8례의 메켈세포암종의 후향적 연구
오승일·진웅식·장학·권성택·민경원 서울대학교 의과대학 성형외과학교실
Background: Merkel cell carcinoma (MCC) is a rare locally aggressive cutaneous neuroendocrine carcinoma with a high incidence of local recurrence, regional lymph node metastasis, followed by distant metastasis. Because of shortage of the retrospective study, standard treatment has not been established. The purpose of this study was to present the surgical treatment and outcome of 8 patients with MCC.
Methods: We report our experiences with 8 patients who underwent treatment for MCC at our institution from 2000 through 2012. Two men and 6 women received treatment for MCC. The mean age was 76.4 years (range, 53 to 93 years).
Results: The follow-up period ranged from 7 to 26 months (mean, 22.9). During the follow-up period, three of 8 patients had a relapse (mean time before recurrence, 10 months; 1 month, 7 months, and 22 months). After primary surgery, 3 patients underwent radiotherapy, and 1 patient received chemotherapy.
Conclusion: MCC is an aggressive skin cancer with a high rate of local recurrence. Complete surgical excision is the mainstay of local treatment, but adjuvant radiotherapy should be considered for better local control.
Keywords: Carcinoma / Merkel cell / Disease management
A Retrospective Analysis of Eight Cases of Merkel Cell Carcinoma
Seung Il Oh, Ung Sik Jin, Hak Chang, Sung Tack Kwon, Kyung Won Minn
Department of Plastic and Reconstructive Surgery, Seoul National University School of Medicine, Seoul, Korea
Introduction
Merkel cell carcinoma (MCC) is an uncommon, primary neu- roendocrine malignant tumor first described in 1972 by Toker [1].
MCC involves frequently sun-exposed areas, with approximately 50% of cases arising in the head and neck region [2]. Occurrence of this cancer is also reported after radiotherapy and immunosup- pressive therapy or in association with other malignant neoplasms.
Clinically, prognostic factors include tumor stage, older age, pri- mary location, and immunosuppression. However, reported prog-
nostic factors are various, and consistent conclusion is not easy as small and large lesions are grouped together for prognostic pur- poses. MCC is characterized by a high rate of local recurrence (12%
to 50%), regional node metastasis (17% to 76%), and distant metas- tasis (12% to 50%) [3-5].
We detected eight cases of MCC from 2000 through 2012 at our institution. The aims of this study were to retrospectively review our experience of surgical treatment in Korean patients with MCC and to study its adjuvant management and outcome.
Materials and Methods
A computer search of patients with a histological diagnosis of MCC was performed in the pathology department. Only patients treated at our institution were included for analysis. We conducted
Correspondence: Ung Sik Jin
Department of Plastic and Reconstructive Surgery, Seoul National University School of Medicine, 101 Daehak-ro, Jongno-gu, Seoul 110-744, Korea Tel: +82-2-2072-2375 / Fax: +82-2-741-3985 / E-mail: [email protected] Received February 1, 2013 / Revised March 15, 2013 / Accepted March 15, 2013
Original Article
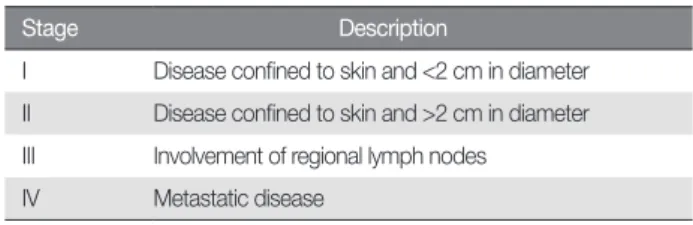
a retrospective analysis of all 8 patients treated between 2000 and 2012. Medical information was obtained from the patients’ medi- cal records and direct patient contact. The four-tiered staging sys- tem of the Memorial Sloan-Kettering Cancer Center (Table 1), which takes into account tumor size and nodal status, was used for clinical staging. Due to the small number of patients with various and different management approaches, statistical analysis was not performed for prognostic factors.
Results
1. Patients and tumor characteristicsCharacteristics of all of the patients are shown in Table 2. Of the 8 patients, there were two males (25%) and 6 females (75%). Their ages ranged from 53 to 93 years (mean 76.1 years). The most com- mon site of tumor location was the cheek (6 cases, 75%), followed by the forearm (1 case), and thigh (1 case). The average tumor size at initial presentation was 22.5 mm (range from 8 to 45 mm) (Fig. 1).
Stage I disease was present in four patients, stage II disease in three patients and stage III disease in one patient.
2. Primary treatment
All patients received surgery as the primary treatment modality.
