서 론
인공 고관절 재 치환술의 목적은 손상된 골조직을 재건하여 인공관절의 안정성을 얻고, 고관절의 역학 을 재수복 함과 동시에 하지 길이 차이를 정상화하 는데 있다. 고관절 재 치환술시 손상된 골조직을 재 건하는데 쓰이는 골조직은 자가골(autograft), 동 종골(allograft), 또는 골 대체물 (bone substi- tute) 등을 사용할 수 있으며 이중 자가골 이식의 결과가 가장 양호하다. 그러나 골 결손의 정도가 심 하면 자가골 이식만으로는 골 결손을 충당할 수 없 어 저장된 동종골을 사용할 수 밖에 없다. 고관절 재 치환술시 사용하는 동종골의 형태는 이식골의 형태 에 따라 크게 나누어 구조적 동종골(structural allograft, bulk allograft) 과 분쇄성 동종골 (morselized allograft, cancellous allograft) 로 구분되며 일반적으로 구조적(structural) 또는 비 공동형(uncontained) 골 결손의 경우에는 구조 적 동종골을 사용하고, 비구조적(non-structural) 또는 동공형(cavitary) 골 결손의 경우에는 분쇄성 골 이식을 사용한다. 인공관절 재 치환술시 동종골 을 사용하면 적용성(availability)이 뛰어나고 이 식골 채취부에 후유증을 남기지 않는다는 장점이 있 지만 면역반응이 나타날 수 있고, osteogenic cell
이나 osteoinductive factor 가 없으며, 질병을 전 염시킬 수 있는 가능성, 이식골의 골절 등의 문제점 이 있으므로 이에 대한 충분한 사전 지식을 가지고 시술하여야 한다. 일반적으로 인공고관절 재치환술 에 사용하는 동종골은 채취 후 2.5 Mrad 의 방사선 조사 후 영하 80도정도에서 냉동 보관된 동종골을 주로 사용하며, 이식하고자 하는 골 결손의 크기, 골 결손 부위, 이식수혜부의 상태, 그리고 골 결손이 구 조적인지 아니면 비구조적인지에 따라 이식골의 형 태를 달리하여 시술하여야 한다. 저자들은 인공 고 관절 재 치환술에 사용하는 동종골 이식술의 적응증 과 역할 및 여러 가지 다양한 동종골 이식술의 방법 들을 소개하고 문헌 고찰을 통하여 그 치료결과를 요약하고자 한다.
비구측 재 치환술시 동종골 이식술
1. 수술 전 처치(Preoperative management)
비구측 골 결손은 일반적으로 인공관절 치환술시 골 제거, 인공관절 부품에 의한 골 결손, 골 용해 (osteolysis), 방패 현상(stress-shielding), 그 리고 파손된 인공관절 부품의 제거시에 골 결손이 발생한다. 이러한 골 결손의 정확한 평가를 위해서
인공 고관절 재 치환술시 동종골 이식술
계명대학교 의과대학 정형외과학교실
민병우∙이경재
� Address for Correspondence : Byung-Woo Min, M.D.
Department of Orthopaedic Surgery College of Medicine Keimyung University, 194, Dong san dong, Joongu, Daegu, Korea
Tel : 82-53-250-7267, Fax : 82-53-250-7205, E-mail : [email protected]
수술 전 정면 및 사면 방사선 촬영과53)더불어 경우 에 따라 컴퓨터 단층 촬영을6)하여 보면 많은 도움 이 된다. 골 결손의 형태는 segmental or cavi- tary, structural or non-structural, con- tained or uncontained defect로 구분하고 심한 경우 완전한 골반 분리(pelvic discontinuity) 가 없는지 살펴 보아야 한다. 골 결손의 분류는 AAOS 분류7), 또는 Paprosky의 분류40)가 많이 쓰인다.
2. 분쇄성 동종골 이식(Morselized allograft)
분쇄성 동종골 이식은 재 치환술시 가장 선호되는 방법으로 골 전도기능(osteoconductive poten- tial)이 강한 반면 골 유도 기능(osteoinductive potential)은 미미하다. 동물 실험 및 사체검사결과 이식골의 재 혈관화(revascularization) 및 재형 성과정을 거쳐 새로운 골 소주를 잘 형성하는 것으 로 알려져 있다15).
