82
통신저자:심 종 섭
서울시 강남구 일원동 50
성균관대학교 의과대학 삼성서울병원 정형외과학교실 Tel:02-3410-2991ㆍFax:02-3410-0061
E-mail:[email protected]
Address reprint requests to:Jong Sup Shim, M.D.
Department of Orthopaedic Surgery, Samsung Medical Center, Sung- kyunkwan University School of Medicine, 50, Irwon-dong, Gangnam-gu, Seoul 135-710, Korea
Tel:82-2-3410-2991ㆍFax:82-2-2-3410-0061 E-mail:[email protected]
소아 상완골 과상부 골절의 최신 치료 경향 (Recent Trends in Treatment of Supracondylar
Fracture of Distal Humerus in Children)
이 순 철ㆍ심 종 섭
성균관대학교 의과대학 삼성서울병원 정형외과학교실
서 론
소아 상완골 과상부 골절은 주관절 부위 골절 중 가장 흔하며, 약 50∼70%를 차지하고 있고, 7세 이하 소아에서 발생하는 전체 골절 중 30%에 이른다9,10,12,20,59)
. 원위 상완 골에 굴곡력이나 신전력이 가해지며 발생하게 되는데, 손 을 뻗은 상태로 넘어지며 과도한 신전력이 가해져 원위 골 편이 후방으로 전위되는 경우가 95∼98%를 차지한다24). Gartland에 의해 제시된 분류법이 가장 흔히 사용되는데, 이는 시상면상 피질골의 손상 (breakage) 유무와 전위의 정도에 따라 3가지 유형으로 분류한 것이다. 훗날 Wilkins 에 의해 전이의 방향에 따른 분류가 추가되었고 Mubarak 과 Davids는 1형 골절을 전위가 없는 경우 1a로 내측 피 질골의 지주가 감입되어 있고 시상면상 경도의 과신장 변 형을 보이는 경우 1b로 재분류하였다. 최근 Leitch 등37)은 다방향에서 불안정성 (multidirectional instability)을 보이는 4형 골절을 제시하였으나, 아직 일반적으로 통용되고 있지 는 않다. 치료 방법은 골절의 분류에 따라 나누어질 수 있 다. 비 전위 골절의 경우, 부목 또는 견인 치료가 사용될 수 있고, 전위 골절의 경우 흔히 도수 정복 후 핀 고정 술 을 이용하여 치료한다. 한 연구에 의하면 숙련되지 않은 술자에 의해 치료받을 경우 약 17%에서 다양한 종류의 합 병증이 발생할 수 있다고 하였다52). 합병증으로는 혈관 및 신경 손상, 핀 주위의 감염, Volkmann 씨 허혈성 구축, 부 정 유합에 의한 내반주, 관절 강직, 화골성 근염 (myositis ossificans) 등이 있는데, 이를 최소화하기 위해 다양한 치 료 방법들이 최근까지 활발히 연구되어 왔다. 하지만 핀
고정 방법과 혈류 장애를 보이는 골절의 처치 방법에 대해 서는 아직도 이견이 있다51). 이에 저자는 소아 상완골 과 상부 골절의 최신 치료 경향에 소개하고자 한다.
치료 원칙
1. 술 전 처치
방사선 사진 시행 전 검진상 종창이 심하다면 20∼40도 정도만 굴곡시킨 상태로 붕대를 느슨하게 감아 장상지 부 목을 시행하여, 구획 내 압력이 올라가지 않도록 한다. 수 상 받은 상지는 반드시 거상시키도록 한다. 방사선 사진상 심한 전위를 보이는 골절이 발견된다면, 혈관 및 신경 손 상의 가능성이 있기 때문에 도수 정복을 시도하여 골절 부 위를 수술 전까지 어느 정도 안정시키는 것이 좋다.
2. 치료 방법
1) 부목고정
전위가 없는 골절일 경우 장 상지 석고 고정을 통해 치 료할 수 있으며, 골절 유합까지는 약 3주가 소요되고, 고정 후 수일 뒤 종창이 가라앉으면 석고 고정이 헐거워질 수 있기 때문에 교체해 주어야 한다.
2) 견인 치료
이는 장기간 입원해야 하며, 환자의 거동이 불가능하다.
핀 고정 술이 상대적으로 입원기간도 짧고, 수술 결과 역 시 견인 치료보다 좋기 때문에 최근에는 거의 이용되지 않
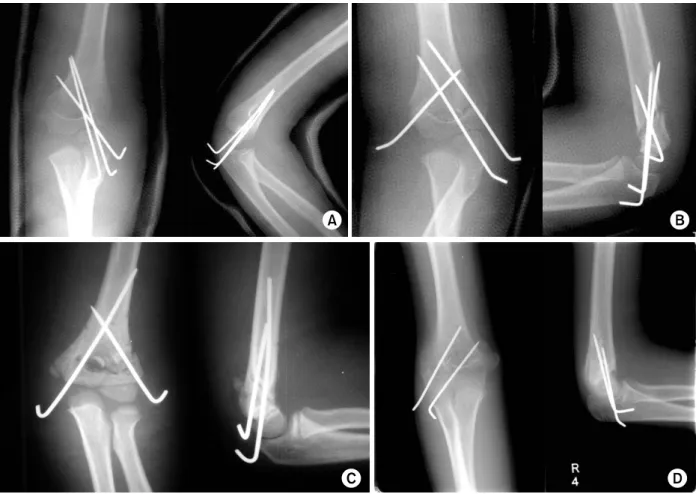
Fig. 1. Various techniques of pin fixation.