Therapeutic lymph node dissection was performed in one patient and elective lymph node dissection (ELND) in one patient. The exci- sion margins ranged from 0.5 to 3 cm (mean, 1.4 cm). Six patients with a cheek tumor received excision with a 0.5 to 2 cm margin (mean, 1.2 cm). Two patients with tumors elsewhere other than the cheek received excision with a 1 to 3 cm margin (mean, 1.5 cm). Sen- tinel lymph node biopsy (SLNB) was conducted in only one case (case 7). In that case, ELND was not performed because the frozen and permanent biopsy results of the sentinel lymph nodes were nega- tive for malignancy. Therapeutic ELND was performed in one pa- tient whose lymph node biopsy was positive for malignancy (case 2).
3. Reconstruction
Among the patients who presented with tumors on the cheek, four had wound closure using a local flap, and two patients had closure with a split thickness skin graft (Fig. 2). Apart from those with cheek tumors, one patient had closure with a local flap, and the rest of the patients had closure with a split thickness skin graft.
4. Recurrence
The follow-up period ranged from 7 to 26 months (mean, 22.9 months). Recurrence was observed in three out of the eight cases during the follow-up period (cases 2, 4, and 5). Local and lymph node recurrence was seen in case 2 at 3-month postoperative follow- Table 1. Four-tiered staging system for Merkel cell carcinoma (Memorial
Sloan-Kettering Cancer Center)
Stage Description
I Disease confined to skin and <2 cm in diameter II Disease confined to skin and >2 cm in diameter III Involvement of regional lymph nodes
IV Metastatic disease
Table 2. Analysis of eight patients with Merkel cell carcinoma
No. Sex/Age Size (mm) Location Stage Treatment Surgical margin (mm) SLNB AdjTx. Follow-up (mo) Recurrence
1 F/53 15×12 Cheek I WLE+local flap 12 No No 18 No
2 M/58 25×20 Thigh III WLE+skin graft 30 Yes CTx.+RTx. 12 Yes
3 M/74 26×13 Cheek II WLE+skin graft 20 No No 12 No
4 F/79 15×12 Cheek I WLE+skin graft 10 No No 26 Yes
5 F/77 30×30 Cheek II WLE+local flap 5 No No 12 Yes
6 F/92 16×9 Cheek I WLE+local flap 20 No RTx. 8 No
7 F/85 8×8 Forearm I WLE+local flap 10 Yes RTx. 8 No
8 F/93 45×42 Cheek II WLE+local flap 5 No No 7 No
SLNB, sentinel lymph node biopsy; AdjTx., adjuvant treatment; WLE, wide local excision; CTx., chemotherapy; RTx., radiotherapy.
up. Positron emission tomography was performed to evaluate dis- tant metastases, but none were found at 3-month follow-up. Exter- nal iliac lymph node dissection and wide excision of the recurred lesion were performed. In cases 4 and 5, regional lymph node recur- rence was found at 12 months and 3 month postoperatively, but these patients refused further treatment due to personal matters.
5. Adjuvant treatment
Postoperative radiotherapy was performed in three cases. We recommended loco-regional radiotherapy regardless of tumor stage to reduce the occurrence of local recurrence; however the rest of the patients refused radiotherapy due to old age, poor health, or personal matters. Chemotherapy was performed in one metastatic case for palliative purposes (case 2).
6. Survival
In the whole sample, there was one tumor-related death 2 year after the operation (case 2), and there was one non-tumor-related death (case 6).
Discussion
MCC is an aggressive carcinoma with poor prognosis. This tu- mor probably arises from a cutaneous mechanoreceptor cell (Merkel cell) located in the basal layer of the epidermis. The annual incidence of MCC is approximately 3 per million in the United States [2]. MCC most commonly occurs in the head and neck re- gion of elderly patients; the mean age is 68 years. It typically pres- ents as a solid, asymptomatic, red-pink, and dome shaped dermal nodule with a tendency to enlarge rapidly over a period of few weeks to months. Acneform and plaque-like lesions have also been described, particularly on the trunk [2,3]. Disease rarely occurs be- fore the age of 50, after which the incidence rises sharply. In one large review, the median age of patients at diagnosis was 69 years [3]. However, MCC occurs more frequently at a substantially younger age among immunosuppressed patients, with an inci- dence between 5 and 11 times greater in individuals with organ transplants and AIDS, respectively [2,4]. Several studies have sug- gested that unfavorable factors related to poor outcome include male gender and patients with involvement in the head and neck region [3,4]. However, in other studies, patients with tumors in the head and neck region had significantly smaller lesions than pa- tients with tumors in other locations [6]. Because of the signifi- cance of size in relation to overall survival, patients with tumors in the head and neck region are most likely to have an improved sur- vival rate secondary to the small size of their tumors rather than due to the difference in behavior because of location alone.