1) 비구컵 교체 없이 골 결손부에 분쇄성 동종골 을 이식하는 방법(Morselized allograft with reten- tion of cup)
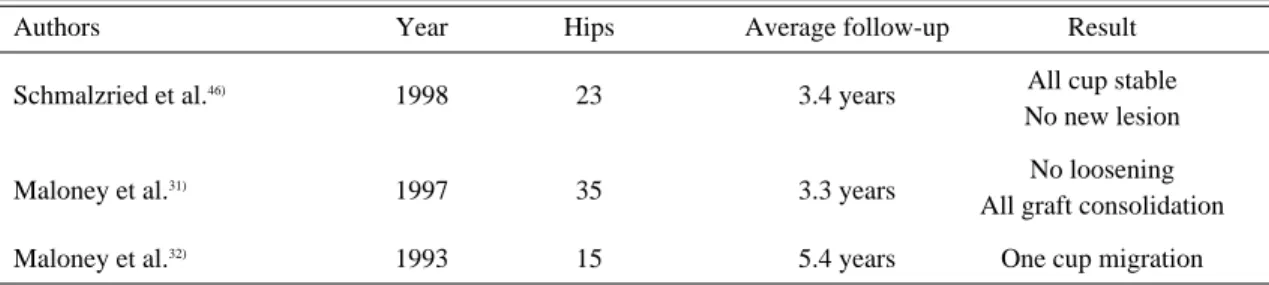
비구컵이 골성 고정되어 있고 폴리에틸렌 라이너 의 잠금 장치가 손상이 없으며, 교환 가능한 폴리에틸 렌 라이너가 있을 경우 비구컵 측면부나 비구컵의 screw hole 을 통해 pseudomembrane 및 골용해 부를 충분히 소파한 후 분쇄성 이식골을 충분히 감입 (impaction) 이식하고 폴리에틸렌 라이너만 교환하 면 좋은 치료효과를 기대할 수 있다. 일반적으로 2~5 년간의 단기 추시결과는 높은 성공율이 보고 되고 있 으나 장기 추시결과는 아직 보고가 없다 (Table 1).
2) 비구컵 교체 및 골 결손부에 분쇄성 동종골을 이식하는 방법 (Morselized allograft with cement- less cup revision)
제 1형 및 제 2형 비구골 결손시 비구컵 교체와 함 께 분쇄성 골 이식을 하는 방법으로 주로 젊은 연령 층에 사용 하는 방법이며 수술 시 반드시 비구컵의 50~70%가 숙주골 (host bone)에 접촉하도록 하 여야 한다. 중장기 추시결과상 실패율은 1~9%로서 비교적 양호한 결과를 보이며 (Table 2), 추시방사 선 소견상 보이는 비구컵 주위의 방사선 투과선 (radiolucent line)은 일반적으로 비구컵의 이완 소견은 아니다34,37).
Table 1. Results of morselized bone chips allograft with retention of the cementless cup
Authors Year Hips Average follow-up Result
All cup stable
Schmalzried et al.46) 1998 23 3.4 years
No new lesion
Maloney et al.31) 1997 35 3.3 years No loosening
All graft consolidation
Maloney et al.32) 1993 15 5.4 years One cup migration
Table 2. Results of morselized bone chips allograft with cementless cup revision
Authors Year Hips Average follow-up Result
Etienne et al.12) 2004 108 7 years 5% failure rate
Jasty23) 1998 019 10 years One revision
Lachiewicz & Poon27) 1998 057 7 years No revision
Woolson & Adamson51) 1996 032 5.8 years 9% failure rate
Dorr & Wan8) 1995 139 4.3 years 4.3% failure rate
3) 비구 보강환 및 골 결손부에 분쇄성 동종골을 이식하는 방법 (Morselized allograft with acetabu- lar reconstruction ring)
제 2형 및 3형 의 구조적 골결손시 50%이상 숙주 골 접촉을 얻을 수 없을 경우 주로 사용한다. 분쇄성 동종골을 감입하여 골 결손 부위에 충진한 다음 비 구컵 보강환을 나사못으로 고정하고 비구보강환 보 다 2~3 mm 작은 폴리에틸렌 라이너를 시멘트로 고 정한다. 단기 추시결과는 24%정도의 비구컵 이완율 을 보이고3), 중장기 추시결과는 20%의 재치환율과 44%정도의 비구컵 이완율이 보고되고 있다52). Pelvic discontinuity 시에는 후방지주(posteri- or column)에 pelvic reconstruction plate로 고정하고 비구보강환을 사용하여 고정한다.
