ISSN 2234-3806 • eISSN 2234-3814
https://doi.org/10.3343/alm.2017.37.4.343 www.annlabmed.org 343
Ann Lab Med 2017;37:343-345
https://doi.org/10.3343/alm.2017.37.4.343
Letter to the Editor
Clinical Chemistry
Toward Better Predictions of Chemosensitivity:
Comparative Study of Conventional and Simulated Chemosensitivity Tests for Bladder Cancer Cell Lines
Taek Sang Kim, M.D.1, Jae Il Chung, M.D.2, Geun Hwa Noh, M.S.3, and Hyunyong Hwang, M.D.4
Department of Urology1, Kosin University Gospel Hospital, Busan; Department of Urology2, Inje University, Busan Paik Hospital, Busan; Seoul Medical Science Institute3, Seoul; Department of Laboratory Medicine4, Kosin University Gospel Hospital, Busan, Korea
Dear Editor,
The recurrence rate of bladder cancer reaches up to 40–50%, and progression from non-muscle invasive bladder cancer (NM- IBC) to muscle invasive bladder cancer (MIBC) occurs in up to 9.8–13.8% of cases [1]. When bladder cancer progresses to MIBC, radical cystectomy with orthotopic neobladder substitu- tion or urinary diversion is required to improve survival, although this decreases patient quality of life [2].
Intravesical instillation of a chemotherapeutic agent is usually performed in cases of NMIBC to prevent recurrence after trans- urethral resection of the bladder tumor (TURBT) [3]. In moder- ate-risk or high-risk NMIBC patients, successive instillation of an intravesical chemotherapeutic agent once a week for six weeks is usually performed [4-6]. Given that proper selection of che- motherapeutic agents is essential for positive outcomes, chemo- sensitivity tests are required to provide a rationale for drug se- lection. To date, chemosensitivity tests have been based on cell survival assessments after a single treatment at a specific time with various methods. However, these in vitro tests are not ac- cepted as routine tests before chemotherapy [7].
We developed in vitro chemosensitivity tests mimicking the situation of clinical chemotherapy by supporting the survival of a cancer cell line in vitro under treatment with an actual intravesi-
cal chemotherapy schedule.
Mitomycin C, epirubicin, gemcitabine, and docetaxel were used at six concentrations for the chemosensitivity tests in six bladder cancer cell lines: J82, T24, SW780, UM-UC-3, TCCSUP, and HT-1376.
For conventional analysis, cancer cells were seeded in welled plates (5 ×103 cells/well) on day one. The chemotherapeutic agent was administered from a dose of 0 (no drug) to 200% on the second day, and chemosensitivity tests were performed after five days. A negative control (no cells) was included on each evaluation plate. The effects of the drugs on cell viability were tested by using CellTiter 96 aqueous nonradioactive cell prolifer- ation assay kits (Promega Co., Madison, WI, USA). Tests were repeated three times, and the mean values were analyzed. Inhi- bition as a percentage of cancer cells was measured for each plate by using the formula (1-T/C)×100, where T/C=absorbance of cultured cancer cells treated with each test drug/absorbance of cultured cells not treated with the test drug.
Simulation of intravesical chemotherapy was performed ac- cording to an in vivo schedule. Chemotherapy was performed once a week in cells in plate wells for two hrs for six weeks (six cycles). The medium containing the chemotherapeutic agent was removed, and fresh medium was added to the wells; two-
Received: August 29, 2016 Revision received: January 31, 2017 Accepted: March 17, 2017
Corresponding author: Hyunyong Hwang
Department of Laboratory Medicine, Kosin University College of Medicine, 262 Gamcheon-ro, Seo-gu, Busan 49267, Korea
Tel: +82-51-990-6371, Fax: +82-51-990-3010 E-mail: [email protected]
© Korean Society for Laboratory Medicine.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
1 / 1 CROSSMARK_logo_3_Test
2017-03-16 https://crossmark-cdn.crossref.org/widget/v2.0/logos/CROSSMARK_Color_square.svg
Kim TS, et al.
Conventional and simulated chemosensitivity tests
344 www.annlabmed.org https://doi.org/10.3343/alm.2017.37.4.343 thirds of the medium was replaced every two days until the next
cycle of chemotherapy. Five days after the last chemotherapy treatment at the sixth week, cell survival was measured to evalu- ate chemosensitivity.