(A) Three lateral pains (AP and Lat view).
(B) Crossed and divergent three pins (AP and Lat view).
(C) Crossed two pains (AP and Lat view).
(D) Divergent two pins (AP and Lat view).
4) 관혈적 정복
내 외측의 연부조직이나 골막이 끼면서 도수적으로 골절 정복이 안될 경우, 혈관 손상이 의심될 경우 혹은 개방성 골절에서 시행될 수 있다. 일반적으로 전내측 도달법이 가
고정 방법은 기본적으로 내측 핀 고정술 시행여부에 따 라 크게 두 가지 방법으로 나뉜다 (Fig. 1). 이는 아직도 논란의 여지가 있는데, 외측에만 핀 고정한 경우와 내 외 측에 교차하여 핀 고정한 경우를 비교한 다양한 연구들이 있다6). 생역학적으로 내 외측에서 교차하여 핀 고정술을
Fig. 2. The medical photo which was taken immediately after operation shows the pin is exposed.
Fig. 3. Pucker sign, one of the spikes from the proximal fragment penetrates the dermal layer. This “pucker sign” is an alert to the fact that the fracture may be difficult to reduce by closed manipulation or traction46).
시행하였을 때, 축 회전 (axial rotation)에 대해 더 안정적 이라고 알려져 있다. 하지만 내측 핀 고정술 시 의인성 척 골 신경 손상이 1∼6% 정도에서 발생할 수 있기 때문에 주의해야 한다2,25,64).
최근 연구들에 의하면 외측에만 핀 고정을 하여 내 외측 핀 고정만큼 양호한 결과를 얻었으며 신경 손상을 줄일 수 있었다고 발표되었다4,16,29,34,35,49,55,75)
. 고정하는 핀 개수에 대해 Sankar 등58)은 Gartland 3형 골절에서 두 개의 외측 핀만을 이용하여 고정할 경우 핀 고정 소실 (loss of pin fixation)이 2.9%에서 발생하였지만, 세 개의 외측 핀을 이 용했을 경우는 발생하지 않았다고 발표하였다. 최적의 핀 위치에 대해 생역학적 분석을 시행한 결과, 세 개의 핀 중 두 개는 서로 다른 (divergent) 방향으로 삽입되어야 하는데, 하나는 외측 피질골에 평행한 방향으로 삽입되고, 다른 하 나의 핀은 구상돌기와 (갈고리 오목, coronoid fossa)의 내측 끝부분 (medial edge level)에서 골절 부위 (fracture site)를 통과하여 삽입될 때 가장 고정력이 강하다는 연구가 있다19). 내측 핀 고정에 대해 Zenios 등77)은 두 개의 외측 핀을 이용하여 고정한 이후 투시촬영 (fluoroscopy)을 이용하여 내 회전, 외 회전시킬 때 골절부위의 안정성이 있는지를 확인하고, 불안정하다고 판단될 경우 외측에 1개의 핀을 추가적으로 고정하고, 이후에도 불안정 할 경우에는 내측 에 핀 고정을 한다고 하였다. 반면에 Shim과 Lee60)는 3형 골절의 경우 불안정하기 때문에 내 외측에 핀 고정을 해야 하며, 이때 우선 외측에 두 개의 핀 고정을 한 이후 어느 정도 안정성을 확보해서 주관절을 신전시킨 상태로, 내측 핀을 삽입하여 척골 신경을 보호하도록 해야 한다고 하였
다35). 또한 내측 피질골의 분쇄 골절이 심한 경우 외측 핀 고정이 제한될 수 있기 때문에 내측에도 핀 고정을 해야 한다70).
내측 핀 고정에 의한 척골 신경 손상을 막기 위한 방법 으로 핀 삽입 시 신경을 촉지하여 아래로 밀어주거나, 최소절 개 (miniopen)하는 방법17) 혹은 신경 자극기 (nerve stimu- lator)를 이용하는 방법 등이 있으나, 술 중 신경 손상이 없었다고 해도, 술 후 박혀 있는 핀에 의해 신경이 자극받 을 수도 있다는 점을 염두해 두어야 한다70).
핀 고정을 끝냈다면 핀은 피부 밖으로 노줄해 놓는 것이 일반적이며, 외래에서 제거하기 용이하게 충분히 밖으로 노출해 놓아야 한다 (Fig. 2).