3. 구조적 동종골을 사용하는 방법(Structural allograft)
비구골에 제 3형 및 4형의 구조적 골 결손이 있을 경우 사용하는 방법이며, 구조적 골(structural bone)을 비구측 골 결손부위에 고정하고 이식골과
숙주골 사이에 자가골을 충진 하는 방법이다. 비구 컵은 시멘트형, 무시멘트형, 비구컵 보강환이 사용 된다. 구조적 이식골은 비구(total acetabulum), 원위 대퇴골(distal femur), 근위 경골(proximal tibia)등이 사용된다. 일반적으로 이식골이 비구컵 의 50%이상 지지되면 실패율이 높다28). 단기 추시 시에는 비교적 양호한 결과를 보이나 중장기 추시시 실패율은 4%~47%로 보고되고 있다(Table 3, 4, 5). 실패의 주된 원인은 이식골이 재 형성기 동안에 골의 흡수가 일어나는 것이 원인이다.
4. 감입 동종골 이식법 (Impaction allograft)
비구부의 골 결손은 광법위하나 구조적 골 이식의 결과가 좋지 않으므로 분절 결손이나 광범위한 공동 결손 (cavitary defect)시에 무시멘트형 비구컵으 로 안정적 고정이 힘든 경우에 사용하는 방법으로 비교적 큰 동종골 파편 (약 10 mm 정도) 을 비구골 결손부에 감입하여 재건한 후 골 시멘트를 사용하여 폴리에틸렌 컵을 고정하는 방법이다. 감입골편은 크 Table 3. Results of structural allograft with cemented cup revision
Authors Year Allograft Hips Average follow-up Result
Sporer et al.49) 2005 Distal femur 023 10.3 years 22% failure rate
Piriou et al.42) 2003 Hemipelvis 020 5 years 35% failure rate
Paprosky et al.40) 1994 Femoral head 147 5.7 years 4% failure rate
Kwong et al.26) 1993 Femoral head 030 10 years 47% failure rate
Table 4. Results of structural allograft with acetabular reconstruction ring
Authors Year Allograft Hips Average follow-up Result
Schelfaut et al.45) 2008 Acetabulum 14 5 years 33% failure rate
Table 5. Results of structural allograft with cementlesss cup revision
Authors Year Allograft Hips Average follow-up Result
Hooten et al.21) 1994 Femoral head 27 5~10 years 44% loosening
Distal femur 19% revision
Paprosky & Magnus39) 1994 Femoral head 55 2~10 years 33% of 3A loosening
Distal femur 70% of 3B loosening
Pollock & Whiteside43) 1992 Femoral head 20 2~7 years 30% mechanical failure
기는 10 mm 정도의 입방형이 좋다고 하였는데, 이 는 이식골편의 크기가 너무 적으면 초기 안정성이 결여되어 이식골의 재형성 과정 중에 비구컵의 조기 전이가 잘 일어나는 것으로 알려져 있다48). 분절결손 의 경우에는 철사망(wire mesh)을 이용하여 결손 부위를 막아 결손부위를 동공형태로 전환하고 이식 골들을 다져 넣는다. 중장기 추시 결과는 비교적 양 호한 결과를 보이며(Table 6), 실패의 주된 원인은 비구컵의 부정위(malposition), 공동결손과 구조 적 결손이 동반되어 있는 경우 등이다24). 골다공증이 심한 공동결손 시에도 유용한 방법이다.
대퇴골 재 치환술시 동종골 이식술
비구부 골 결손 시와 마찬가지로 수술 전에 골 결손 의 형태 및 구조 등을 세밀히 파악하는 것이 중요하며, 골 결손의 분류는 AAOS 분류법이 가장 많이 쓰인다.
1. 분쇄성 동종골 이식(Morselized allograft)
1) 대퇴스템 교체 없이 골 결손부에 분쇄성 동종골을 이식하는 방법(Morselized allograft with retention of stem)
대퇴 스템이 안정 고정되어 있는 대퇴골 골 용해 시에 주로 사용된다. 추시 결과는 비교적 양호하다 (Table 7).
2) 무시멘트성 대퇴스템 교체 및 골 결손부에 분 쇄성 동종골을 이식하는 방법(Cementless stem revision with morselized allograft)
비구 골 결손 시에 무 시멘트성 비구컵 교체와 분 쇄성 골이식은 잘 알려져 있는 술식이나 대퇴측에는 보고가 드물며 그 정확한 적응증도 잘 기술되어 있 지 않다22).
