Vol. 20, No. 4, December, 2012
□ 원 저 □소아 전신성 홍반성 낭창 환자에서 신경학적 증상
울산대학교 의과대학 서울아산병원 소아청소년병원 소아청소년과학교실
황선영ㆍ김은희ㆍ최해원ㆍ박영서ㆍ염미선ㆍ고태성
= Abstract =
Neuropsychiatric Manifestations of Childhood Systemic Lupus Erythematosus
Seonyoung Hwang, M.D., Eun-Hee Kim, M.D., Hae-Won Choi, M.D., Young Seo Park, M.D., Mi-Sun Yum, M.D., and Tae-Sung Ko, M.D.
Department of Pediatric Neurology, Asan Medical Center Children’s Hospital University of Ulsan College of Medicine, Seoul, Korea
Purpose : Systemic lupus erythromatosus (SLE) is an autoimmune disease which involves multiple organs, including the central nervous system. Neuropsychiatric (NP) involvement is one of the major causes of morbidity and mortality in children with SLE. The aim of this study was to evaluate neuropsychiatric manifestations and to find the clinical factors associated with the development of NP manifestation in children with SLE (NPSLE).
Methods : We retrospectively reviewed the medical records of 51 patients diagnosed with SLE at Asan Medical Center Children's hospital between April 1998 and January 2011. Clinical factors between patients with NP manifestations and patients without NP manifestations were compared.
Results : NPSLE developed in 41.2% (21/51) of the patients with SLE. The mean age of onset was 13.0 (8-19) years. Twelve patients (57.1%) developed NP manifestations within 1 month after the diagnosis of SLE. NP manifestations included seizures (47.6%), headaches (42.9%), movement disorders (9.5%), peripheral neuropathy/AIDP (9.5%), stroke/TIA (9.5%), psychosis (4.8%). As comparing clinical factors, hematological profile and immunologic profile between patients with NP manifestations and patients without NP manifestations, there were no significant differences between the two groups.
Conclusion : NP symptoms are common in children with SLE, especially within 1 month after the diagnosis of SLE. However, there were no clinical factors or laboratory profiles that may predict the development of NPSLE. Therefore, careful monitoring of NP manifestations may be important in children with newly-diagnosed SLE and prompt immunomodulatory treat- ment should be considered.
Key Words : Neuropsychiatric; SLE; Autoimmune diseases of the Nervous system; Child;
Immunomodulation
1)
접수 : 2012년 11월 30일, 수정 : 2012년 12월 23일 승인 : 2012년 12월 28일
책임저자 : 고태성, 울산대학교 서울아산병원 소아청소년과 Tel : 02)3010-3386 Fax : 02)473-3725 E-mail : tsko@amc.seoul.kr
서 론
전신성 홍반성 낭창(SLE)은 여러 장기를 침범하 여 염증과 조직 손상을 일으키는 자가면역질환이다.
특히 신경학적 증상을 보이는 전신성 홍반성 낭창 (Neuropsychiatric SLE, NPSLE) 환자는 전체 환
자의 15-91%에서 볼 수 있으며 일반적으로 신경학 적 증상은 전신성 홍반성 낭창의 증상 재발 및 사망 에 중요한 영향을 미치는 불량 예후인자로 보고되어
왔다1, 2). 소아에서는 성인에 비해 연구된 바는 적으
나 후향적 연구를 통해 신경학적 증상을 보이는 전 신성 홍반성 낭창의 유병률이 22-43%에 이른다고 보고되고 있다3-5). 소아에서의 신경학적 증상을 보 이는 전신성 홍반성 낭창의 원인과 병리기전 그리고 임상경과에 대해서는 아직까지 잘 알려지지 않았으 나 성인과는 다른 증상, 임상 경과 및 면역학적 결과 등을 보인다고 보고되고 있다6).
최근 검사 방법의 발달 등으로 소아 전신성 홍반 성 낭창의 발생 빈도가 증가추세를 보이고 있는 데 반해 앞서 밝힌 바와 같이 신경학적 증상을 보이는 전신성 홍반성 낭창은 진단 기준이 명확하지 않고 병인에 대해서도 확실히 밝혀진 바 없어 진단과 분 류에 어려움이 있다. 다만 대부분의 연구에서 신경 학적 증상의 발생기전을 자가항체나 염증 사이토카 인 등과 관련하여 자가면역 항체와 항원/항체 복합 체의 형성으로 발현되는 것으로 추정하고 있다6, 7).
저자들은 전신성 홍반성 낭창 환자에서 신경학적 증상의 발현 가능성을 초기 임상 증상 및 자가 면역 항체를 포함한 혈청학적 인자 등의 차이를 통해 예 측할 수 있다면, 이를 예후 예측과 치료에 반영할 수 있을 것으로 기대하였다. 이에 신경학적 증상을 보 인 환자군과 그렇지 않은 환자군 사이에서 전신성 홍반성 낭창 진단기준, 임상 양상, 자가 면역항체 포 함한 혈청학적 인자 등의 차이를 비교 분석하고자 하였다. 또한 각 신경학적 임상 증상의 발생 빈도를 알아보고 각 신경학적 임상 양상에 따른 특징 및 치 료, 예후 등을 평가하였다.