3. 수술 시기
최근 연구에 의하면 대부분의 경우 촉각을 다툴 만큼 응 급수술이 필요한 것은 아니다8). 수상 후 12시간 이상 경과 한 후 수술하여도 결과에 차이가 없다는 후향적 연구가 있 었다18,23,36,48,61)
. 하지만 Ramachandran 등56)에 의하면 22시 간 이상 경과한 후 수술한 경우, 구획 증후군의 발생이 유 의하게 더 높았다고 하였다. 또한 Gartland 3형 환자만을 대상으로 조사한 한 연구에 의하면 12시간 이후에 수술한 군에서 더 불량한 결과를 보였다는 연구가 있다41). 따라서 환자가 내원하였을 때 연부 조직의 부종 정도 및 혈류의 상태를 파악하여, 개방성 골절, 구획 증후군 발생가능성이 높은 경우로 맥박이 없거나 동맥 손상이 의심되는 경우 (특히 제3b형 골절로 원위골편이 후외방 전위되어 근위골 편이 상완 동맥이나 정중 신경을 누르고 있을 경우) 혹은
Fig. 4. (A) At postoperative 3 months, plain radiograph of the elbow joint showed myositis ossificans, (B) which resolved spontaneously after 1 year.
Fig. 5. Undisplaced supracondylar fracture of distal humerus, Gartland type 1a shows the posterior fat pad sign (AP and Lat view).
상완근 등의 연부조직이 감입된 주름 징후 (pucker sign) 등이 보일 경우라면 응급치료가 필수적이고, 그 외의 경 우에도 가능한 조기에 수술을 시행하는 것이 좋겠다 (Fig.
3)42,72).
4. 술 후 처치
핀 고정술 후 주관절 부위 부종이 심하거나, 동맥손상으 로 인한 혈류 확인 등이 필요할 경우 부목 고정 후 석고붕 대 고정으로 환원할 수도 있으나, 대부분의 경우 처음부터 80 내지 90도 굴곡 상태에서 석고붕대 고정을 한다. 첫 1주 후에 부종이 감소하여 고정상태가 헐거워지면 석고붕대를 교체하는 것이 좋다. 전위가 심한 골절, 특히, 동맥압이 소 실된 경우라면 석고붕대 고정을 80도 굴곡 또는 그 이하에 서 고정하는 것이 좋다. 3∼4주 뒤 방사선 사진상 신생골 (periosteal new bone)이 관찰되면, 핀을 제거한다. 일반적 으로 소아의 경우 물리 치료는 필요 없으며, 관절 운동 시 작 후 3∼5주까지 일상 생활이 가능한 정도의 운동 범위를
회복한다27,73). 이후 술 후 1년 정도까지 서서히 운동 범위
가 증가하게 되며, 나이가 어릴수록 회복이 빠르다66,78). 개 방성 골절, 대뇌손상 등이 동반된 경우 골절 주위 화골성 근염의 발생이 쉬우므로 관절 운동 회복을 위한 수동적 운 동은 금지하는 것이 좋다 (Fig. 4)28).
골절 유형에 따른 처치
1. 1a형 골절 (Fig. 5)
이는 비전위 골절을 의미하는 것으로, 골절은 수상 당시
에 진단을 못하고, 수주 뒤 다시 확인한 방사선 사진상 골 막 반응을 통해 후향적으로 진단이 되는 경우도 있다. 따 라서 정확한 진단이 중요한데, 환자가 종창 및 명확한 압 통이 있을 경우, 지방체 징후 (fat pad sign)가 있다면 이 는 관절 내 혈 관절증 (hemarthrosis)이 있다는 것을 의미하 기 때문에 골절 진단에 도움이 될 수 있다 (Fig. 5). 지방 체 징후는 관절의 전방과 후방에 나타날 수 있는데, 전방 은 정상에서도 보일 수 있는 반면에 후방은 주관절을 90도 굴곡시 정상적으로는 관찰되지 않기 때문에, 후방의 지방체 징후 유무를 자세히 관찰해야 한다. Skaggs와 Mirzayan62)은 주관절 후방에 지방체 징후가 관찰된 환자 중 76%에서 골 절이 있었으며, 이 중 절반은 상완골 과상부 골절이었다고 하였다.
Fig. 6. In Gartland type 1b, supracondylar fracture of distal humerus, medial cortex is impacted and treated operatively.
(A) Preoperative AP view, (B) Preoperative Lat view, (C) Postoperative AP view, (D) Postoperative Lat view.
Fig. 7. Gartland type 2, supracondylar fracture of distal humerus has the intact posterior cortex (AP and Lat view).
또한 환자의 나이에 따라 성장판 모양으로 인해 골절선 의 확인이 어려운 경우가 있기 때문에, 반드시 반대쪽 주 관절 방사선 사진을 확인해야 한다24). 주관절 부위의 골 화는 상완골 소두, 요골두, 내상과, 활차, 주두, 외상과 순 으로 진행되며, 소두의 골화가 2세경에 시작되며 나머지 골화 중심이 약 2년 간격으로 나타난다는 것을 숙지하고 있다면 진단에 도움이 될 것이다. 1a형 골절의 경우 진단 이 되었다면 치료에 대해서는 이견이 별로 없다. 대부분 의 경우 석고붕대 고정만으로 쉽게 치료된다. 이때 주관 절을 90∼110도로 굴곡시키고, 전완부를 중립 위치로 장 상지 부목 고정을 하게되는데, 고정 후 반드시 혈류장애 여부를 확인해야 한다. 종창이 심하다면 주관절 굴곡을 줄인 상태로 부목 고정을 실시한다. 수일 뒤 종창이 가라 앉으면 장상지 석고고정을 하고, 골절 유합까지는 약 3∼
4주가 소요된다.