2. 지주 동종골 이식(cortical strut allograft)
피질골의 골 결손이 완전하지 않아 대퇴스템을 지 지할 수는 있지만 골 결손이 광범위한 uncon- tained, non-circumferential defect 에 주로 사 용되며 얇아지거나 결손이 된 피질골에 덧대어 지주 동종골(cortical strut)을 circlage wire로 감아 주는 방법으로 접촉면이 넓고 견고한 고정을 얻기 쉬워 숙주골과 이식골의 결합(incorporation)에 유리하다. 주로 피질골의 non-circumferential
Table 6. Results of impaction allograft in acetabular revision
Authors Year Hips Average follow-up Result
Schreurs et al.47) 1998 60 1.8 years 6% failure rate
Slooff et al.48) 1996 88 5.8 years 11.4 % failure rate
Azuma et al.1) 1994 24 5.8 years 0% failure rate
Table7. Results of morselized allograft with retention of stem
Authors Year Hips Length of Follow-up Progression of
osteolytic lesions
Chang et al.5) 2007 7 5.9 years Not available
Maloney30) 2005 15 6.2 years No progression
Benson et al.2) 2000 17 > 2 years Regression of
osteolytic lesion
Hozack et al.22) 1996 154 2-5 years No progression
defect의 보 강 , cortical window의 보 강 , stress-riser의 bypass, 스템 주위골절의 보강, 감 입 골 이식술(impaction graft)의 대퇴지주 보강, 근위대퇴부 구조적 골 이식(proximal structural allograft)시 이식골과 숙주골 경계부위 보강 등을 위하여 주로 사용된다. metal plate 보다 stress- shielding이 적고, 숙주골과 결합하여 향후 재이식 술시 필요한 bone stock을 제공한다. 그러나 지주 동종골 이식으로 일차적인 대퇴 스템의 고정력을 얻 으려 하거나 무시멘트형 대퇴 스템이 지주 동종골로 골 결합을 얻도록 하면 안된다. 수술시 주의 할 점은 숙주골에 붙어있는 연부조직을 너무 많이 박리하면 혈액순환의 장애를 초래하며, 숙주골과 이식골 사이 에 자가골 이식을 충분히 하여야 한다. 사용하는 대 퇴 스템은 distal fixation stem 을 사용할 경우 체중부하가 이식골에 충분히 전달되지 않아 장기 추 시시 이식골의 흡수가 일어나므로 proximal load bearing cementless stem을 주로 사용한다. 중 장기 추시 결과는 비교적 양호하다(Table 8). 동물 실험 결과로 보면 이식 지주골의 변화는 고정후 7개 월 정도에 이식골의 상단 및 하단에 이식골의 흡수 (rounding off) 현상이 나타나고, 7.7 개월 정도에 이식골의 외면에 scalloping이 일어난다.
8개월 정도에 이식골과 숙주골 사이에 부분적인 골 결합이 나타나며, 약 12.5 개월에 완전한 골결합 소견 이 보인다. 26.5개월 정도에서 이식골의 골연화 현상 (cancellization) 이 나타나고, 마지막으로 이식골의
골흡수(resorption)가 다양한 정도로 나타난다11). 3. 구조적 동종골 이식(Structural allograft)
대퇴 근위부의 골 결손이 심하여 다른 방법으로 재 건이 어려운 경우에 사용하는 방법으로 근위 대퇴부 의 5cm 이상 완전 골 소실(noncontained cir- cumferential defect) 이 있는 AAOS 분류상 제 3,4 5형 골 결손시에 주로 사용한다. 이 방법은 근위 대퇴골의 골 결손이 심한 경우 대전자 및 중둔근을 이식 골에 부착시키고 남아있는 숙주골을 최대한 손 상하지 않고 이식골에 부착할 수 있으며, 향후 재건 술에 필요한 골을 제공할 수 있는 장점이 있으나, 수 술 수기가 매우 어렵고, 이식골과 숙주골 사이의 골 결합이 확실하지도 않고, 설사 골 결합이 일어나더라 도 오랜 기간을 필요로 하며, 이식골과 숙주골 사이 의 불유합, 이식골의 골절 및 흡수 등이 나타날 수 있 다. 수술 방법은 냉동 저장된 이식 골이나 냉동 건조 된 이식골을 사용하여 이식골과 대퇴스템을 시멘트 로 고정하고, 이 proximal femoral allograft- cement-prosthesis composite를 step cut technique 또는 oblique cut technique 을 이용하 여 숙주골에 고정한다. 이때 숙주골과 동종골 사이에 시멘트가 세어 나오지 못하게 하고, 경계부위에 충분 히 자가골 이식을 하여야 한다. 구조적 동종골을 이 용한 대퇴부 재건술의 결과는 그리 만족스럽지 못하 며, 합병증의 빈도도 높다(Table 9). 대표적인 합병 증으로는 감염(infection) 이 있으며 오랜 수술시간,
Table 8. Results of cortical strut allograft in femoral revision
Authors Year Hips Average follow-up Result
92% union
Gross et al.17) 2003 52 4.8 years 2 resorption
2 nonunion
Head et al.19) 1998 265 8-12 years 99% union