To compare the effectiveness of the conventional and simula- tion methods, the ratio of the half-maximal inhibitory concentra- tion (IC50) for a test drug concentration (TDC) from the simulation method to that from the conventional method was calculated.
The IC50 value of each chemotherapeutic agent was compared by the %TDC to calculate the drug with the lowest IC50 concen- tration by the conventional and simulation methods to determine the most sensible chemotherapeutic agent among the tested drugs.
All bladder cancer cell lines were more resistant to epirubicin than to other drugs (Table 1). The IC50 ratio of the conventional method and simulation protocol showed significant differences for mitomycin C and gemcitabine (P =0.003 and P =0.020, re- spectively; Table 1). All tested cancer cell lines were most sensi- tive to mitomycin C by the conventional method (Table 2). In five of six cancer cell lines, sensitivity was highest to gemcitabine by
the simulation method.
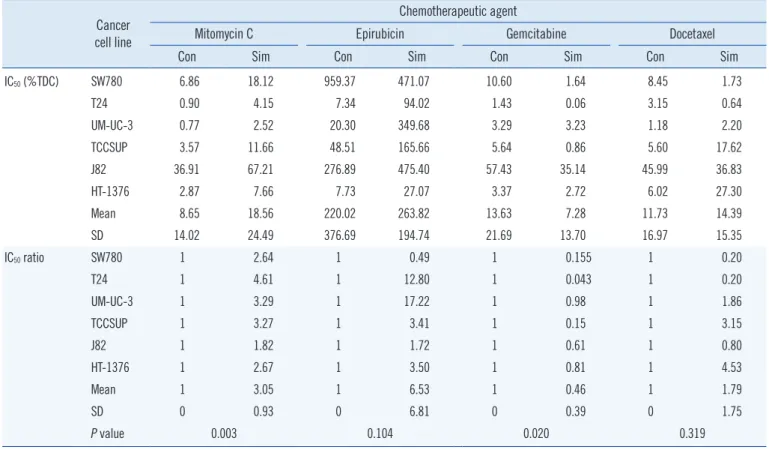
For patients who receive chemotherapy six times per week, one-time chemotherapy in a chemosensitivity test is a completely Table 1. IC50 values by cancer cell line and IC50 ratios for the comparison of conventional and simulation methods
Cancer cell line
Chemotherapeutic agent
Mitomycin C Epirubicin Gemcitabine Docetaxel
Con Sim Con Sim Con Sim Con Sim
IC50 (%TDC) SW780 6.86 18.12 959.37 471.07 10.60 1.64 8.45 1.73
T24 0.90 4.15 7.34 94.02 1.43 0.06 3.15 0.64
UM-UC-3 0.77 2.52 20.30 349.68 3.29 3.23 1.18 2.20
TCCSUP 3.57 11.66 48.51 165.66 5.64 0.86 5.60 17.62
J82 36.91 67.21 276.89 475.40 57.43 35.14 45.99 36.83
HT-1376 2.87 7.66 7.73 27.07 3.37 2.72 6.02 27.30
Mean 8.65 18.56 220.02 263.82 13.63 7.28 11.73 14.39
SD 14.02 24.49 376.69 194.74 21.69 13.70 16.97 15.35
IC50 ratio SW780 1 2.64 1 0.49 1 0.155 1 0.20
T24 1 4.61 1 12.80 1 0.043 1 0.20
UM-UC-3 1 3.29 1 17.22 1 0.98 1 1.86
TCCSUP 1 3.27 1 3.41 1 0.15 1 3.15
J82 1 1.82 1 1.72 1 0.61 1 0.80
HT-1376 1 2.67 1 3.50 1 0.81 1 4.53
Mean 1 3.05 1 6.53 1 0.46 1 1.79
SD 0 0.93 0 6.81 0 0.39 0 1.75
P value 0.003 0.104 0.020 0.319
We calculated the IC50 value for each chemotherapeutic agent for each cancer cell line. All concentrations are presented as the percent test drug concentra- tion (%TDC) and ranged from 0.06% to 959.37%. Paired t-tests were used to analyze the differences in IC50 ratios between the conventional and simulation methods. Differences were significant for mitomycin C and gemcitabine. Statistical significance was established at P <0.05.