2. 1b형 골절 (Fig. 6)
이 골절은 그대로 고정할 경우 내측 피질골 지주의 감입 에 의해 내반 변형이 발생할 수 있기 때문에, 반드시 내반 변형을 교정한 후 경피적 핀 고정술을 시행해야 한다.
3. 2형 골절 (Fig. 7)
후방 피질골은 유지되고 있는 골절 형태이다. 흔히 과신 전 형태의 골절을 보이고, 관상면상 전이는 거의 관찰되지 않는다. 수술 시행 여부에 대해 논란이 있지만 원위 상완 골은 재형성이 거의 안되는 부위이기 때문에 해부학적 정 복이 안될 경우 수술이 필요하다. Camus 등7)은 155명의 Gartland 2형 소아 상완골 과상부 골절 환자들을 대상으로 도수정복 후 석고 고정만을 실시한 결과 80%의 환자에서 신전 변형이 남아 있었다고 하였고 Skaggs 등63)도 역시 수 술을 통해 정복 후 핀 고정술을 실시할 것을 권장하였다.
4. 3형 골절 (Fig. 8)
완전 전위를 보이는 골절로써, 신경 및 혈관 손상의 가 능성이 높으므로 가능하면 조기에 정복을 시행하여야 한 다. 도수정복이 만족스럽지 못할 경우 다른 방법으로 3∼5 mm 정도의 작은 절개를 만들고, S-pin이나, mosquito 집 게를 이용하여 지렛대 원리를 이용해 정복을 시도할 수 있
다34,35,39). Hur 등22)은 전방에 최소 절개를 만들고, 술자의
무지를 이용해 정복을 시도하여 좋은 결과를 발표하였고, Parmaksizolgu 등54)은 근위 골절편에 K 강선을 이용해 고 정한 후 정복하는 joystick 방법을 소개하였다.
Fig. 8. Completely displaced Gartland type 3, supracondylar fracture of distal humerus treated with closed reduction and percutaneous pinning.
(A) Preoperative AP view, (B) Preoperative Lat view, (C) Postoperative AP view, (D) Postoperative Lat view.
Fig. 9. Flexion type, supracondylar fracture of distal humerus treated with open reduction and pinning.
(A) Preoperative AP and Lat view, (B) Postoperative AP and Lat view.
5. 굴곡형 골절 (Fig. 9)
드물게 발생하는 골절로, 주관절 후방부에 과도한 압력 을 받아 발생한 굴곡력에 의해 원위 골편이 전방 전위된 다. 19% 정도의 환아에서 술 전에 이미 척골 신경의 손상 이 있을 수 있으니, 주의해야 한다. 치료 역시 까다로운데, 가능하면 도수정복 후 경피적 핀고정술을 하는 것이 좋으 나, 신전형 골절에 비해 관혈적 정복을 시행해야 하는 경 우가 더 많다15,68). Mahan 등44)에 의하면 Gartland 3형 골 절 중 신전형에서는 11%만 개방성 정복이 필요했으나, 굴 곡형에서는 39%에서 필요했다고 하였다. 관혈적 정복은 후 내측 도달법을 주로 이용한다.
특수한 상황에서의 치료
1. 혈관 손상 (Fig. 10)
혈관 손상은 약 1%의 환아들에게서 발생한다59). 원위부 골편이 후 외방 전위되며 상완 동맥이 손상되는 경우가 가 장 흔하다. 술 전에 촉지되지 않았던 맥박이 적절한 골절 정복 후에도 계속 촉지되지 않는 경우가 있다. 이때 이환 된 상지의 혈액 순환이 괜찮다면 경과 관찰하는 것만으로 충분하다는 의견이 있는 반면 White 등은 수술을 통해 확 인한 결과, 단순 혈관 경련 (spasm)에 의한 경우는 9%였 고, 상완 동맥 손상이 70%에서 발견되었기 때문에 color flow doppler 등의 비침습적인 검사를 이용하여, 적극적인
Fig. 11. Volkmann’s ischemic contracture.
(A) 5 days after supracondylar fracture compartment syndrome is developed.
(B) Volkmann’s ischemic con- tracture
Fig. 10. CT angiogram of 5 year-old aged boy of left supra- condylar fracture. The contrast media doesn’t pass the left brachial artery (Arrow).
진단 및 치료가 필요하다고 하여 아직도 논란의 여지가 있
다30,57,74). 하지만 술 전에 촉지되었던 맥박이 술 후 촉지되
지 않을 경우 (골절 정복하며 골절편 사이에 동맥이 끼면 서 손상됨을 의미함), 상지의 허혈성 장애가 의심되는 경 우, 혹은 심한 통증을 호소할 경우 혈류 손상에 대해 수술 을 통해 확인하여 Volkmann씨 허혈성 구축을 예방하여야 한다 (Fig. 11)5).