대상 및 방법
1. 대 상
1998년 4월부터 2011년 1월까지 13년간 서울 아산병원 소아청소년 병원에 방문 및 입원 치료한 전신성 홍반성 낭창 환자 51례의 환아를 대상으로
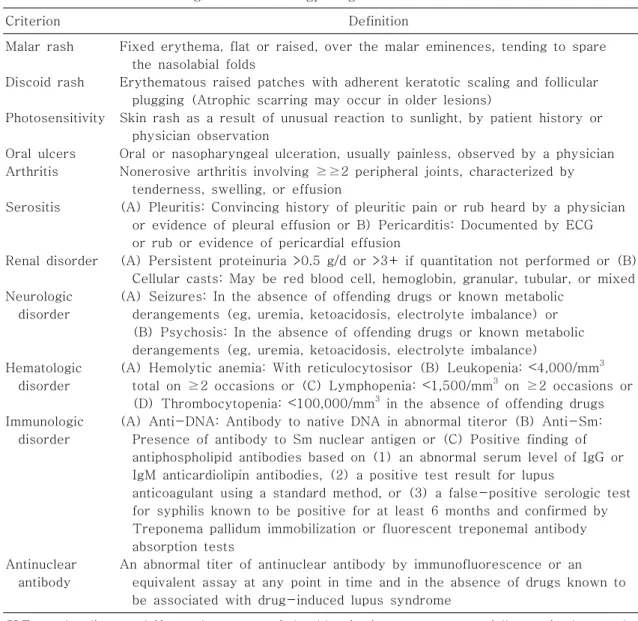
의무기록을 후향적으로 고찰하였다. 전신성 홍반성 낭창의 진단은 1997년 the American College of Rheumatology (ACR)에서 권유한 전신성 홍반성 낭창의 진단 기준8) 11가지 중에서 4가지 이상을 만 족할 때로 하였으며 신경학적 증상을 보이는 전신성 홍반성 낭창 역시 the American College of Rheu- matology (ACR)의 명명법과 정의에 근거해 분류하 였다(Table 1).
2. 방 법
51명 환아의 의무 기록을 후향적으로 고찰하여 성별, 나이, 임상 증상, 검사 소견, 영상 소견, 치료와 경과 등을 조사하였다. 또한 대표적 신경학적 증상 인 경련, 두통, 무도증에 대해 영상 소견, 뇌척수액 검사 소견, 항 인지질 항체 검사 소견, 치료에 대해 분석하였다.
3. 통 계
통계분석은 SPSS 12.0을 사용하였고 두 그룹 사 이의 자료에 대한 분석은 chi square test or Fi- sher’s exact test를 이용하였다.
결 과
1. 연구 대상 환자군의 임상적 특징 및 진단시기
1998년 4월부터 2011년 1월까지 13년간 서울 아산병원 소아청소년 병원에 방문 및 입원 치료한 전신성 홍반성 낭창 환자 51명 중 21명(41.2%)이 신경학적 증상을 보이는 전신성 홍반성 낭창 진단을 받았고 이 중 여아가 16명(76%)이었다. 또한 진단 시 평균 나이는 13.0세이고 중추 신경학적 증상은 12명(57.1%)의 환자에게서 진단 후 1개월 내에 발 현되었다. 51명의 전신성 홍반 낭창 환자는 평균 70 개월을 추적 관찰하였고 이 중 신경학적 증상을 보 이는 전신성 홍반성 낭창 진단을 받은 환자는 평균 67개월 동안 추적 관찰하였다.
신경학적 증상을 보이는 전신성 홍반성 낭창 환자
Table 1. The American College of Rheumatology Diagnosis Criteria
Criterion Definition
Malar rash
Discoid rash
Photosensitivity
Oral ulcers Arthritis
Serositis
Renal disorder
Neurologic disorder
Hematologic disorder
Immunologic disorder
Antinuclear antibody
Fixed erythema, flat or raised, over the malar eminences, tending to spare the nasolabial folds
Erythematous raised patches with adherent keratotic scaling and follicular plugging (Atrophic scarring may occur in older lesions)
Skin rash as a result of unusual reaction to sunlight, by patient history or physician observation
Oral or nasopharyngeal ulceration, usually painless, observed by a physician Nonerosive arthritis involving ≥≥2 peripheral joints, characterized by tenderness, swelling, or effusion
(A) Pleuritis: Convincing history of pleuritic pain or rub heard by a physician or evidence of pleural effusion or B) Pericarditis: Documented by ECG or rub or evidence of pericardial effusion
(A) Persistent proteinuria >0.5 g/d or >3+ if quantitation not performed or (B) Cellular casts: May be red blood cell, hemoglobin, granular, tubular, or mixed (A) Seizures: In the absence of offending drugs or known metabolic
derangements (eg, uremia, ketoacidosis, electrolyte imbalance) or (B) Psychosis: In the absence of offending drugs or known metabolic derangements (eg, uremia, ketoacidosis, electrolyte imbalance)
(A) Hemolytic anemia: With reticulocytosisor (B) Leukopenia: ˂4,000/mm3 total on ≥2 occasions or (C) Lymphopenia: ˂1,500/mm3 on ≥2 occasions or (D) Thrombocytopenia: ˂100,000/mm3 in the absence of offending drugs (A) Anti-DNA: Antibody to native DNA in abnormal titeror (B) Anti-Sm:
Presence of antibody to Sm nuclear antigen or (C) Positive finding of antiphospholipid antibodies based on (1) an abnormal serum level of IgG or IgM anticardiolipin antibodies, (2) a positive test result for lupus
anticoagulant using a standard method, or (3) a false-positive serologic test for syphilis known to be positive for at least 6 months and confirmed by Treponema pallidum immobilization or fluorescent treponemal antibody absorption tests
An abnormal titer of antinuclear antibody by immunofluorescence or an equivalent assay at any point in time and in the absence of drugs known to be associated with drug-induced lupus syndrome
SLE can be diagnosed if any 4 or more of the 11 criteria are present, serially or simultaneously, during any interval of observation.
