthma: united airways disease. Curr Opin Allergy Clin Immunol 2001;1:7-13.
3) Tosca MA, Riccio AM, Marseglia GL, Caligo G, Pallestrini E, Ameli F, et al. Nasal endoscopy in asthmatic children: assessment of rhi- nosinusitis and adenoiditis incidence, correlations with cytology and microbiology. Clin Exp Allergy 2001;31:609-15.
4) Bresciani M, Paradis L, Des Roches A, Vernhet H, Vachier I, Godard P, et al. Rhinosinusitis in severe asthma. J Allergy Clin Immunol 2001;107:73-80.
5) Pfister R, Lutolf M, Schapowal A, Glatte B, Schmitz M, Menz G.
Screening for sinus disease in patients with asthma: a computed tomography-controlled comparison of A-mode ultrasonography and standard radiography. J Allergy Clin Immunol 1994;94:804-9.
6) Boulet LP. Asymptomatic airway hyperresponsiveness: a curiosity or an opportunity to prevent asthma? Am J Respir Crit Care Med 2003;
167:371-8.
7) Laprise C, Boulet LP. Asymptomatic airway hyperresponsiveness: a three-year follow-up. Am J Respir Crit Care Med 1997;156:403-9.
8) Laprise C, Laviolette M, Boutet M, Boulet LP. Asymptomatic airway hyperresponsiveness: relationships with airway inflammation and remodelling. Eur Respir J 1999;14:63-73.
9) Porsbjerg C, von Linstow ML, Ulrik CS, Nepper-Christensen SC, Backer V. Outcome in adulthood of asymptomatic airway hyperres- ponsiveness to histamine and exercise-induced bronchospasm in childhood. Ann Allergy Asthma Immunol 2005;95:137-42.
10) Zhong NS, Chen RC, Yang MO, Wu ZY, Zheng JP, Li YF. Is asymptomatic bronchial hyperresponsiveness an indication of poten- tial asthma? A two-year follow-up of young students with bronchial hyperresponsiveness. Chest 1992;102:1104-9.
11) Cosio MG, Hale KA, Niewoehner DE. Morphologic and morphometric effects of prolonged cigarette smoking on the small airways. Am Rev Respir Dis 1980;122:265-21.
12) Cosio Piqueras MG, Cosio MG. Disease of the airways in chronic obstructive pulmonary disease. Eur Respir J Suppl 2001;34:41s-9s.
13) Hale KA, Ewing SL, Gosnell BA, Niewoehner DE. Lung disease in long-term cigarette smokers with and without chronic air-flow obstruc- tion. Am Rev Respir Dis 1984;130:716-21.
14) Hamid Q, Song Y, Kotsimbos TC, Minshall E, Bai TR, Hegele RG, et al. Inflammation of small airways in asthma. J Allergy Clin Im- munol 1997;100:44-51.
15) Tulic MK, Christodoulopoulos P, Hamid Q. Small airway inflam- mation in asthma. Respir Res 2001;2:333-9.
16) Yanai M, Sekizawa K, Ohrui T, Sasaki H, Takishima T. Site of airway obstruction in pulmonary disease: direct measurement of intrabronchial pressure. J Appl Physiol 1992;72:1016-23.
17) Ragab A, Clement P, Vincken W. Objective assessment of lower air- way involvement in chronic rhinosinusitis. Am J Rhinol 2004;18:
15-21.
18) Lanza DC, Kennedy DW. Adult rhinosinusitis defined. Otolaryngol Head Neck Surg 1997;117:S1-7.
19) Lund VJ, Kennedy DW. Staging for rhinosinusitis. Otolaryngol Head Neck Surg 1997;117:S35-40.
20) Lung function testing: selection of reference values and interpretative strategies. American Thoracic Society. Am Rev Respir Dis 1991;144:
1202-18.
21) Crapo RO, Casaburi R, Coates AL, Enright PL, Hankinson JL, Irvin CG, et al. Guidelines for methacholine and exercise challenge testing-1999. This official statement of the American Thoracic So- ciety was adopted by the ATS Board of Directors, July 1999. Am J Respir Crit Care Med 2000;161:309-29.
22) Guidelines for the diagnosis and management of asthma. National Heart, Lung, and Blood Institute. National Asthma Education Program.
Expert Panel Report. J Allergy Clin Immunol 1991;88:425-534.
23) McFadden ER Jr, Linden DA. A reduction in maximum mid-expira- tory flow rate. A spirographic manifestation of small airway disease.
Am J Med 1972;52:725-37.
24) Kim SH. Prevalence of adult asthma based on questionnaires and methacholine bronchial provocation test in Seoul. J Asthma Allergy Clin Immunol 2001;21:618-27.
25) Dejima K, Hama T, Miyazaki M, Yasuda S, Fukushima K, Oshima A, et al. A clinical study of endoscopic sinus surgery for sinusitis in patients with bronchial asthma. Int Arch Allergy Immunol 2005;
138:97-104.
26) Dinis PB, Gomes A. Sinusitis and asthma: how do they interrelate in sinus surgery? Am J Rhinol 1997;11:421-8.
27) Newman LJ, Platts-Mills TA, Phillips CD, Hazen KC, Gross CW.
Chronic sinusitis. Relationship of computed tomographic findings to allergy, asthma, and eosinophilia. JAMA 1994;271:363-7.
28) Nishioka GJ, Cook PR, Davis WE, McKinsey JP. Functional endo- scopic sinus surgery in patients with chronic sinusitis and asthma.
Otolaryngol Head Neck Surg 1994;110:494-500.