3% revision
Chandler et al.4) 1993 19 2.2 years 2 nonunion due to
devascularization
Emerson et al.11) 1992 114 2.1 years 97% union
광범위한 연부조직 손상, 심한 출혈 시에 그 빈도가 증가한다. 관절 불안정성은 대전자부가 이식 동종골 에 유합 되지 않으면 잘 발생한다. 동종 이식골의 불 유합은 이식골 경계부의 시멘트 유출, 숙주골의 광범 위한 연부조직 손상이 있을 경우 잘 발생하며, 이식 골의 골절은 나사못 등을 사용하여 stress-riser을 만들 경우에 잘생기며, 주로 이식후 2~3년 사이에
잘 발생한다. 이식골의 흡수(resorption of graft) 는 34% 정도에서 발생하고 주로 면역거부반응 (immunologic rejection)이거나 stress-shield- ing으로 발생한다고 알려져 있다18).
4. 감입 동종골 이식(Impaction allograft)
Table 10. Results of impaction allograft in femoral revision
Mean Femur
Series Stem Hips Follow up
Fracture Subsidence Failure rate Dislocation (Months)
Eldridge et al.9) Exeter, CPT 79 13 NA 023% 10% NA
Elting et al.10) CPT 67 31 05% 048% 05% 03%
Flugsrud et al.13) Exeter, CPT 10 52 00% 080% 00% NA
Gie et al.14) Exeter 58 30 07% 079% 05% 05%
Knight and Hemling25) CPT 31 31 16% 050% 00% 13%
Lind et al.24) Exeter 87 42 02% 002% 00% 06%
Masterson et al.33) Exeter 35 NA 17% 020% NA 06%
Meding et al.35) CPT 34 30 24% 044% 06% 03%
Mikhail et al.36) CPT 43 60 05% 086% 03% 08%
Ornstein et al.38) Exeter 18 24 NA 2.5% NA NA
Pekkarinen et al.41) Exeter 36 1-72 25% 086% 06% 03%
Bi-Metric 21 33% 090% 05% 14%
Head-Neck 11 64% 100% 09% 00%
van Biezen et al.50) Exeter 21 60 10% 081% 00% 05%
* NA : not available
Table 9. Results of structural allograft in femoral revision
Authors Year Hips Average follow-up Result
Nonunion (8%)
Haddad et al.18) 2000 39 5 years Dislocation (5%)
Infection (5%) Nonunion (4%)
Gross et al.16) 1993 200 2 years Dislocation 6%
Infection (3%) Nonunion (9%)
Head et al.20) 1993 11 2.4 years Dislocation (23%)
Infection (0%) Nonunion (9%)
Roberson et al.44) 1992 24 4 years Dislocation (4%)
Infection (8%)
골 결손이 심해 어떠한 방법으로도 대퇴스템을 지 지 할 수 없는 경우인 AAOS 분류상 uncon- tained, circumferential defect일 경우, 특히 젊 은 연령 일 경우 대퇴 근위부의 골구조 재생이 필요 한 경우에 주로 사용된다. 대퇴 골수강내에 충분한 파쇄골들을 감입(impaction)하여 다져 넣고 이렇 게 형성된 신생 골수강에 시멘트를 이용하여 스템을 고정하는 방법으로 Slooff 등48)이 1984년 비구부에 이 방법을 소개한 이후로 Gie 등14)이 이방법을 많 이 사용하고 있다. Slooff48)등의 보고에 의하면 수 술후 사망한 사체 연구에서 수술후 평균 3.5년 뒤에 조직학적 검사상 3가지 영역으로 재생됨을 보고하 였다. 재생 영역은 제일 바깥쪽의 remodeled cor- tical zone 이 있고, 그 안쪽으로 viable cancel- lous intermediate zone, 그리고 제일 안쪽의 necrotic inner zone으로 구성되는데 이중 remodeled cortical zone은 조직학적으로 정상 적인 피질골과 지방성 골수 및 약간의 괴사골로 되 어있어, 이식된 동종골이 결손골을 대치함을 증명한 다. 이수술시 주의 할 점은 이식 파쇄골의 크기인데, 비구부는 10 mm 정도의 size가 적당한데 반해 대 퇴골에서는 이식 파쇄골의 크기는 3~5 mm 가 적당 하므로9), bone mill 보다는 bone nibbler로 파쇄 골을 만드는 것이 좋으며, 대퇴 골수강내에 단단하 게 채워 넣는 것이 좋다. 대퇴스템은 일반적으로 highly polished colorless double taper stem 이 선호되며, 최근에는 효율적으로 bone 을 감입할 수 있는 여러 기구들이 개발되어 있다. 수술의 결과 는 중장기 추시 결과는 비교적 양호한 편이다 (Table 10). 합병증으로는 대퇴골 골절 또는 대퇴 골 천공 (perforation)이 5~24%에서 발생 하며
9,38), 골 결손이 심하면 심할수록 잘 생긴다. 효과적
인 감입이 어려울 경우 심한 대퇴 스템의 침강도 보 고되고 있다.