2. 신경 손상
2010년 Babal 등2)은 5,148명의 소아 과상부 골절 환자 들을 대상으로 meta-analysis를 시행하여, 신전형에서 12.7%, 굴곡형에서는 16.6%의 신경좌상 (neuropraxia)이 발생했으며, 신전형에서 전 골간 신경의 손상이 가장 흔하 였고, 굴곡형에서는 척골 신경의 손상이 가장 흔하다고 하
였다. 수술 시 발생할 수 있는 의인성 신경 손상에 대해 총 3.9%에서 발생하였으며, 외측 핀 고정술 시 3.4%에서 정중 신경 혹은 요골 신경의 손상이 발생하였고, 내측 핀 고정술 시 4.1%에서 척골 신경 손상이 발생하였다고 발표 하였다. 이러한 신경 손상의 경우 대부분에서 별다른 처치 없이 호전되는데, 의인성 척골 신경 손상의 경우 대부분에 서 별다른 처치 없이 7개월 이내에 완전 회복되며, 2개월 이내에 감각이 돌아오고, 운동 신경은 평균 5.4개월의 회복 시간이 필요하다25). 또한 정중 신경 혹은 전 골간 신경 손 상이 있을 경우는 동반하여 상완 동맥의 손상도 함께 있을 수 있기 때문에 주의하여야 한다45).
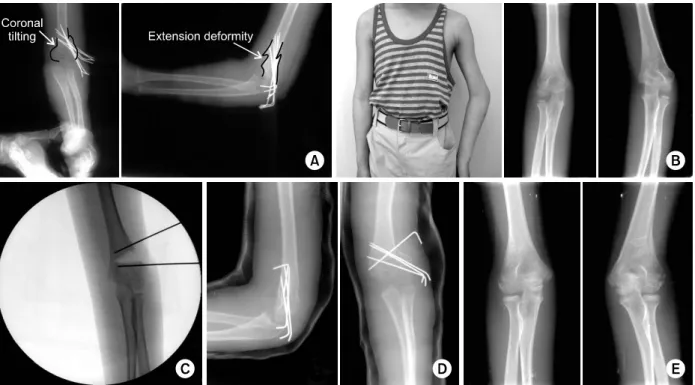
3. 내반주 변형 (Fig. 12)
소아 상완골 과상부 골절에서 가장 흔한 합병증으로, 원 인은 거의 대부분 골절 정복 및 유합 시의 부정 유합이다.
하지만 성장장애에 의한 경우도 드물게 보고되고 있다47,69). 대부분의 내반주 변형은 골절 부분의 내측 감입 (coronal tilting), 내회전 변형, 신전 변형이 동반된다.
발생된 내반주 변형은 진행되어 악화되지도 않고, 저절 로 교정되지도 않는다. 대부분의 문제는 미용적인 외형적 인 문제이다. 그러나, 근력약화나 외과골절 등의 기능적 문 제를 일으킬 수 있다. 특히 신전 변형이 동반된 경우, 이 를 치료하지 않을 경우 굴곡운동 제한 및 과신전 장애가 교정되지 않는다.
치료는 교정 절골술이다. 경과 관찰하더라도 변형의 호 전을 기대할 수는 없기 때문에, 교정 수술 후 신속한 회복 을 원한다면, 성인이 될 때까지 기다리는 것보다는 성장기 소아시기에 실시하는 것이 좋다.
수술 방법은 외측 폐쇄성 절골술, 내측 개방성 절골술, pentalateral 절골술, dome 절골술 등의 다양한 방법들이 있다11,33,43,50,53,76)
. 이 중 외측 폐쇄성 절골술은 가장 널리 알려진 방법인데 외측 원위부 골편이 돌출되는 단점이 있 다. 하지만 소아의 경우 재형성되며 점차 호전되기 때문에
Fig. 12. Cubitus varus.
(A) The 6 year-old aged patient who suffered supracondylar fracture of distal humerus was treated with closed reduction and percutaneous pinning. Immediate postoperative plain radiogram shows the coronal tilting and extension deformity (AP and Lat view).
(B) He developed cubitus varus. (Left) Medical photo. (Right) Plain radiopraphy of both elbow AP view.
(C) Corrective osteotomy with using lateral closing wedge osteotomy is performed.
(D) Immediate postop plain radiography shows the prominence of lateral condyle of distal humerus.
(E) At postoperative 3 years, the lateral prominence is decreased by remodeling.
대부분 좋은 결과를 보인다3). 이 방법은 수술이 간단하며 피부 절개 부위가 적고, 내측 골막 또는 피질골을 지렛대 로 이용하여 절골하기 때문에 절골 부위가 안정적이다. 따 라서 금속 핀으로 고정하여도 충분한 고정력을 얻을 수 있 다. 그러나, 청소년기 또는 성인에서는 외측 원위부 골편의 돌출이 미용적으로 흉하고 돌출된 부위가 재형성되지 않기 때문에, pentalateral 절골술, dome 절골술, translation step-cut 절골술, reverse V 절골술 등이 사용되며 금속판 또는 체외고정 장치 등 다양한 고정 기구를 이용할 수 있 다21,38,40).
결 론
상완골 과상부 골절은 소아에게 가장 흔하게 발생하는 골절로써, 다양한 합병증이 발생할 수 있으며, 가능하면 조 기에 골절 부위를 안정화해 주어야 한다. Gartland 1형 골 절의 경우 비수술적으로 치료가 가능하지만, 1b형의 경우 내반 변형의 발생이 가능하기에 주의를 요한다. 2형 및 3
형은 대부분 수술적 치료를 요하는데, 가능하면 도수정복 을 하고, 핀 고정을 해야 한다. 이때 일반적으로 외측에만 핀 고정을 하면 되나, 일부의 골절에서는 내측의 핀 고정 술이 추가적으로 필요할 수 있다. 내측 핀 고정은 척골 신 경의 손상에 주의하여야 한다. 술 후 혈류 장애에 대한 치 료는 아직 논란의 여지가 있으나, 구획증후군이 의심될 경 우 즉시 수술적으로 확인해 보아야 한다. 내반주 변형은 부정 유합에 의해 발생하는데, 재형성되지 않기 때문에 심 할 경우 수술로 교정해야 한다.