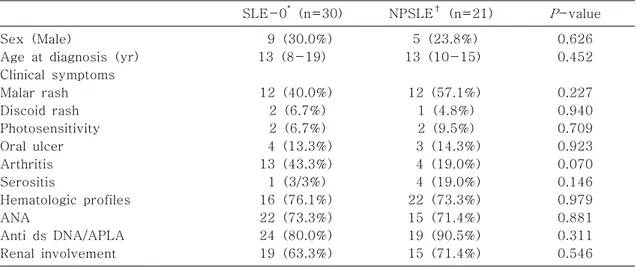
군에서 전신성 홍반성 낭창 진단 시의 초기 임상 증 상으로는 나비 모양 홍반이 12례(57.1%)로 가장 많았고 그 다음으로 관절통, 장막염이 각 4례(19.0
%), 구강 궤양 3례(14.3%), 광 과민성 2례(9.5%), 원반상 발진 1례(4.8%) 순이었으며, 이러한 증상의 발생률은 신경학적 증상이 없었던 환자군과 차이가 없었다. 병의 활동성을 반영하는 항 dsDNA 항체 및 co-morbidity를 반영하는 루프스 신염은 신경학적
증상을 보이는 전신성 홍반성 낭창 환자군에서 각각 90.5%와 71.4%로, 신경학적 증상이 없었던 환자군 에 비하여 상대적으로 높은 양성률을 보였으나 통계 적 유의성은 없었다. 신경학적 증상을 보인 환자군 과 신경학적 증상이 없었던 군 사이에 성별, 초기 임 상 증상 및 혈청학적 검사에서 통계적으로 유의한 차이는 없었다(Table 2).
진단 기준 외의 신경학적 증상을 보인 환자군과
Table 2. Comparisons of Initial Clinical Manifestation at Diagnosis in Patients with or without Neuropsychiatric Manifestations
SLE-0* (n=30) NPSLE† (n=21) P-value Sex (Male)
Age at diagnosis (yr) Clinical symptoms Malar rash Discoid rash Photosensitivity Oral ulcer Arthritis Serositis
Hematologic profiles ANA
Anti ds DNA/APLA Renal involvement
9 (30.0%) 13 (8-19)
12 (40.0%) 2 (6.7%) 2 (6.7%) 4 (13.3%) 13 (43.3%) 1 (3/3%) 16 (76.1%) 22 (73.3%) 24 (80.0%) 19 (63.3%)
5 (23.8%) 13 (10-15)
12 (57.1%) 1 (4.8%) 2 (9.5%) 3 (14.3%) 4 (19.0%) 4 (19.0%) 22 (73.3%) 15 (71.4%) 19 (90.5%) 15 (71.4%)
0.626 0.452
0.227 0.940 0.709 0.923 0.070 0.146 0.979 0.881 0.311 0.546 Abbreviations: ANA, antinuclear antibody; APLA, antiphospholipid antibody.
*SLE-0: SLE patients without neuropsychiatric symptoms.
†NPSLE: SLE patients with neuropsychiatric symptoms.
Table 3. Comparisons of Serological Markers in SLE patients with or without Neuropsychiatric Events
Disease activity marker SLE-0* (n=30) NPSLE† (n=21) P-value
C3 decreased (˂80mg/dL) C4 decreased (˂16mg/dL) Anti-dsDNA elevation ESR elevation
LA positivity
Anticardiolipin IgM Ab positivity Anticardiolipin IgG Ab positivity Antiphospholipid Ab positivity
24/30 (80%) 25/30 (83.3%) 24/30 (80%) 22/26 (84.6%) 11/28 (39.3%) 10/25 (40%) 15/25 (60%) 18/30 (60%)
19/21 (90.5%) 19/21 (90.5%) 18/21 (85.7%) 14/20 (70%)
8/20 (40%) 9/16 (56.3%) 7/16 (43/8%) 13/21 (61.9%)
0.445 0.685 0.720 0.292 0.960 0.309 0.309 0.891 Abbreviations: ESR, Erythrocyte sedimentation rate; LA, Lupus anticoagulant.
*SLE-0: SLE patients without neuropsychiatric symptoms.
†NPSLE: SLE patients with neuropsychiatric symptoms.
신경학적 증상을 보이지 않았던 환자군 간에 질병의 활동도 지표와 자가항체 양성률을 비교하였을 때, 신경학적 증상을 보인 전신성 홍반성 낭창 환아 21 명은 대조군에 비해 항핵항체(85.7%), 항인지질항 체(61.9%), ALCA IgM 양성율(56.3%) 및 C3, C4 보체 감소율(90.5%)이 대조군에 비해 높은 경향을 보였으나 통계적 유의성은 없었다(Table 3).
2. 신경학적 증상을 보이는
전신성 홍반성 낭창의 임상적 증상 및 경과
본 연구에서는 두통과 경련으로 발현한 환자가 대 부분으로, 각각 10명(47.6%)과 9명(42.9%)이었 다. 그 외 운동 이상, 말초신경증상, 뇌경색 등의 증 상이 각 2명(9.5%)에서 관찰되었다. 그리고 1명의 환자(4.8%)는 정신 증상(psychosis)을 보였다 (Table 4).