결 론
인공고관절 재 치환술이 보편화함에 따라 동종골 을 이용한 골 결손 부위의 골 수복 방법은 갈수록 그 사 용 빈 도 가 증 가 하 고 있 다 . 파 쇄 성 동 종 골
(morselized allograft) 이식은 주로 대퇴부나 비 구부의 동공형-비구조적 골 결손(cavitary-non- structural defect)에 주로 사용하고, 구조적 동종 골(structural allograft)은 지주형-구조적 골 결 손(segmental-structural defect)부위에 주로 사용한다. 그러나 구조적 동종골의 경우 장기 추시 결과 이식골의 흡수 등이 문제가 됨으로 최근에는 구조적 골 결손 시에도 파쇄감입 동종골 이식술 (impaction allograft)이 선호 되고 있으며, 이식 골의 성공적인 재생을 위해서는 수술전 골 결손의 정확한 평가가 필수적이고, 되도록이면 이식되는 숙 주골의 연부조직 손상을 최소화 하고, 이식골과 숙 주골의 연결부위에 자가골을 충분히 이식하는 것이 중요하다.
REFERENCES
01) Azuma T, Yasuda H, Okagaki K, Sakai K:
Compressed allograft chips for acetabular recon- struction in revision hip arthroplasty. J Bone Joint Surg Br, 76:740-744, 1994.
02) Benson ER, Christensen CP, Monesmith EA, Gomes SL, Bierbaum BE: Particulate bone grafting of osteolytic femoral lesions around sta- ble cementless stems. Clin Orthop Relat Res, 381:
58-67, 2000.
03) Berry DJ, Muller ME: Revision arthroplasty using an anti-protrusio cage for massive acetabu- lar bone deficiency. J Bone Joint Surg Br, 74:711- 715, 1992.
04) Chandler HP, King D, Limbird R, Hedley A, McCarthy J, Penenberg B, Danylchuk K: The use of cortical allograft struts for fixation of frac- tures associated with well-fixed total joint prosthe- ses. Semin Arthroplasty, 4:99-107, 1993.
05) Chang JD, Yoo JH, Hur M, Lee SS, Chung YK, Lee CJ: Revision total hip arthroplasty for pelvic osteolysis with well-fixed cementless cup. J Arthroplasty, 22:987-992, 2007.
06) Claus AM, Totterman SM, Sychterz CJ, Tamez-Pena JG, Looney RJ, Engh CA Sr:
Computed tomography to assess pelvic lysis after total hip replacement. Clin Orthop Relat Res, 422:
167-174, 2004.
07) D’’Antonio JA, Capello WN, Borden LS, Bargar WL, Bierbaum BF, Boettcher WG, Steinberg ME, Stulberg SD, Wedge JH : Classification and management of acetabular abnormalities in total hip arthroplasty. Clin Orthop Relat Res, 243:126-137, 1989.
08) Dorr LD, Wan Z: Ten years of experience with porous acetabular components for revision surgery.
Clin Orthop Relat Res, 319:191-200, 1995.
09) Eldridge JD, Smith EJ, Hubble MJ, et al.: Massive early subsidence following femoral impaction grafting. J Arthroplasty, 12:535-540, 1997.
10) Elting JJ, Mikhail WE, Zicat BA, et al. : Preliminary report of impaction grafting for exchange femoral arthroplasty. Clin Orthop Relat Res, 319:159-167, 1995.
