Ⅰ. INTRODUCTION
The odontogenic myxomafibroma(odontogenic myxoma) of the jaws is a benign, usually slow-growing infiltrative tumor of connectice tissue.
1)According to a recent review article, prevalence of this entity shows 1:1.4 male/female ratio, the average age is 29.5 years. The most frequent location is the mandible.
2)Smaller lesions may be asymptomatic and larger lesions are often associated with a painless expansion of the involved bone. Facial deformity rarely reported with involvement of maxillary sinus.4) Pathogenesis of myxofibroma is unknown.
Radiographically, the myxofibroma appears as a unilocular or multilocular radiolucency that may displace or cause resorption of teeth in the areea of the tumor. The margins of the radiolucency are often irregular or scalloped. The radiolucent defect may contain thin, wispy trabecular of residual bone.
5)Histologically, these are characterized by presence of stellate and spindle-shaped cells embedded in an abundant
Korean Journal of Oral and Maxillofacial Pathology 2019;43(6):269-273 ISSN:1225-1577(Print); 2384-0900(Online) Available online at http://journal.kaomp.org https://doi.org/10.17779/KAOMP.2019.43.6.003
* Correspondence: Sang-Hun Shin, Department of Oral and Maxillofacial Surgery, School of Dentistry, Pusan National University, 49 Busandaehak- ro, Mulgeum-eup, Yangsan 50612, Korea
Tel: +82-55-360-5100, Fax: +82-55-360-5104 E-mail: [email protected]
ORCID: 0000-0002-0467-6206
상악에 재발한 거대한 치성 점액섬유종 : 증례 보고
이준상, 신상훈*, 전민아
부산대학교 치의학전문대학원 구강악안면외과학 교실
<Abstract>
A Giant Odontogenic Myxofibroma Recurred in Maxilla : A Case Report
Jun-Sang Lee, Sang-Hun Shin
*, Min-A Jeon
Department of Oral and Maxillofacial Surgery, School of Dentistry, Pusan National University, 49 Busandaehak-ro, Mulgeum-eup, Yangsan 50612, Korea
The myxoma(odontogenic myxoma, myxofibroma) of the jaws is a benign, usually slow-growing infiltrative tumor of connectice tissue.
This article describes a case history of the treatment of recurred odontogenic myxofibroma in the maxilla and further discusses the appropriate management of such cases with reference to the literature review. A 55-year-old male patient presented with a gingival swelling in the right side of maxilla. He had history of second time recurred disease. Microscopically, a high cellularity fibrous tumor with fibroblastic cells was observed. Tumor cells were composed of stellate and spindle shaped fibroblasts. Islands of odontogenic epithelium were seen in the specimen. The final diagnosis was made with odontogenic myxofibroma in consideration of twice-time recurrences and histological characteristics. Because of the high likelihood of recurrence, an accurate differential diagnosis of pathology at the time of initial visit is very important in determining treatment options, and immunohistochemical tests may be helpful. Also close following up is required.(155 words)
Key words : Odontogenic Myxoma, Odontogenic Myxofibroma, Recurrence, Surgical management
myxoid or mucoid extracellular matrix.
6)Trabeculae of woven bone and capillaries, islands of odontogenic epithelium and mast cells are also seen dispersed within the lesion.
2)This article describes a case history of the treatment of recurred odontogenic myxofibroma in the maxilla and further discusses the appropriate management of such cases with reference to the literature review.
Ⅱ. Patients and methods
A 55-year-old male patient presented with a gingival swelling in the right side of maxilla.(Fig. 1,2) He had no underlying disease. In 1982, he underwent excision of a benign mass which expanded after a car accident in the other university hospital. In 1992, re-operation was performed due to recurrence of the lesion. Unfortunately, histological diagnosis and medical records are no longer preserved at this time.
Clinical findings showed swelling on his right side of face causing facial deformity. Intraorally, palatal and buccal expansion of the right maxilla was shown.
Radiologically, a 65mm oval shaped large mass with fracture pattern of hard palate and maxillary sinus wall was
observed.(Fig. 3,4,5) A number of small radiopaque lesions were suspected as calcification or bony remnant within the lesion. We performed preoperative incisional biopsy to confirm malignancy and establish a surgical plan, and as a result, it was diagnosed as fibroma.
For complete removal of the lesion, Weber-Furguson approach was performed and the suspicious malignancy of the destructive bone boundary was confirmed through frozen biopsy during the operation. Frozen biopsy showed no evidence of malignant lesions, pre-fabricated resin stent to prevent facial deformity was applied.
Microscopically, a tumor mass was observed beneath stratified squamous epithelium without bony tissue, supporting the radiographic findings of bony destruction by odontogenic myxofibroma (a). The tumor consisted of randomly oriented stellate or spindle-shaped cells, and the cells were dispsersed in abundant myoxid stroma that contains fine collagen fibers (b). The final diagnosis was made with odontogenic myxofibroma in consideration of twice-time recurrences and histological characteristics.