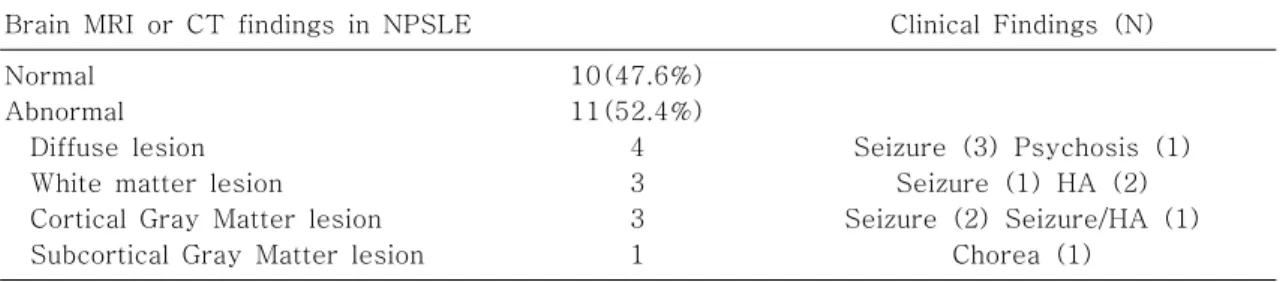
자기 공명영상에서는 신경학적 증상을 보였던 21 명의 환자 중 10례(47.6%)에서 이상 소견이 발견 되었으며 이 중 대부분에 해당하는 8명의 환자에게
Table 4. Features of Neuropsychiatric Mani- festations in NPSLE
Neuropsychiatric manifestation in SLE
N (total, 21) Seizure
Headache
Movement disorders Peripheral neuropathy/AIDP Stroke/TIA
Psychosis
10 (47.6%) 9 (42.9%) 2 (9.5%) 2 (9.5%) 2 (9.5%) 1 (4.8%) Abbreviations: TIA, Transient Ischemic Attack;
AIDP, Acute Inflammatory Demyelinating Poly- neuropathy
Table 5. Brain MRI or CT Findings of Patients with NPSLE
Brain MRI or CT findings in NPSLE Clinical Findings (N)
Normal Abnormal Diffuse lesion White matter lesion Cortical Gray Matter lesion Subcortical Gray Matter lesion
10(47.6%) 11(52.4%)
4 3 3 1
Seizure (3) Psychosis (1) Seizure (1) HA (2) Seizure (2) Seizure/HA (1)
Chorea (1) Abbreviations: HA, Headache
서 기저핵, 시상, 피질, 피질 하 백질, germinal matrix 등에 국소적 이상 소견이 관찰되었다. 2명의 환자에서 연수막하 조영 증강 소견이 관찰되었고 각 각 1명의 환자에서 대뇌 위축 및 척수의 다발성 병 변 소견이 보였다(Table 5).
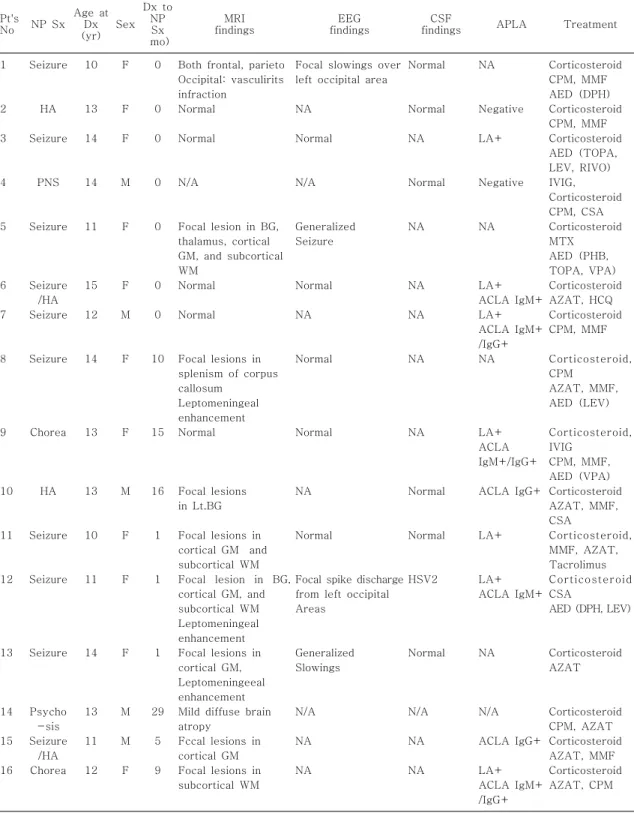
본 연구에 신경학적 증상을 보이는 전신성 홍반성 낭창 환자 21명 중 발작을 주 증상으로 하는 환자는 10명(47.6%)이었고 이 중 8명(80%)이 진단 1개 월 내에 증상이 나타났다. 10명의 환자는 모두 전신 성 강직 간대 발작을 보였고 이 중 6명의 환자가 자 기공명영상에서 다발성 병변의 연수막하 조영 증강 의 소견을 보였다. 그리고 5명의 환자가 뇌파검사상 부분/전반적 서파 또는 부분 극파 등의 이상 소견을 보였다. 이 중 4명의 환자에게 척수검사를 시행하였 고 제2형 단순포진 바이러스 양성 소견을 보인 1명 외에 3명은 모두 정상 뇌척수액 소견을 보였다 (Table 6).
발작을 보인 환자군 10명 중 5명(50%)의 환자가 발작 당시 항경련제를 복용하였고 이 중 자기공명영 상과 뇌파 검사상 이상 소견을 보인 2명의 환자는 현재까지도 항경련제를 복용하고 있다. 항경련제를 지속하고 있는 환자 5는 당시 간질중첩증으로 발현 하였고, 뇌전증 발작이 여전히 남아 있으며, 간질중 첩증의 합병증으로 재활치료 중인 상태이다. 환자 12는 최근 2년간 임상적 발작은 없으나 뇌파상에서 부분 발작 소견이 지속되는 상태로 항경련제를 지속 하고 있다.