Microscopically, MCC is located in the dermis, infiltrating the subcutaneous tissue; the overlying dermis is normal. The charac- teristic histological findings are nuclei with finely granular chro- matin, small-cell size, dense hyperchromatic nuclei and nuclear moulding (Fig. 3). Because at times it is impossible to differentiate from small cell carcinomas of the lung, immunohistochemical Fig. 1. Case 5. A 77-year-old woman with Merkel cell carcinoma on
her right cheek. (A) Preoperative photograph. (B) Close-up view.
Fig. 2. Case 8. A 93-year-old woman with Merkel cell carcinoma on her left cheek. (A) Preoperative photograph. (B) Postoperative (wide excision and local flap) photograph on month 1.
analysis is routinely performed for diagnosis. Staining for cytoker- atin 20 (CK 20) is a fairly accurate indicator, but a third of pulmo- nary small cell carcinomas also stain for CK 20. More certainty about the etiology of the lesion can be obtained by the additional use of thyroid transcription factor 1 (TTF-1). While most small cell carcinomas of the lung stain for TTF-1, MCC does not [2,4].
There is no international consent on a staging system for MCC.
The most common staging system was developed by the Memorial Sloan-Kettering Cancer Center, which divided the disease into four stages: the diameter of the primary lesion, the absence or presence of nodal metastases, and distant metastatic disease (Table 1). In a recent large study series that included 251 MCC patients, this classification system performed well in defining the prognosis of the disease, with disease stage being the only independent predictor of survival (stage I, 81%; stage II, 67%; stage III, 52%; stage IV, 11%; p=0.001) [6].
In this study, we found four patients in stage I, three in stage II, and one in stage III. A stage III case (case 2) had clinical palpable inguinal lymph nodes at the time of presentation, and ELND was performed. However, as mentioned above, local and lymph nodal recurrences were seen in that case at 3 months postoperatively.
Multiple different guidelines exist for the management of MCC, although none are universally accepted and all are based on limit- ed data. Surgical excision remains the cornerstone of therapy.
There have been no randomized comparative study on diverse margin sizes and clinical results; the published literature has most-
ly failed to report the exact margin size. Historical data suggest that wide excision with a 3 cm margin is the treatment of choice for lo- calized tumors [5,7]. However, a low local recurrence rate (8%) has been accomplished after margin-free resection, with the margin size averaging 1.1 cm [8]. In our study, 2 patients who presented with MCC on the extremity received wide excision with 2 and 3 cm margins. However, the question still remains regarding the recommended margins for tumors in the head and neck region.
We did not perform wide excision with margins over 2 cm in the cases of MCC on the cheek. During the follow-up period, we found local recurrence in 2 patients with 0.5 and 1.0 cm margins. We rec- ommend wide excision of the primary lesion with a margin of at least 1 cm for early stage MCC in the head and neck region. If this is difficult, a negative surgical margin should be achieved.
Although MCC is believed to be a radio-responsive malignant neoplasm, different MCC cell lines are found to be different in their radio-responsiveness [9].Some clinical studies have suggested that the rate of local recurrence and regional lymph node metastasis may be significantly lower in patients receiving adjuvant radiotherapy.
Many other clinical studies have also advocated local radiotherapy to reduce the occurrence of local recurrence [9,10].In our study, we recommended radiotherapy after wide excision of MCC for any stage. However, radiotherapy was not performed in some cases. Ev- ery decision has to be taken individually depending on age, general condition, and choice of the patient. Recurrence was observed in two out of five cases without radiotherapy during the follow-up pe- riod (case 4, 5). In one case of stage III, recurrence and metastasis were observed after completion of adjuvant radiotherapy (case 2).
The role of adjuvant chemotherapy is still debated because of the lack of data and uneven response rate. Several authors have sug- gested that MCC is a chemosensitive disease, and the addition of adjuvant chemotherapy to local excision and radiation is a reliable therapeutic option because many patients die of distant metastasis [11]. However, there is no powerful evidence that adjuvant chemo- therapy, both after the initial excision of the tumor or after tumor recurrence improves survival [5,8]. In addition, adjuvant chemo- therapy has failed to provide any benefit. Garneski and Nghiem [12] showed that the chemotherapeutic regimen is toxic, and since the target population is the elderly, a treatment-related death rate of Fig. 3. Histologic findings of Merkel cell carcinoma (case 5). The
tumorwas composed of monotonous small round cells with scanty cytoplasm and hyperchromatic nuclei (H&E, × 400).
approximately 16% is detected in patients older than 65 years. Mor- bidity is also high in these cases. The chemotherapeutic regimen is adapted from that used for small-cell lung carcinoma. Without the evidence of improved outcome, it does not seem reasonable to take on the risk of such a toxic treatment [6,13]. In our study, one patient received adjuvant chemotherapy as palliative treatment for ad- vanced disease with multiple metastasis (case 2).