Abbreviations: Con, conventional method; Sim, simulation method.
Table 2. Sensitivity ranking for the conventional and simulation methods
Cancer cell line Sensitivity ranking Conventional Simulation
SW780 M>D>G>E G>D>M>E
T24 M>G>D>E G>D>M>E
UM-UC-3 M>D>G>E D>M>G>E
TCCSUP M>D>G>E G>M>D>E
J82 M>D>G>E G>D>M>E
HT-1376 M>G>D>E G>M>D>E
Chemotherapeutic agents were ranked by cell sensitivity for each cell line.
Left, agents to which cells showed the highest sensitivity. All tested cancer cell lines were the most sensitive to mitomycin C when assessed by using the conventional method; however, mitomycin C was ranked second for UM- UC-3, TCCSUP, and HT-1376, and third for SW780, T24, and J82 by using the simulation method.
Abbreviations: M, mitomycin C; G, gemcitabine; D, docetaxel; E, epirubicin.
Kim TS, et al.
Conventional and simulated chemosensitivity tests
https://doi.org/10.3343/alm.2017.37.4.343 www.annlabmed.org 345
different regimen than that for in vitro cancer cells. Although it is impossible to create an environment identical to that of cancer cells in the body, it is important to establish in vitro environments that are as similar as possible to conditions in the body for ac- curately predicting chemosensitivity. We attempted this with our simulation protocols by providing fresh media two hr after che- motherapy and replacing the media every other day. This was assumed to affect the survival of cancer cell lines in the simula- tion protocol.
Although other factors such as pharmacokinetics and phar- macogenomics were not considered, different treatment sched- ules and media replacement in the simulation protocol were be- lieved to cause the observed differences in chemosensitivities.
This study used established bladder cancer cell lines. Addi- tional studies employing in vivo models or cancer cells and clini- cal data from bladder cancer patients are needed to confirm our findings regarding these chemosensitivity methods and the clinical relevance of the newly developed chemosensitivity test.
Authors’ Disclosures of Potential Conflicts of Interest
No potential conflicts of interest relevant to this article were re- ported.
REFERENCES
1. Sylvester RJ, Oosterlinck W, van der Meijden AP. A single immediate postoperative instillation of chemotherapy decreases the risk of recur- rence in patients with stage Ta T1 bladder cancer: a meta-analysis of published results of randomized clinical trials. J Urol 2004;171:2186- 90, quiz 435.
2. Rouprêt M, Babjuk M, Compérat E, Zigeuner R, Sylvester R, Burger M, et al. European guidelines on upper tract urothelial carcinomas: 2013 update. Eur Urol 2013;63:1059-71.
3. O’Brien T, Ray E, Chatterton K, Khan MS, Chandra A, Thomas K. Pro- spective randomised trial of hexylaminolevulinate photodynamic-assist- ed transurethral resection of bladder tumor (TURBT) plus single-shot intravesical mitomycin C vs conventional white-light TURBT plus mito- mycin C in newly presenting non-muscle-invasive bladder cancer. BJU Int 2013;1096-104.
4. van Lingen AV and Witjes JA. Current intravesical therapy for non-mus- cle invasive bladder cancer. Expert Opin Biol Ther 2013;13:1371-85.
5. Koie T, Ohyama C, Hosogoe S, Yamamoto H, Imai A, Hatakeyama S, et al. Oncological outcomes of a single but extensive transurethral resec- tion followed by appropriate intra-vesical instillation therapy for newly diagnosed non-muscle-invasive bladder cancer. Int Urol Nephrol 2015;
47:1509-14.
6. Hayne D, Stockler M, McCombie SP, Chalasani V, Long A, Martin A, et al. BCG+MMC trial: adding mitomycin C to BCG as adjuvant intravesical therapy for high-risk, non-muscle-invasive bladder cancer: a randomised phase III trial (ANZUP 1301). BMC Cancer 2015;15:432.
7. Burstein HJ, Mangu PB, Somerfield MR, Schrag D, Samson D, Holt L, et al. American Society of Clinical Oncology clinical practice guideline update on the use of chemotherapy sensitivity and resistance assays. J Clin Oncol 2011;29:3328-30.