참 고 문 헌
1) Aktekin CN, Toprak A, Ozturk AM, Altay M, Ozkurt B, Tabak AY: Open reduction via posterior triceps spar- ing approach in comparison with closed treatment of post- eromedial displaced Gartland type III supracondylar hume- rus fractures. J Pediatr Orthop B, 17: 171-178, 2008.
2) Babal JC, Mehlman CT, Klein G: Nerve injuries asso-
ciated with pediatric supracondylar humeral fractures: a meta-analysis. J Pediatr Orthop, 30: 253-263, 2010.
3) Barrett IR, Bellemore MC, Kwon YM: Cosmetic results of supracondylar osteotomy for correction of cubitus varus. J Pediatr Orthop, 18: 445-447, 1998.
4) Belhan O, Karakurt L, Ozdemir H, et al: Dynamics of the ulnar nerve after percutaneous pinning of supra- condylar humeral fractures in children. J Pediatr Orthop B, 18: 29-33, 2009.
5) Blakey CM, Biant LC, Birch R: Ischaemia and the pink, pulseless hand complicating supracondylar fractures of the humerus in childhood: long-term follow-up. J Bone Joint Surg Br, 91: 1487-1492, 2009.
6) Brauer CA, Lee BM, Bae DS, Waters PM, Kocher MS: A systematic review of medial and lateral entry pin- ning versus lateral entry pinning for supracondylar frac- tures of the humerus. J Pediatr Orthop, 27: 181-186, 2007.
7) Camus T, MacLellan B, Cook PC, Leahey JL, Hyndman JC, El-Hawary R: Extension type II pediatric supracondylar humerus fractures: a radiographic outcomes study of closed reduction and cast immobilization. J Pediatr Orthop, 31: 366-371, 2011.
8) Carmichael KD, Joyner K: Quality of reduction versus timing of surgical intervention for pediatric supracondylar humerus fractures. Orthopedics, 29: 628-632, 2006.
9) Cheng JC, Shen WY: Limb fracture pattern in different pediatric age groups: a study of 3,350 children. J Orthop Trauma, 7: 15-22, 1993.
10) de las Heras J, Durán D, de la Cerda J, Romanillos O, Martinez-Miranda J, Rodriguez-Merchan EC: Supra- condylar fractures of the humerus in children. Clin Orthop Relat Res, (432): 57-64, 2005.
11) Devnani AS: Lateral closing wedge supracondylar osteot- omy of humerus for post-traumatic cubitus varus in children. Injury, 28: 643-647, 1997.
12) Farnsworth CL, Silva PD, Mubarak SJ: Etiology of su- pracondylar humerus fractures. J Pediatr Orthop, 18:
38-42, 1998.
13) Fu D, Xiao B, Yang S, Li J: Open reduction and bio- absorbable pin fixation for late presenting irreducible su- pracondylar humeral fracture in children. Int Orthop, 35:
725-730, 2011.
14) Gadgil A, Hayhurst C, Maffulli N, Dwyer JS: Elevated, straight-arm traction for supracondylar fractures of the hu-
merus in children. J Bone Joint Surg Br, 87: 82-87, 2005.
15) Garg B, Pankaj A, Malhotra R, Bhan S: Treatment of flexion-type supracondylar humeral fracture in children. J Orthop Surg (Hong Kong), 15: 174-176, 2007.
16) Gaston RG, Cates TB, Devito D, et al: Medial and lat- eral pin versus lateral-entry pin fixation for Type 3 supra- condylar fractures in children: a prospective, surgeon- randomized study. J Pediatr Orthop, 30: 799-806, 2010.
17) Green DW, Widmann RF, Frank JS, Gardner MJ:
Low incidence of ulnar nerve injury with crossed pin placement for pediatric supracondylar humerus fractures using a mini-open technique. J Orthop Trauma, 19: 158- 163, 2005.
18) Gupta N, Kay RM, Leitch K, Femino JD, Tolo VT, Skaggs DL: Effect of surgical delay on perioperative complications and need for open reduction in supra- condylar humerus fractures in children. J Pediatr Orthop, 24: 245-248, 2004.
19) Hamdi A, Poitras P, Louati H, Dagenais S, Masquijo JJ, Kontio K: Biomechanical analysis of lateral pin placements for pediatric supracondylar humerus fractures.
J Pediatr Orthop, 30: 135-139, 2010.
20) Hanlon CR, Estes WL Jr: Fractures in childhood, a stat- istical analysis. Am J Surg, 87: 312-323, 1954.
21) Horstmann HM, Blyakher AA, Quartararo LG, Cavalier R: Treatment of cubitus varus with osteotomy and Ilizarov external fixation. Am J Orthop (Belle Mead NJ), 29: 389-391, 2000.
