65 Received:April 10, 2017, Revised:May 13, 2017, Accepted:May 29, 2017
Corresponding to:Young Mo Kang, Division of Rheumatology, Department of Internal Medicine, Kyungpook National University Hospital, 130 Dongdeok-ro, Jung-gu, Daegu 41944, Korea. E-mail:[email protected]
Copyright ⓒ 2018 by The Korean College of Rheumatology. All rights reserved.
This is a Open Access article, which permits unrestricted non-commerical use, distribution, and reproduction in any medium, provided the original work is properly cited.
Case Report
pISSN: 2093-940X, eISSN: 2233-4718
Journal of Rheumatic Diseases Vol. 25, No. 1, January, 2018 https://doi.org/10.4078/jrd.2018.25.1.65
Bilateral Involvement of Juvenile Temporal Arteritis Associated with Kimura Disease
Na Ri Kim1, Churl Hyun Im1, Jong Wan Kang1, Ji Hun Kim2, Tae-In Park3, Han-Ik Bae3, Eon Jeong Nam1, Young Mo Kang1
1Division of Rheumatology, Department of Internal Medicine, Kyungpook National University School of Medicine, Daegu, 2Division of Rheumatology, Department of Internal Medicine, Andong Medical Group Hospital, Andong, 3Department of Pathology, Kyungpook National University School of Medicine, Daegu, Korea
Juvenile temporal arteritis (JTA) is a localized nodular arteritis confined to the temporal artery without evidence of systemic in- flammation, and it occurs mainly in patients younger than 50 years. From the first case report, the pathological features of JTA have been suspected to be the morphological equivalent of Kimura disease (KD), which has been supported further by the con- current cases of JTA with KD. We present the first case of bilateral JTA accompanying KD, which was confirmed by histological and ultrasound evaluations and supports the hypothesis that JTA is a manifestation of KD. The un-excised JTA lesion was re- solved completely after corticosteroid therapy with no recurrence. (J Rheum Dis 2018;25:65-68)
Key Words. Juvenile temporal arteritis, Kimura disease, Corticosteroids
INTRODUCTION
Juvenile temporal arteritis (JTA) is a localized nodular arteritis confined to the temporal artery, without evi- dence of systemic inflammation, and it occurs mainly in patients younger than 50 years [1]. Histologic examina- tion of the JTA shows intimal proliferation and panarter- itis with lymphocyte and eosinophil infiltrates but no giant cell, which may extend to the perivascular area [1].
From the first case report [1], the pathologic features of JTA have been suspected to be the morphological equiv- alent of Kimura disease (KD), which has been supported further by the concurrent cases of JTA with KD [2-5]. KD is a chronic inflammatory disorder that affects the sub- cutaneous tissue and lymph nodes, especially in the head and neck area, with peripheral blood eosinophilia [6].
Pathological study of the specimens from KD showed a marked reactive follicular hyperplasia with prominent follicles that were surrounded with a large number of eo- sinophils, lymphocytes and mast cells [6]. Fibrosis and
vascular proliferation were also seen in KD [6].
Determination of the association between JTA and KD, that is, whether JTA is a manifestation of KD or whether these two diseases occur coincidentally, is important not only for understanding of the disease pathogenesis, but for the clinical decision of management. We present the first case of bilateral JTA accompanying KD, which showed a good response to corticosteroid therapy.
CASE REPORT
A 37 year old Asian Korean man visited the hospital for painless nodular lesions on bilateral temporal areas. Two years earlier, right inguinal and left antecubital masses developed with no previous history of either local in- fection or trauma. A few months later, a nodular lesion of the size of a corn, without cutaneous irritation symp- toms, developed on the left anterior temporal area (Figure 1A). He did not have constitutional symptoms, except for occasional headache. Two weeks before hospi-
Na Ri Kim et al.
66 J Rheum Dis Vol. 25, No. 1, January, 2018
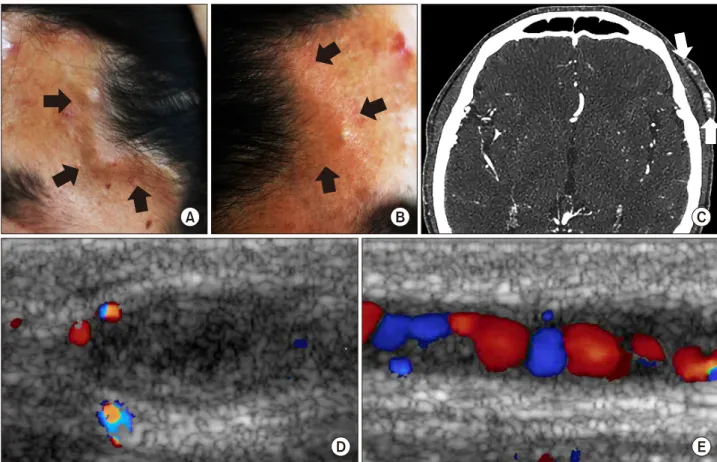
Figure 1. Gross appearance (A: left, B: right), computed tomographic angiography (C) and Doppler ultrasound images (D: short ax- is, E: long axis) of the nodular lesion on the left superficial temporal artery.
tal admission, another nodular lesion of smaller size was detected on the opposite temporal area (Figure 1B).