Currently, the patient is well healed, and is undergoing prosthetic treatment under close observation.
(a) Extraoral feature (b) Intraoral feature
Fig. 1. Pre-operative features.
Intraoral feature. A giant gingival swelling in the Right side of maxilla. The patient showed swelling on the right maxilla
causing some facial asymmetry.
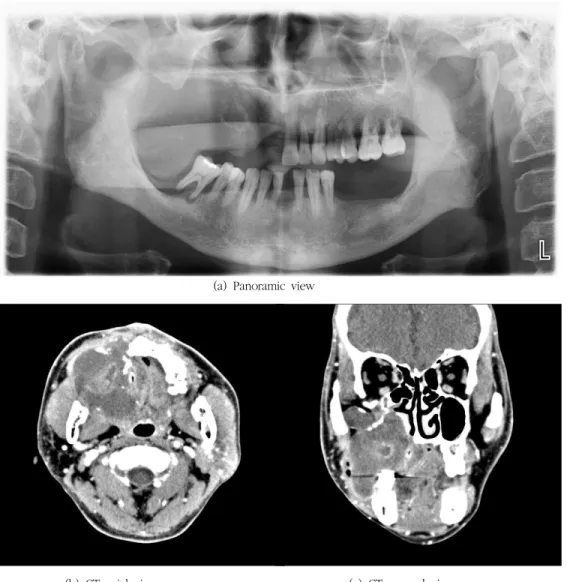
(a) Panoramic view
(b) CT axial view (c) CT coronal view
Fig. 2. Radiographic features. Panoramic image shows a mixed radiolucent radiopaque lesion with partially ill-defined borders in the right maxilla. A 65mm oval shaped large mass with fracture pattern of hard palate and maxillary sinus wall was observed.
A number of small radiopaque lesions were suspected as calcification or bony remnant within the lesion.
(a) (b)
Fig. 3. (a) Tumor after excision. Firm lesion of 60mm was excised. (b) Cross-section of tumor.
Ⅲ. Results and discussion
Odontogenic myxofibroma is a rare form of tumor that is histologically benign but has the nature of infiltrating and destroying adjacent bones and tissues.
1)Conventional radiological examinations have limitations in differential diagnosis, whereas CT and MRI can detect the tendency of tumor invasion toward adjacent tissues. These findings can differentiate myxoma from other benign tumors.
The use of CR, CT, and MRI should be routine in the diagnosis of odontogenic myxoma.
3)Histologically, this lesion is characterized by spindle-shaped cells with branching processes lying loosely in an abundany background of acid mucopolysaccharide. Islands of inactive odontogenic epithelium may be observed on occasion.
4)Immunofluorescence responds to vimentin, which clearly demonstrates that the lesion is a mesenchymal-derived tumor.
4)The recurrence rate of myxofibroma is reported to be higher than that of other benign tumors. The highest recurrence rate is 33% with the average recurrence rate of 25%
4), and a
recent review paper reports a 9.52% to 13% recurrence rate.
2),5)Eman Kheir et al. radiologically reported distinctive patterns of growth of the tumors were observed in all cases on MRI and CT, and appeared as lobulations, budding, and crevice formation. And they assumed that these parts of the tumors may account for high recurrence rate associated with odontogenic myxofibroma.
3)Also, recurrence is associated to local invasion into cansellous bone beyound radiographically visible margins in absence of tumor encapsulation.
2)Odontogenic myxoma is a benign tumors and it does not show mitotic activity patterns and high proliferation in histological features.
7)Thus, the huge growth of odontogenic myxoma in this case is thought to be due to the production of mucous substance in the tumor. Irritation from repeated surgery may affect tumor growth. Surgical removal of adjacent bone may promote growth of remnant tumor, similar to that of maxillary sinus lesions.
Various treatment options such as radical resection, excision, enucleation are introduced.
8)In a recent systemic review, a review of the average 10-year follow-up patients showed no significant difference between conservative excision and resection in recurrence rates and they argued that conservative treatment should be a priority given the morbidity and quality of life of patients.
5)However, they also emphasized that the maxillary lesions have more space spread before they are clinically clearly spread, which makes optimal treatment difficult and contributes to the rate of recurrence.
5)Considering the high probability of recurrence of the lesion in the maxillary sinus, as in this case, radical resection surgery considering the safety margin would be appropriate as a treatment method.
Due to the simultaneous consideration of high recurrence rates, morbidity due to surgery and the quality of life of the patient, an accurate differential diagnosis of pathology at the time of initial visit is very important in determining treatment options, and immunohistochemical tests may be helpful.
Also close following up is required.
(a) (H and E, x40) (b) (H and E, x200)