11) Emerson RH Jr, Malinin TI, Cuellar AD, Head WC, Peters PC: Cortical strut allografts in the reconstruction of the femur in revision total hip arthroplasty. A basic science and clinical study.
Clin Orthop Relat Res, 285:35-44, 1992.
12) Etienne G, Bezwada HP, Hungerford DS, Mont MA: The incorporation of morselized bone grafts in cementless acetabular revisions. Clin Orthop Relat Res, 428:241-246, 2004.
13) Flugsrud GB, Ovre S, Grogaard B, et al.:
Cemented femoral impaction bone grafting for severe osteolysis in revision hip arthroplasty:
Good results at 4-year follow-up of 10 patients.
Arch Orthop Trauma Surg, 120:386-389, 2000.
14) Gie GA, Linder L, Ling RS, et al.: Impacted can- cellous allografts and cement for revision total hip arthroplasty. J Bone Joint Surg Br, 75:14-21, 1993.
15) Gross AE: Revision arthroplasty of the acetabu- lum with restoration of bone stock. Clin Orthop Relat Res, 369:198-207, 1999.
16) Gross AE, Allan DG, Lavoie GJ, Oakeshott RD: Revision arthroplasty of the proximal femur using allograft bone. Orthop Clin North Am, 24:
705-715, 1993.
17) Gross AE, Wong PK, Hutchison CR, King AE:
Onlay cortical strut grafting in revision arthro- plasty of the hip. J Arthroplasty, 18:104-106, 2003.
18) Haddad FS, Spangehl MJ, Masri BA, Garbuz DS, Duncan CP: Circumferential allograft replacement of the proximal femur. A critical analysis. Clin Orthop Relat Res, 371:98-107, 2000.
19) Head WC, Malinin TI, Mallory TH, Emerson RH Jr.: Onlay cortical allografting for the femur.
Orthop Clin North Am, 29:307-312, 1998.
20) Head WC, Wagner RA, Emerson RH Jr, Malinin TI: Restoration of femoral bone stock in revision total hip arthroplasty. Orthop Clin North Am, 24:697-703, 1993
21) Hooten JP Jr, Engh CA Jr, Engh CA: Failure of structural acetabular allografts in cementless revi- sion hip arthroplasty. J Bone Joint Surg Br, 76:
419-422, 1994.
22) Hozack WJ, Bicalho PS, Eng K: Treatment of femoral osteolysis with cementless total hip revi- sion. J Arthroplasty, 11:668-672, 1996.
23) Jasty M: Jumbo cups and morselized graft.
Orthop Clin North Am, 29:249-254, 1998.
24) Knight JL, Fujii K, Atwater R, Grothaus L:
Bone-grafting for acetabular deficiency during pri- mary and revision total hip arthroplasty. A radi- ographic and clinical analysis. J Arthroplasty, 8:
371-382, 1993.
25) Knight JL, Helming C: Collarless polished tapered impaction grafting of the femur during revision total hip arthroplasty: Pitfalls of the sur- gical technique and follow-up in 31 cases. J Arthroplasty, 15:159-165, 2000.
26) Kwong LM, Jasty M, Harris WH: High failure rate of bulk femoral head allografts in total hip acetabular reconstructions at 10 years. J Arthroplasty, 8:341-346, 1993.
27) Lachiewicz PF, Poon ED: Revision of a total hip arthroplasty with a Harris-Galante porous-coated acetabular component inserted without cement. A follow-up note on the results at five to twelve years. J Bone Joint Surg Am, 80:980-984, 1998.
28) Leopold SS, Jacobs JJ, Rosenberg AG : Cancellous allograft in revision total hip arthro- plasty. A clinical review. Clin Orthop Relat Res, 371:86-97, 2000.
29) Lind M, Krarup N, Mikkelsen S, et al. : Exchange impaction allografting for femoral revi- sion hip arthroplasty: Results in 87 cases after 3.6 years’ follow-up. J Arthroplasty, 17:158-164, 2002.
30) Maloney WJ: The surgical management of femoral osteolysis. J Arthroplasty, 20:75-78, 2005 31) Maloney WJ, Herzwurm P, Paprosky W,
Rubash HE, Engh CA: Treatment of pelvic oste- olysis associated with a stable acetabular compo- nent inserted without cement as part of a total hip replacement. J Bone Joint Surg Am, 79:1628- 1634, 1997.