22) Hur CR, Suh SW, Oh CU, et al: Minimally invasive an- terior approach in open reduction of displaced supra- condylar fractures of humerus in children. J Korean Fracture Soc, 18: 185-190, 2005.
23) Iyengar SR, Hoffinger SA, Townsend DR: Early versus delayed reduction and pinning of type III displaced supra- condylar fractures of the humerus in children: a com- parative study. J Orthop Trauma, 13: 51-55, 1999.
24) John AH: Tachdjian's Pediatric Orthopaedics. 4th ed.
philadelphia, Saunders: 2451-2476, 2008.
25) Kalenderer O, Reisoglu A, Surer L, Agus H: How should one treat iatrogenic ulnar injury after closed reduc- tion and percutaneous pinning of paediatric supracondylar humeral fractures? Injury, 39: 463-466, 2008.
26) Kazimoglu C, Cetin M, Sener M, Aguş H, Kalanderer O: Operative management of type III extension supracondylar fractures in children. Int Orthop, 33: 1089-1094, 2009.
children. A randomized clinical trial. J Bone Joint Surg Am, 89: 706-712, 2007.
30) Korompilias AV, Lykissas MG, Mitsionis GI, et al:
Treatment of pink pulseless hand following supracondylar fractures of the humerus in children. Int Orthop, 33:
237-241, 2009.
31) Kraus R, Joeris A, Castellani C, Weinberg A, Slongo T, Schnettler R: Intraoperative radiation exposure in dis- placed supracondylar humeral fractures: a comparison of surgical methods. J Pediatr Orthop B, 16: 44-47, 2007.
32) Lacher M, Schaeffer K, Boehm R, Dietz HG: The treat- ment of supracondylar humeral fractures with elastic stable intramedullary nailing (ESIN) in children. J Pediatr Orthop, 31: 33-38, 2011.
33) Laupattarakasem W, Mahaisavariya B: Stable fixation of pentalateral osteotomy for cubitus varus in adults. J Bone Joint Surg Br, 74: 781-782, 1992.
34) Lee HY, Kim SJ: Treatment of displaced supracondylar fractures of the humerus in children by a pin leverage technique. J Bone Joint Surg Br, 89: 646-650, 2007.
35) Lee HY, Song JH: Treatment of pediatric displaced su- pracondylar fractures of the humerus by pin leverage technique. J Korean Fracture Soc, 19: 83-88, 2006.
36) Leet AI, Frisancho J, Ebramzadeh E: Delayed treatment of type 3 supracondylar humerus fractures in children. J Pediatr Orthop, 22: 203-207, 2002.
37) Leitch KK, Kay RM, Femino JD, Tolo VT, Storer SK, Skaggs DL: Treatment of multidirectionally unstable su- pracondylar humeral fractures in children. A modified Gartland type-IV fracture. J Bone Joint Surg Am, 88:
980-985, 2006.
38) Levine MJ, Horn BD, Pizzutillo PD: Treatment of post- traumatic cubitus varus in the pediatric population with humeral osteotomy and external fixation. J Pediatr Orthop,
2009.
42) Louahem DM, Nebunescu A, Canavese F, Dimeglio A:
Neurovascular complications and severe displacement in supracondylar humerus fractures in children: defensive or offensive strategy? J Pediatr Orthop B, 15: 51-57, 2006.
43) Mahaisavariya B, Laupattarakasem W: Osteotomy for cubitus varus: a simple technique in 10 children. Acta Orthop Scand, 67: 60-62, 1996.
44) Mahan ST, May CD, Kocher MS: Operative manage- ment of displaced flexion supracondylar humerus fractures in children. J Pediatr Orthop, 27: 551-556, 2007.
45) Mangat KS, Martin AG, Bache CE: The ‘pulseless pink' hand after supracondylar fracture of the humerus in children: the predictive value of nerve palsy. J Bone Joint Surg Br, 91: 1521-1525, 2009.
46) Marquis C, Cheung G, Dwyer J, Emery D: Supracon- dylar fractures of the humerus. Current Orthopaedics, 22:
62-69, 2008.
47) McKee M: Progressive cubitus varus due to a bony phys- eal bar in a four year old girl following supracondylar fracture: a case report. J Orthop Trauma, 20: 372, 2006.
48) Mehlman CT, Strub WM, Roy DR, Wall EJ, Crawford AH: The effect of surgical timing on the perioperative complications of treatment of supracondylar humeral frac- tures in children. J Bone Joint Surg Am, 83: 323-327, 2001.
49) Memisoglu K, Cevdet Kesemenli C, Atmaca H: Does the technique of lateral cross-wiring (Dorgan's technique) reduce iatrogenic ulnar nerve injury? Int Orthop, 35: 375- 378, 2011.
50) Moon MS, Kim SS, Kim ST, et al: Lateral closing wedge osteotomy with or without medialisation of the distal fragment for cubitus varus. J Orthop Surg (Hong Kong), 18: 220-223, 2010.
51) Omid R, Choi PD, Skaggs DL: Supracondylar humeral fractures in children. J Bone Joint Surg Am, 90: 1121- 1132, 2008.