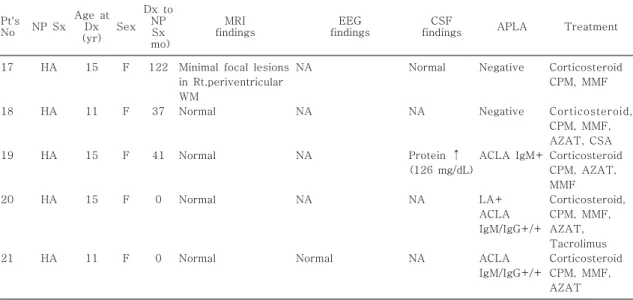
신경학적 증상을 보이는 전신성 홍반성 낭창 환자 21명중 두통을 주 증상으로 하는 환자는 9명(42.9
%)이며 발작을 보인 환자군과는 달리 전신성 홍반 성 낭창 진단 1개월 내에 증상을 보이는 환자는 9명 중 4명(44.4%)이었다. 두통은 대부분 갑작스럽게 발현하였으며 전두엽 혹은 측두엽을 병변으로 하였 고 9명의 환자 중 일시적인 시력상실을 동반한 1명 을 제외하고 3명은 열, 5명은 빈혈을 동반하였다. 이 중 자기공명영상 소견 상 이상 소견을 보인 환자는 9명중 3명으로 국소 병변 이상소견을 보였고 뇌파검 사를 시행한 2명은 모두 정상 소견, 척수검사를 시 행한 4명 중 1명만이 척수 내 단백이 126으로 상승 된 소견을 보였다. 이들 대부분이 면역 치료 이후 증 상이 호전되었다(Table 6).
무도증을 주 증상으로 하는 환자는 2명으로 2명 모두 항인지질 항체 양성이며 이 중 한 명은 자기 공 명영상 소견에서 피질하 백질의 국소적 이상소견을 보였다. 그리고 한 명은 고용량 스테로이드 치료에 반응이 없어 면역글로불린(400mg/kg/일, 5일)을
Table 6. Description of Patients Presenting with Neuropsychiatric Symptoms (N=21)
Pt's
No NP Sx Age at Dx (yr)
Sex Dx to
NP Sx mo)
MRI
findings EEG
findings CSF
findings APLA Treatment 1
2 3
4
5
6 7
8
9
10
11
12
13
14 15 16
Seizure
HA Seizure
PNS
Seizure
Seizure /HA Seizure
Seizure
Chorea
HA
Seizure
Seizure
Seizure
Psycho -sis Seizure
/HA Chorea
10
13 14
14
11
15 12
14
13
13
10
11
14
13 11 12
F
F F
M
F
F M
F
F
M
F
F
F
M M F
0
0 0
0
0
0 0
10
15
16
1
1
1
29 5 9
Both frontal, parieto Occipital: vasculirits infraction
Normal Normal
N/A
Focal lesion in BG, thalamus, cortical GM, and subcortical WM
Normal Normal
Focal lesions in splenism of corpus callosum
Leptomeningeal enhancement Normal
Focal lesions in Lt.BG
Focal lesions in cortical GM and subcortical WM Focal lesion in BG, cortical GM, and subcortical WM Leptomeningeal enhancement Focal lesions in cortical GM, Leptomeningeeal enhancement Mild diffuse brain atropy
Fccal lesions in cortical GM Focal lesions in subcortical WM
Focal slowings over left occipital area NA
Normal
N/A
Generalized Seizure
Normal NA
Normal
Normal
NA
Normal
Focal spike discharge from left occipital Areas
Generalized Slowings
N/A NA NA
Normal
Normal NA
Normal
NA
NA NA
NA
NA
Normal
Normal
HSV2
Normal
N/A NA NA
NA
Negative LA+
Negative
NA
LA+
ACLA IgM+
LA+
ACLA IgM+
/IgG+
NA
LA+
ACLA IgM+/IgG+
ACLA IgG+
LA+
LA+
ACLA IgM+
NA
N/A ACLA IgG+
LA+
ACLA IgM+
/IgG+
Corticosteroid CPM, MMF AED (DPH) Corticosteroid CPM, MMF Corticosteroid AED (TOPA, LEV, RIVO) IVIG, Corticosteroid CPM, CSA Corticosteroid MTX AED (PHB, TOPA, VPA) Corticosteroid AZAT, HCQ Corticosteroid CPM, MMF
Corticosteroid, CPM
AZAT, MMF, AED (LEV)
Corticosteroid, IVIG
CPM, MMF, AED (VPA) Corticosteroid AZAT, MMF, CSA
Corticosteroid, MMF, AZAT, Tacrolimus Corticosteroid CSA
AED (DPH, LEV)
Corticosteroid AZAT
Corticosteroid CPM, AZAT Corticosteroid AZAT, MMF Corticosteroid AZAT, CPM
Table 6. Description of Patients Presenting with Neuropsychiatric Symptoms (N=21) (continue)
Pt's
No NP Sx Age at Dx (yr)
Sex Dx to
NP Sx mo)
MRI findings
EEG findings
CSF
findings APLA Treatment 17
18
19
20
21 HA
HA
HA
HA
HA 15
11
15
15
11 F
F
F
F
F 122
37
41
0
0
Minimal focal lesions in Rt.periventricular WM
Normal
Normal
Normal
Normal
NA
NA
NA
NA
Normal
Normal
NA
Protein ↑ (126 mg/dL) NA
NA
Negative
Negative
ACLA IgM+
LA+
ACLA IgM/IgG+/+
ACLA IgM/IgG+/+
Corticosteroid CPM, MMF
Corticosteroid, CPM, MMF, AZAT, CSA Corticosteroid CPM, AZAT, MMF Corticosteroid, CPM, MMF, AZAT, Tacrolimus Corticosteroid CPM, MMF, AZAT
Abbreviations: HA, Headache; PNS, Peripheral nerve system; BG, Basal gangalia; GM, Gray matter;
WM, White matter; N/A, Not available; LA, Lupus anticoagulant; ACLA: Anticardiolipin antibody;
HSV2, Herpes simplex virus 2; CPM, Cyclophosphamide; CSA, Cyclosporin; AED, Antiepileptic drug; DPH, Phenytoin; TPM, Topiramate; LEV, Levetiracetam; CLZ, Clonazepam, MTX, Metho- trexate; PHB, Phenobarbital; VPA, Valporic acid; AZAT, Azathioprine; HCQ, Hydroquinone; MMF, Mycophenolate; IVIG: intravenous immunoglobulin; ANA, antinuclear antibody; APLA, antiphos- pholipid antibody.