32) Maloney WJ, Peters P, Engh CA, Chandler H:
Severe osteolysis of the pelvic in association with acetabular replacement without cement. J Bone Joint Surg Am, 75:1627-1635, 1993.
33) Masterson EL, Busch CA, Duncan CP, et al.:
Impaction allografting of the proximal femur using a Charnley-type stem: A cement mantle analysis. J Arthroplasty, 14:59-63, 1999.
34) McGann WA, Welch RB, Picetti GD 3rd.:
Acetabular preparation in cementless revision total hip arthroplasty. Clin Orthop Relat Res, 235:
35-46, 1988.
35) Meding JB, Ritter MA, Keating EM, et al.: Impaction bone-grafting before insertion of a femoral stem with cement in revision total hip arthroplasty: A minimum two-year follow-up study. J Bone Joint Surg Am, 79: 1834-1841, 1997.
36) Mikhail WE, Wretenberg PF, Weidenhielm LR, et al.: Complex cemented revision using pol- ished stem and morselized allograft: Minimum 5- years’ follow-up. Arch Orthop Trauma Surg, 119:
288-291, 1999.
37) Nivbrant B, Karrholm J: Migration and wear of hydroxyapatite-coated press-fit cups in revision hip arthroplasty: a radiostereometric study. J Arthroplasty, 12: 904-912, 1997.
38) Ornstein E, Atroshi I, Franzen H, et al.: Results of hip revision using the Exeter stem, impacted allograft bone, and cement. Clin Orthop Relat Res, 389: 126-133, 2001.
39) Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty.
Acetabular technique. Clin Orthop Relat Res, 298:
147-155, 1994.
40) Paprosky WG, Perona PG, Lawrence JM:
Acetabular defect classification and surgical reconstruction in revision arthroplasty. A 6-year follow-up evaluation. J Arthroplasty, 9: 33-44, 1994.
41) Pekkarinen J, Alho A, Lepisto J, et al. : Impaction bone grafting in revision hip surgery: A high incidence of complications. J Bone Joint Surg Br, 82: 103-107, 2000.
42) Piriou P, Sagnet F, Norton MR, de Loubresse CG, Judet T: Acetabular component revision with frozen massive structural pelvic allograft: average 5-year follow-up. J Arthroplasty. 2003
43) Pollock FH, Whiteside LA: The fate of massive allografts in total hip acetabular revision surgery .J Arthroplasty, 7: 271-276, 1992.
44) Roberson JR: Proximal femoral bone loss after total hip arthroplasty. Orthop Clin North Am, 23:
291-302, 1992.
45) Schelfaut S, Cool S, Mulier M: The use of struc- tural periacetabular allografts in acetabular revi- sion surgery: 2.5-5 years follow-up. Arch Orthop Trauma Surg, 2008.
46) Schmalzried TP, Fowble VA, Amstutz HC: The fate of pelvic osteolysis after reoperation. No recurrence with lesional treatment. Clin Orthop Relat Res. 350: 128-137, 1998.
47) Schreurs BW, Slooff TJ, Buma P, Gardeniers JW, Huiskes R: Acetabular reconstruction with impacted morsellised cancellous bone graft and cement. A 10- to 15-year follow-up of 60 revision arthroplasties. J Bone Joint Surg Br, 80: 391-395, 1998.
48) Slooff TJ, Buma P, Schreurs BW, Schimmel JW, Huiskes R, Gardeniers J: Acetabular and femoral reconstruction with impacted graft and
cement. Clin Orthop Relat Res, 324:108-115, 1996.
49) Sporer SM, O’Rourke M, Chong P, Paprosky WG: The use of structural distal femoral allografts for acetabular reconstruction. Average ten-year fol- low-up. J Bone Joint Surg Am, 87:760-765, 2005.
50) van Biezen FC, ten Have BL, Verhaar JA:
Impaction bone-grafting of severely defective femora in revision total hip surgery: 21 hips fol- lowed for 41-85 months. Acta Orthop Scand, 71:
135-142, 2000.
51) Woolson ST, Adamson GJ: Acetabular revision using a bone-ingrowth total hip component in patients who have acetabular bone stock deficien- cy. J Arthroplasty, 11:661-667, 1996.
52) Zehntner MK, Ganz R: Midterm results (5.5-10 years) of acetabular allograft reconstruction with the acetabular reinforcement ring during total hip revision. J Arthroplasty, 9:469-479, 1994.
53) Zimlich RH, Fehring TK: Underestimation of pelvic osteolysis: the value of the iliac oblique radiograph. J Arthroplasty, 15:796-801, 2000.