On physical examination, both lesions were firm, pain- less, and pulsatile on both temporal arteries. Two en- larged painless lymph nodes were palpated on the right inguinal and left antecubital areas. There was no evidence of other organ involvement. Laboratory tests showed no abnormalities except for peripheral blood eosinophilia (15.4%) and markedly elevated serum immunoglobulin E level (5,111 IU/mL). We identified the enhanced focal wall thickening at the left superficial temporal artery on computed tomographic angiography (Figure 1C).
Ultrasonography with Doppler images of the lesional su- perficial temporal artery (Figure 1D and 1E) showed dif- fuse edematous wall thickening (i.e., the “halo” sign), vascular tortuosity, and irregular luminal stenosis with turbulent flow.
Histological features of both left antecubital and right inguinal lymph nodes included exuberant follicular for- mation and angiogenesis, with prominent eosinophilic infiltration, which were typical KD histology (Figure 2).
On excisional biopsy of the nodular lesion on the left su-
perficial temporal artery, the vascular lumen was com- pacted by the hyperplastic endothelium (CD34 positive), with canalicular tract formation. Disruption of internal elastic lamina and adventitial inflammation with eosino- philic infiltrates were found on the vessel wall (Figure 3).
However, there were no epithelioid endothelial cells or giant cells within the lesions.
The patient was diagnosed as JTA on bilateral superficial temporal arteries, accompanying KD. The patient re- ceived treatment with corticosteroid of 0.5 mg/kg per day, followed by azathioprine therapy (1.5 mg/kg) with tapering of corticosteroid. The nodular lesion on the right superficial temporal artery disappeared 5 months after treatment. The patient had received maintenance therapy for a year. There was no recurrence of either JTA or KD during 7 years of follow-up.
DISCUSSION
The clinical and pathological presentation of this case was compatible with those of JTA with bilateral involve- ment, accompanying KD lesions. Among 21 cases identi-
Bilateral Involvement of Juvenile Temporal Arteritis Associated with Kimura Disease
www.jrd.or.kr 67
Figure 2. Inguinal and antecubital lymph nodes showed markedly increased lymphoid follicles with germinal centers and exuber- ant eosinophilic infiltrations, which is compatible with Kimura disease (H&E, A: ×40; B: ×200; C: ×400).
Figure 3. Biopsy of the superficial temporal artery lesions (H&E, A: ×40; B: ×100) showed intravascular proliferating structures, with eosinophilic infiltrations covered by endothelial linings (C: CD 34, ×200) and intramural and perivascular inflammatory lesions.
fied in a PubMed search for JTA [1,2,5,7-12] and the pres- ent case, most of the JTA patients were younger than 40 years old, except for two cases. Males were predom- inantly affected with JTA than female (15 males in 21 cas- es). Most JTA lesions were painless mass at the temporal area without systemic symptoms, except for headache and fatigue. These patients did not show any internal or- gan involvement and systemic inflammatory reaction.
Histologically, JTA showed endothelial proliferation with luminal narrowing, disruption of the internal elastic lami- na, and panarteritis with lymphoid follicle formation in the periarterial tissues [1]. KD showed similar pathologic features with JTA, including lymphatic eosinophilic in- filtration, vascular proliferation, and multiple follicle for- mation, except for differences in the distribution of the involved tissues. Previous case reports of JTA accompany- ing KD, in which JTA either preceded [2] or developed at the same time with KD [3-5]. One case was old age JTA, and KD developed as retroauricular mass in 3 years later after JTA excision [2]. The other three cases were JTA, which co-existed with neighboring KD lesions at the con- current periarterial specimen [3-5]. These features sug-
gested that JTA is a manifestation of KD, which is further supported by the present case.
In contrast to classic temporal arteritis, JTA usually in- volves unilateral side. Only four case reports of bilateral involvement of the JTA have been identified up to now [9-12]. Common characteristics of bilateral cases and our case included occurrence at age between 20 and 40 years, male gender, and peripheral blood eosinophilia. The his- tological features and clinical course were not different from those with unilateral involvement. To the best of our knowledge, this is the first case of bilateral JTA associated with KD. Whether JTA is an independent entity or a pre- sentation of KD or angiolymphoid hyperplasia with eosi- nophilia (ALHE) is difficult to define, until now, histo- logic findings have been the key to differentiate these entities. Compared to histologic findings of JTA or KD, ALHE showed vascular proliferation by thick-walled blood vessels lined by epithelioid, hypertrophic endothe- lial cells with vacuolated cytoplasm and vesicular nuclei [7].