투여 하였고 다른 한 명은 고용량 스테로이드 치료 후에 증상 호전을 보였다(Table 6).
3. 신경학적 증상을 보이는
전신성 홍반성 낭창의 치료와 임상경과 본 연구에 포함된 신경학적 증상을 보이는 전신성 홍반성 낭창 환자 21명 모두가 고용량 스테로이드요 법과 면역 억제 치료(cyclophosphamide, cyclos- porine, mycophenolate, azathioprine)를 받았으며 추적 관찰이 불가한 3명을 제외하고 18명 중 대부분 인 13명(72%)이 현재까지 스테로이드 유지요법을 지속하고 있으나 5명(28%)은 스테로이드를 중단한 상태이다. 현재 추적 관찰중인 환자는 모두 임상 경 과 상 호전을 보였다. 경련을 주 증상으로 보였던 10명중 2명만이 현재까지 항경련제를 지속하고 있 고 무도증 혹은 Guillain-Barre syndrome의 임상 증상을 보였던 환아는 IVIG 또는 스테로이드 투여 후 모두 증상이 호전되었으며 두통을 주 증상으로 보인 9명의 환자 중에서는 1명을 제외하고 모두 호
전되었다. 경련과 두통으로 진단 시 자기 공명영상 을 시행한 11명의 환자 중 추적관찰이 불가했던 1명 과 이후 검사를 시행하지 않은 4명을 제외한 6명 (55%)은 추적관찰 영상소견에서도 호전을 보였다.
고 찰
전신성 홍반성 낭창에서 신경학적 증상은 질환의 중증도와 활동도의 척도가 되며 전신성 홍반성 낭창 을 진단받은 환자에게서 삶의 질을 결정하는 주요한 인자가 된다고 알려져 왔다9). 소아 전신성 홍반성 낭창 환자는 성인에 비해 신경학적 증상의 유병률 및 중증도가 더 높은 것으로 알려져 있다10).
전신성 홍반성 낭창의 병리기전 및 원인에 대해 정립된 가설은 없지만 대부분 혈관병증, 자가면역 항체, 염증반응으로 설명되고 있다. 특히 뇌 혈관 장 벽은 신경학적 증상을 설명하는데 중요한 요소라고 할 수 있다. 염증 유발 인자인 사이토카인 혹은 자가 면역항체가 혈관 내피세포에 손상을 주고 이는 중추
신경계로 림프구의 유입을 촉진시켜 뇌 혈관 장벽을 손상시키는데, 이것이 결국 신경학적 증상으로 이어 진다는 가설이다. 그러나 대부분의 연구가 성인과 소아의 면역학적 기전 및 뇌의 구조적인 차이에 대 해서는 고려하지 않았다10).
본 연구에서 전신성 홍반성 낭창 환자 중 40% 정 도가 신경정신학적 이상을 보였으며 이 중 진단 1개 월 이내 신경학적 증상을 보이는 경우가 57.1%로 신경학적 증상이 비교적 흔한 초기 임상 증상임을 알 수 있었다. 이는 객관적인 신경학적 이상 소견을 보인 경우만을 포함한 것으로, 여기에 기분장애, 불 안, 정신병 등의 정신과적 증상과 주의력 결핍, 기억 력 장애까지도 포함시킨다면 훨씬 높은 비율로 나타 날 것이다. 이러한 맥락에서는 오히려 신경학적 증 상이 본 연구에서 과소평가 되었을 가능성이 있다고 볼 수 있다. 하지만 전신성 홍반성 낭창은 만성 질환 으로 만성화에 따른 기분장애가 있을 수 있으며 사 춘기 시기에 호발하는 질환으로 본 연구에 포함된 환자들의 연령을 고려할 때 사춘기에 따른 감정 변 화와도 감별이 필요하다11).
본 연구 결과를 요약하면, 신경학적 증상을 보이 는 전신성 홍반성 낭창 환자군이 대조군에 비해 진 단 기준 뿐만 아니라 질병의 활동도 및 불량 예후인 자라고 볼 수 있는 자가 면역 항체 등 혈청학적 요소 의 비교에서도 통계적으로 유의한 차이를 보이지 않 았다고 요약할 수 있다. 이전 연구에서는 신경학적 증상은 보통 학령기나 사춘기 시기보다는 학령전기 에서 더 호발한다고 보고된 바 있었고12), 보체의 감 소 정도나 항핵항체가 더 낮은 즉 질병의 활동도가 낮은 시기에 신경학적 증상이 더 발현될 확률이 높 다는 보고들이 있었다13, 14). 그러나 본 연구에서는 이전 연구와는 상반되게 신경학적 증상을 보이는 전 신성 홍반성 낭창과 대조군에서 호발 연령은 학령기 로 동일하게 나타났고 통계적으로 유의한 정도는 아 니지만 보체의 감소 정도는 신경학적 증상을 보인 환자군에서 더 큰 변화를 보였다. 또한 신경학적 증 상을 보이는 전신성 홍반성 낭창 환자군에서 LA, ACLA IgM도 차이가 없었다. 따라서 본 연구에서는 전신성 홍반성 낭창 진단 시에 신경학적 증상의 발
병을 예측하는 유의한 임상적인 인자 및 혈청학적 인자가 없었다. 추적관찰기간 동안 사망률이나 치명 적인 합병증에서도 차이를 보이지 않았다.
그 이유는 본 연구는 3차 단일 병원에서 진행된 것으로 21명의 신경학적 증상을 보이는 전신성 홍반 성 낭창 환자 중 12명(57%)이 진단 후 대부분 2주 에서 4개월 후에 전원되어 정확한 초기 검사 소견을 확인할 수 없었으며 초기 진단 시 항 인지질 항체에 대한 검사가 대부분 시행되지 않았었기 때문이다.