The presence of lymph node involvement is an important prog- nostic factor [9].The use of SLNB has also been reported in MCC recently. Gupta et al. [14] reviewed 122 patients with MCC who underwent SLNB and observed that 60% of those patients with a positive sentinel node recurred in three years compared to a recur- rence rate of 20% in those with negative SLNB [6,12]. Allen et al. [6]
advocate the significance of determining nodal status, and they do not suggest the routine use of adjuvant radiotherapy in MCC pa- tients who underwent SLNB with no micrometastasis.
Kokoska et al. [8] reported 100% versus 35% 2-year overall survival rate and 0% versus 91% loco-regional recurrence for patients receiv- ing ELND versus no ELND. ELND in patients with clinically nega- tive lymph nodes is advocated by many authors [5,7], but others rec- ommend this only for patients with worrisome prognostic features, such as larger lesions, 10 or more mitoses per high-power field, small cell histologic findings, and head and neck involvement [15].
We reviewed our experience of 8 patients with MCC retrospec- tively. In our opinion, a low local recurrence rate can be achieved af- ter margin-negative resection with a resection margin size of at least 1.0 cm. SLNB should be considered to determine accurate nodal staging. Also, we suggest adjuvant radiotherapy after surgery for better local control. However, adjuvant chemotherapy is not recom- mended because its role remains controversial. In our study, the number of patients was small and the follow up period was short, so the evidence level was not high. In the future, we need a perspective study with a larger number of cases to analyze MCC disease.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
References
1. Toker C. Trabecular carcinoma of the skin. Arch Dermatol 1972;105:
107-10.
2. Rockville Merkel Cell Carcinoma Group. Merkel cell carcinoma: re- cent progress and current priorities on etiology, pathogenesis, and clin- ical management. J Clin Oncol 2009;27:4021-6.
3. Heath M, Jaimes N, Lemos B, Mostaghimi A, Wang LC, Penas PF, Nghiem P. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J Am Acad Dermatol 2008;58:
375-81.
4. Becker JC. Merkel cell carcinoma. Ann Oncol 2010;21 Suppl 7:vii81-5.
5. Allen PJ, Zhang ZF, Coit DG. Surgical management of Merkel cell car- cinoma. Ann Surg 1999;229:97-105.
6. Allen PJ, Bowne WB, Jaques DP, Brennan MF, Busam K, Coit DG.
Merkel cell carcinoma: prognosis and treatment of patients from a sin- gle institution. J Clin Oncol 2005;23:2300-9.
7. Yiengpruksawan A, Coit DG, Thaler HT, Urmacher C, Knapper WK.
Merkel cell carcinoma. Prognosis and management. Arch Surg 1991;
126:1514-9.
8. Kokoska ER, Kokoska MS, Collins BT, Stapleton DR, Wade TP. Early aggressive treatment for Merkel cell carcinoma improves outcome. Am J Surg 1997;174:688-93.
9. Meeuwissen JA, Bourne RG, Kearsley JH. The importance of postop- erative radiation therapy in the treatment of Merkel cell carcinoma. Int J Radiat Oncol Biol Phys 1995;31:325-31.
10. Lewis KG, Weinstock MA, Weaver AL, Otley CC. Adjuvant local irra- diation for Merkel cell carcinoma. Arch Dermatol 2006;142:693-700.
11. King MM, Osswald MB. Adjuvant chemotherapy for Merkel cell carci- noma. Am J Clin Oncol 2005;28:634.
12. Garneski KM, Nghiem P. Merkel cell carcinoma adjuvant therapy: cur- rent data support radiation but not chemotherapy. J Am Acad Derma- tol 2007;57:166-9.
13. Jabbour J, Cumming R, Scolyer RA, Hruby G, Thompson JF, Lee S.
Merkel cell carcinoma: assessing the effect of wide local excision, lymph node dissection, and radiotherapy on recurrence and survival in early-stage disease: results from a review of 82 consecutive cases di- agnosed between 1992 and 2004. Ann Surg Oncol 2007;14:1943-52.
14. Gupta SG, Wang LC, Penas PF, Gellenthin M, Lee SJ, Nghiem P. Senti- nel lymph node biopsy for evaluation and treatment of patients with Merkel cell carcinoma: The Dana-Farber experience and meta-analysis of the literature. Arch Dermatol 2006;142:685-90.
15. Cotlar AM, Gates JO, Gibbs FA Jr. Merkel cell carcinoma: combined surgery and radiation therapy. Am Surg 1986;52:159-64.