52) Padman M, Warwick AM, Fernandes JA, Flowers MJ, Davies AG, Bell MJ: Closed reduction and stabilization of supracondylar fractures of the humerus in children: the crucial factor of surgical experience. J Pediatr Orthop B, 19: 298-303, 2010.
53) Pankaj A, Dua A, Malhotra R, Bhan S: Dome osteot- omy for posttraumatic cubitus varus: a surgical technique to avoid lateral condylar prominence. J Pediatr Orthop, 26: 61-66, 2006.
54) Parmaksizoglu AS, Ozkaya U, Bilgili F, Sayin E, Kabukcuoglu Y: Closed reduction of the pediatric supra- condylar humerus fractures: the "joystick" method. Arch Orthop Trauma Surg, 129: 1225-1231, 2009.
55) Queally JM, Paramanathan N, Walsh JC, Moran CJ, Shannon FJ, D'Souza LG: Dorgan's lateral cross-wiring of supracondylar fractures of the humerus in children: A retrospective review. Injury, 41: 568-571, 2010.
56) Ramachandran M, Skaggs DL, Crawford HA, et al:
Delaying treatment of supracondylar fractures in children:
has the pendulum swung too far? J Bone Joint Surg Br, 90: 1228-1233, 2008.
57) Ramesh P, Avadhani A, Shetty AP, Dheenadhayalan J, Rajasekaran S: Management of acute 'pink pulseless' hand in pediatric supracondylar fractures of the humerus. J Pediatr Orthop B, 20: 124-128, 2011.
58) Sankar WN, Hebela NM, Skaggs DL, Flynn JM: Loss of pin fixation in displaced supracondylar humeral frac- tures in children: causes and prevention. J Bone Joint Surg Am, 89: 713-717, 2007.
59) Scherl SA, Schmidt AH: Pediatric trauma: getting through the night. Instr Course Lect, 59: 455-463, 2010.
60) Shim JS, Lee YS: Treatment of completely displaced su- pracondylar fracture of the humerus in children by cross- fixation with three Kirschner wires. J Pediatr Orthop, 22:
12-16, 2002.
61) Sibinski M, Sharma H, Bennet GC: Early versus de- layed treatment of extension type-3 supracondylar fractures of the humerus in children. J Bone Joint Surg Br, 88:
380-381, 2006.
62) Skaggs DL, Mirzayan R: The posterior fat pad sign in association with occult fracture of the elbow in children. J Bone Joint Surg Am, 81: 1429-1433, 1999.
63) Skaggs DL, Sankar WN, Albrektson J, Vaishnav S, Choi PD, Kay RM: How safe is the operative treatment of Gartland type 2 supracondylar humerus fractures in children? J Pediatr Orthop, 28: 139-141, 2008.
64) Slobogean BL, Jackman H, Tennant S, Slobogean GP, Mulpuri K: Iatrogenic ulnar nerve injury after the surgi- cal treatment of displaced supracondylar fractures of the humerus: number needed to harm, a systematic review. J Pediatr Orthop, 30: 430-436, 2010.
65) Slongo T, Schmid T, Wilkins K, Joeris A: Lateral ex- ternal fixation--a new surgical technique for displaced un- reducible supracondylar humeral fractures in children. J Bone Joint Surg Am, 90: 1690-1697, 2008.
66) Spencer HT, Wong M, Fong YJ, Penman A, Silva M:
Prospective longitudinal evaluation of elbow motion fol- lowing pediatric supracondylar humeral fractures. J Bone Joint Surg Am, 92: 904-910, 2010.
67) Srikumaran U, Tan EW, Erkula G, Leet AI, Ain MC, Sponseller PD: Pin size influences sagittal alignment in percutaneously pinned pediatric supracondylar humerus fractures. J Pediatr Orthop, 30: 792-798, 2010.
68) Steinman S, Bastrom TP, Newton PO, Mubarak SJ:
Beware of ulnar nerve entrapment in flexion-type supra- condylar humerus fractures. J Child Orthop, 1: 177-180, 2007.
69) Theruvil B, Kapoor V, Fairhurst J, Taylor GR:
Progressive cubitus varus due to a bony physeal bar in a 4-year-old girl following a supracondylar fracture: a case report. J Orthop Trauma, 19: 669-672, 2005.
70) Tripuraneni KR, Bosch PP, Schwend RM, Yaste JJ:
Prospective, surgeon-randomized evaluation of crossed pins versus lateral pins for unstable supracondylar hume- rus fractures in children. J Pediatr Orthop B, 18: 93-98, 2009.
71) Turhan E, Aksoy C, Ege A, Bayar A, Keser S, Alpaslan M: Sagittal plane analysis of the open and closed methods in children with displaced supracondylar fractures of the humerus (a radiological study). Arch Orthop Trauma Surg, 128: 739-744, 2008.
72) Walmsley PJ, Kelly MB, Robb JE, Annan IH, Porter DE: Delay increases the need for open reduction of type-III supracondylar fractures of the humerus. J Bone Joint Surg Br, 88: 528-530, 2006.
73) Wang YL, Chang WN, Hsu CJ, Sun SF, Wang JL, Wong CY: The recovery of elbow range of motion after
technique. J Bone Joint Surg Am, 90 Suppl 2 Pt 1: Relat Res, 467: 2007-2010, 2009.