The Doppler ultrasound may be a useful imaging tool for JTA. In the Doppler sonographic study of ALHE involving the temporal artery, characteristic findings included the
Na Ri Kim et al.
68 J Rheum Dis Vol. 25, No. 1, January, 2018
“halo” sign reflecting vascular wall edema around the in- volved artery and the sinusoidal blood flow in the lumen [13]. Although the halo sign was suggested as a specific marker for classic temporal arteritis in a recent meta-anal- ysis [14], it should be interpreted in the context of specif- ic clinical settings, such as JTA and ALHE.
In the previously reported JTA lesions, surgical excision was both diagnostic and curative management. The un-excised JTA lesion in the present case, however, was resolved completely after moderate dose corticosteroid therapy, without recurrence. Considering the hypothesis that JTA is a manifestation of KD and the recommended therapeutic options for multiple or recurred KD include corticosteroid and immune-suppressant therapy, medical treatment may be effective for JTA patients with accom- panying KD [6]. Furthermore, in patients of JTA with typ- ical Doppler ultrasound findings, such as the halo sign, medical treatment with corticosteroid may be considered as the first line treatment and the surgical option may be considered only when the disease is refractory to medical therapy. However, surgery may be the first choice for the treatment of single and localized JTA or KD [1,15].
Ethical considerations
The study was approved by the Institutional Review Board (IRB) of the Kyungpook National University Hospital (IRB no. 2011-06-001).
SUMMARY
There is currently no agreement as to whether JTA rep- resents an independent entity or a manifestation of KD, with no established long-term treatment. This is the first case of a bilateral involvement of JTA accompanying KD, which was confirmed by histological and ultrasound eval- uations and supports that JTA is a manifestation of KD.
The un-excised JTA lesion was resolved completely after corticosteroid therapy. Medical treatment with cortico- steroid may be considered as the first line treatment while surgery can be considered for treatment of focal lesions or refractory cases to medical therapy.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
1. Nesher G, Oren S, Lijovetzky G, Nesher R. Vasculitis of the temporal arteries in the young. Semin Arthritis Rheum 2009;39:96-107.
2. Watanabe C, Koga M, Honda Y, Oh-I T. Juvenile temporal arteritis is a manifestation of Kimura disease. Am J Dermatopathol 2002;24:43-9.
3. Brown I, Adkins G, McClymont K. Juvenile temporal arter- itis: a case report. Pathology 2005;37:559-60.
4. Fukunaga M. Juvenile temporal arteritis associated with Kimura's disease. APMIS 2005;113:379-84.
5. Kim MB, Shin DH, Seo SH. Juvenile temporal arteritis with perifollicular lymphoid proliferation resembling Kimura disease. Report of a case. Int J Dermatol 2011;50:70-3.
6. Sun QF, Xu DZ, Pan SH, Ding JG, Xue ZQ, Miao CS, et al.
Kimura disease: review of the literature. Intern Med J 2008;38:668-72.
7. Kolman OK, Spinelli HM, Magro CM. Juvenile temporal arteritis. J Am Acad Dermatol 2010;62:308-14.
8. Durant C, Connault J, Graveleau J, Toquet C, Brisseau JM, Hamidou M. Juvenile temporal vasculitis: a rare case in a middle-aged woman. Ann Vasc Surg 2011;25:384.e5-7.
9. McGeoch L, Silecky WB, Maher J, Carette S, Pagnoux C.
Temporal arteritis in the young. Joint Bone Spine 2013;80:324-7.
10. Bollinger A, Leu HJ, Brunner U. Juvenile arteritis of ex- tracranial arteries with hypereosinophilia. Klin Wochenschr 1986;64:526-9.
11. Lie JT. Bilateral juvenile temporal arteritis. J Rheumatol 1995;22:774-6.
12. Fujimoto M, Sato S, Hayashi N, Wakugawa M, Tsuchida T, Tamaki K. Juvenile temporal arteritis with eosinophilia: a distinct clinicopathological entity. Dermatology 1996;192:
32-5.
13. Arnander MW, Anderson NG, Schönauer F. The ultrasound halo sign in angiolymphoid hyperplasia of the temporal artery. Br J Radiol 2006;79:e184-6.
14. Arida A, Kyprianou M, Kanakis M, Sfikakis PP. The diag- nostic value of ultrasonography-derived edema of the tem- poral artery wall in giant cell arteritis: a second meta-analysis. BMC Musculoskelet Disord 2010;11:44.
15. Dai L, Wei XN, Zheng DH, Mo YQ, Pessler F, Zhang BY.
Effective treatment of Kimura's disease with leflunomide in combination with glucocorticoids. Clin Rheumatol 2011;
30:859-65.