그리고 신경학적 증상은 급성기를 지나면서 대부분 호전된 경과를 보였고 외래에서 추적 관찰 시 주기 적인 자가 면역항체 검사가 시행되지 않아 질병의 경과와 자가 면역항체 역가의 상관관계를 비교하는 것이 불가능했다. 그 다음으로는 인종과 질병의 단 계에 따른 차이 역시 다른 연구와의 상대적인 비교 를 어렵게 하는 요인이라고 할 수 있겠다. 신경학적 증상을 보이는 전신성 홍반성 낭창의 예측 및 예후 인자들에 대한 연구는 서양인을 대상으로 한 연구가 대부분이었고15-17), 25명의 일본인 대상으로 한 연 구에서는 초기 진단 시 혈청학적 인자들이 통계적으 로 유의한 차이를 보이지 않았으나 이 후 29년 동안 의 추적관찰 기간 동안 신경학적 증상이 재발한 경 우에 있어 항 dsDNA항체, 백혈구 수, 적혈구 침강 속도에서 유의한 차이를 보였다는 보고가 있었다13). 또 본 연구에 포함된 환자군에서 신경학적 증상의 대표적 증상이었던 발작의 경우 항인지질 항체 검사 를 시행하지 않는 4명의 환자들을 제외하고 6명의 환자에서 모두 LA나 ACLA IgM/G 양성 소견을 보 였다. 따라서 초기 진단과 평가 시에 항인지질 관련 항체의 적극적인 검사가 필요하며 이는 진단과 예후 를 예측하는데 도움이 될 것이라 생각한다.
치료 결과에서 본 연구에 포함된 신경학적 증상을 보이는 전신성 홍반성 낭창 환자들의 예후는 이전 연구의 결과17)와는 달리 대부분 치료에 대한 반응이 좋아 신경학적 증상의 재발이나 사망률의 증가를 보 이지 않았다. 환자 4는 하지 쇠약감을 주소로 내원 하였고 Gullain-Barre Syndrome 의증으로 면역글 로불린을 투여하였으나 신경학적 증상의 변화를 보 이지 않았다. 추후 상기 증상은 전신성 홍반성 낭창
의 신경학적 증상의 하나로 여겨져 3일간의 고용량 스테로이드 요법을 시행하였고 이후 신경학적 증상 의 뚜렷한 호전양상을 보였다18). 이는 전신성 홍반 성 낭창에 대한 초기 진단과 적극적인 치료의 결과 로 보여지나, 역시 향후 장기적 추적 관찰 시의 증상 재발 등에 대한 추가적 연구가 필요하겠다.
본 연구는 몇 가지 한계점을 가지고 있다. 첫째는 선택 편의(selection bias)로 본원은 3차 병원으로 질병의 중증도가 높아 진단 기준, 혈청학적 인자, 기 타 검사 소견, 예후 등에서 일반적인 인구 분포와는 차이가 있으리라는 점이다. 두 번째로는 이차적인 원인에 의한 신경학적 증상의 배제가 정확히 이루어 지지 않았다는 점이다. 예를 들어, 본 연구에서 발작 을 신경학적 주 증상으로 하는 환자 중 항경련제를 지속하고 있는 두 명중 한 명은 발작 당시 뇌척수액 검사 소견 상 제2형 단순포진 바이러스 양성 소견을 보였으며 자기공명 영상 소견에서도 감염의 가능성 을 완전히 배제할 수는 없는 상태였다. 세 번째로는 객관적 신경학적 증상의 평가가 어려웠다는 점이다.
특히 본원에서 대표적인 신경학적 증상 중 하나인 두통은 환자들이 임상 증상의 하나로 자각하는 경우 가 드물거나 객관적 평가 척도의 부재로 인해 과소 평가 되었을 가능성이 높다. 네 번째로는 본 연구에 서 각 환자들을 추적 관찰한 기간이 평균 13년으로 추적 관찰 중 환자의 소실 혹은 성인 이후로 소아과 의 추적 관찰이 불가한 경우가 있었다. 따라서 장기 간의 추적 관찰로 질병의 활동도 및 재발 유무에 따 른 지속적인 연구 자료가 더 축적되어야 할 것이다.
소아 전신성 홍반성 낭창 환자에서 신경학적 증상 은 드물지 않으며 진단 초기에 발생하는 경우가 흔 하다. 따라서 특정한 원인을 찾을 수 없는 발작, 또 는 두통 등 신경학적 증상을 보이는 경우에 신경학 적 증상을 보이는 전신성 홍반성 낭창을 감별질환으 로 고려해 보아야 할 것이다. 더불어 더 많은 연구를 토대로 좀 더 정확하고 구체적인 진단 기준이 마련 되어야 할 것이며 이를 위해 다기관, 전향적 연구를 통한 신경학적 증상을 보이는 소아 전신성 홍반성 낭창의 체계적 진단 및 장기적인 추적 관찰의 자료 축적이 이루어져야 하겠다. 그럼으로써 구체적 진단
기준이 확립되어 이에 따라 치료한다면 증가하는 신 경학적 증상을 보이는 소아 전신성 홍반성 낭창의 치료와 예후 향상에 큰 도움이 될 것이라고 생각된 다.
요 약
목 적 : 전신성 홍반성 낭창(SLE)은 다발성 장기 를 침범하는 자가면역 질환으로 그 중 신경학적 증 상의 발현은 소아 전신성 홍반성 낭창 환자의 사망 률과 예후를 결정하는 요인 중의 하나로 알려져 있 다. 본 연구에서는 소아 전신성 홍반성 낭창 환자들 의 신경학적 증상의 발현 양상 및 혈청학적 인자, 뇌 영상 소견 등을 파악하여 향후 신경학적 증상을 보 이는 전신성 홍반성 낭창의 진단과 예후 판단에 도 움이 되고자 하였다.
방 법 : 1998년 04월부터 2011년 01월까지 울산 의대 서울아산병원 소아청소년과에서 전신성 홍반성 낭창으로 진단받은 62명의 환자 중 추적 가능한 51 명을 대상으로 의무기록 검토를 통해 나이, 성별, 신 경학적 증상 및 기타 임상 증상, 진단시의 혈청학적 인자, 신경학적 이상 발현 시의 뇌 영상 소견을 조 회, 분석 하였다.
결 과 : 1년 이상 추적 관찰이 가능했던 51명 중 41.2%에 해당하는 21명이 신경학적 증상을 보이는 전신성 홍반성 낭창으로 진단되었다. 12명(57.1%) 의 환자가 전신성 홍반성 낭창 진단 1개월 내에 신 경학적 증상이 발현되었으며 당시 평균 연령은 13세 였다. 21명의 환자 중 10명(47.6%)에서 경련발작 이 보였고 9명(42.9%)에서 두통이, 2명(9.5%)에 서 무도증이 보였다. 소아 전신성 홍반성 낭창 환자 들과 신경학적 증상을 보인 환자군을 비교했을 때 임상증상, 혈액학적 그리고 면역학적 소견에서 유의 한 차이는 보이지 않았다.
결 론 : 소아에서 신경학적 증상을 보이는 전신성 홍반성 낭창은 성인에 비해 높은 유병율을 보인다고 알려져 있다. 그러나 진단 시 신경학적 증상을 보이 는 전신성 홍반성 낭창을 예측할 수 있는 유의한 인 자가 없어 임상적 의심이 진단에 가장 중요한 요소 라고 할 수 있다. 그러므로 신경학적 증상을 보이는
전신성 홍반성 낭창의 예후를 향상시키기 위해서는 자세한 병력 청취 및 신체검진, 필요한 진단적 검사 를 시행하여 진단하고 이어 즉각적인 치료가 이루어 져야 한다.
References
1) Huizinga TWJ, Diamond B. Lupus and the central nervous system. Lupus 2008;17:376-9.
2) Benseler SM, ED Silverman. Review: Neuropsy- chiatric involvement in pediatric systemic lupus erythematosus. Lupus 2007;16:564-71.
3) Yu HH, Lee JH, Wang LC, Yang YH, Chiang BL.
Neuropsychiatric manifestations in pediatric sys- temic lupus erythematosus: a 20-year study.
Lupus 2006;15:651-7.
4) Hanly JG. Neuropsychiatric Lupus. Rheum Dis Clin N Am 2005;31:273-98.
5) Jennekens F.G.I , Kater L. The central nervous system in systemic lupus erythematosus. part 2.
pathogenetic mechanisms of clinical sysdromes:
a literature investigation. Rheumatology 2002;
41:619-30.
6) West SG. Lupus and the central nervous system.
Curr Opin Rheumatol 1996;8:408-14.
7) Efthimiou P, Blanco M. Pathogenesis of neurop- sychiatric systemic lupus erythematosus and potential biomarkers. Mod Rheumatol 2009;15:
457-68.
8) Hochberg MC. Updating the American College of Rheumatology revised criteria for the classifica- tion of systemic lupus erythematousus. Arthritis Rheumatol 1997;40:1725.
9) Feng X, Zou Y, Pan W, Wang X, Wu M, Zhang M, et al. Prognostic indicators of hospitalized patients with systemic lupus erythematosus: a large retrospective multicenter study in China. J Rheumatol 2011;38:1289-95.
10) Demirkaya E, Bilginer Y, Aktay-Ayaz N, Yalni-
zoglu D, Karli-Oguz K, Isikhan V, et al. Neurop- sychiatric involvement in juvenile systemic lupus erythematosus. The Turkish Journal of Pediat- rics 2008;50:126-31.
11) Eyal M, Robin B. Neurological Manifestations of Systemic Lupus Erythematosus in Children and Adults. Neurol Clin 2010;28:61-73.
12) Zhu J, Wu F, Huang X. Age-related differences in the clinical characteristics of systemic lupus erythematosus in children. Rheumatol Int 2012;
07:DOI 10.1007/s00296-011-2354-4.
13) Shimojima Y, Matsuda M, Gono T, Ishii W, Ikeda S. Relationship between clinical factors and neu- ropsychiatric manifestations in systemic lupus erythematousus. Clin Rheumatol 2005;24:469- 75.
14) Hanly JG, McCurdy G, Fougere L, Douglas JA, Thompson K. Neuropsychiatric events in sys- temic lupus erythematosus: attribution and clini- cal significance. J Rheumatol 2004;31:2156-62.
15) Sibbitt WL Jr, Brandt JR, Johnson CR, Maldo- nado ME, Patel SR, Ford CC, et al. The inci- dence and prevalence of neuropsychiatric synd- romes in pediatric onset systemic lupus erythe- matosus. J Rheumatol 2002;29:1536-42.
16) Brey RL, Holliday SL, Saklad AR, Navarrete MG, Hermosillo-Romo D, Stallworth CL, et al.
Neuropsychiatric syndromes in lupus: preva- lence using standardized definitions. Neurology 2002;58:1214-20.
17) Rosner S, Ginzler EM, Diamond HS, Weiner M, Schlesinger M, Fries JF, et al. A multicenter study of outcome in systemic lupus erythemato- sus. II. Causes of death. Arthritis Rheum 1982;
25:612-7.
18) Kang SH, Yum MS, Lee EH, Ko TS. Concurrent Gullain-Barre Syndrome and acute transverse myelitis as an initial presentation of systemic lupus erythematosus. J Korean Child Neurol Soc 2012;20:121-8.