이소성 다형성 선종: 증례 보고
모하메드 바크리1),3), 예서 말하즈미2),3), 박준형1), 전재호1), 파레디 묵람3), 명훈1)*
서울대학교 치과병원 구강악안면외과학교실, 뉴욕주립대학교 구강악안면병리학교실, 사우디아라비아 야잔대학교 치의학부
<Abstract>
Ectopic Pleomorphic Adenoma: A Case Report
Mohammed Bakri1),3), Yaser Alhazmi2),3), Park Jun Hyung1), Jae-ho Jeon1), Fareedi Mukram Ali3), Hoon Myoung1)*
1)Department of Oral & Maxillofacial Surgery, Seoul National University Dental Hospital, Seoul, Korea
2)Department of Oral & Maxillofacial Pathology, SUNY at Buffalo, NY, USA
3)Department of Oral & Maxillofacial Surgery, Jazan University Dental school, Jazan, Saudi Arabia
The most common benign salivary gland tumor is pleomorphic adenoma. It affects major and minor salivary glands. Minor salivary gland tumors constitute <20% of all salivary gland neoplasms. Most minor salivary gland tumors occur on the palate. We present the case of a patient with pleomorphic adenoma that developed at a rare intraoral location. This patient presented to the Department of Oral and Maxillofacial Surgery of Seoul National University Dental Hospital.
Key words: Adenoma, Pleomorphic adenoma, Ectopic, Rare location
Korean Journal of Oral and Maxillofacial Pathology 2017;41(5):233-236 ISSN:1225-1577(Print); 2384-0900(Online) Available online at http://journal.kaomp.org https://doi.org/10.17779/KAOMP.2017.41.5.005
* Correspondence: Hoon Myoung, Department of Oral and Maxillofacial Surgery, School of Dentistry and Dental Research Institute, Seoul National University, 101 Daehak-ro, Jongno-gu, Seoul 03080, Korea Tel: +82-2-2072-3059, Fax: +82-2-766-4948
E-mail: [email protected] ORCID : 0000-0002-9984-8479
Received: Sep. 16. 2017; Revised: Sep. 29. 2017; Accepted: Oct. 13. 2017
Ⅰ. INTRODUCTION
1. Patient
A 70-year-old woman presented to Seoul National University Dental Hospital with a painless swelling in the left pterygomaxillary area. The patient had a history of medically controlled hypertension, with no other significant medical conditions.
On clinical examination, a 2.5 × 1.5 × 1-cm dome-shaped
mass was noted in the left pterygomaxillary region. The covering mucosa was smooth; on palpation, the lesion was rubber-like and non-tender and had some mobility over the underlying tissues.
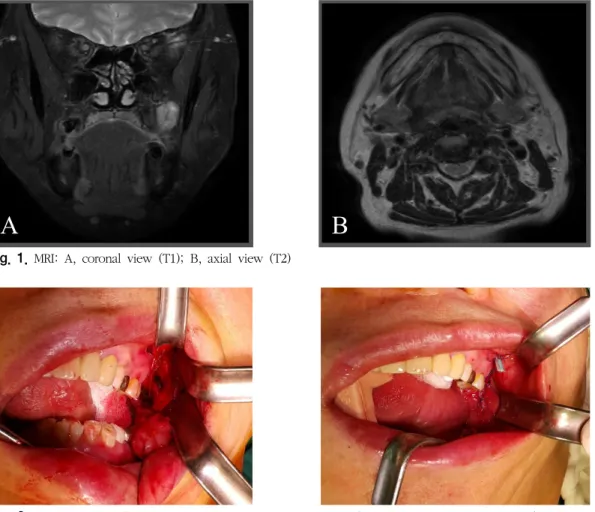
Magnetic resonance imaging (MRI) revealed a heterogeneous lesion with hyperintense T2 signals. The buccinator, lateral pterygoid, and temporalis muscles surrounded the lesion.
The lesion was capsulated and had clear margins (Fig. 1).
Based on the disease history and clinical findings, fibroma and a minor salivary gland tumor were in the top of differential diagnoses list.
234
A B
Fig. 1. MRI: A, coronal view (T1); B, axial view (T2)
Fig. 2. Wide excision of the lesion with primary closure was performed. The excised specimen (2.5 × 2.5cm) was sent for histopathological examination. The tumor lies in the left pterygomaxillary region.
Fig. 3. The mass after excision (size, 1.5 × 2.5 cm) 2. Surgery
Under general anesthesia wide excision of the lesion with primary closure was performed. The excised specimen
(size: 2.5 × 2.5 cm) was sent to histopathological lab for examination (Fig. 2, 3). Surgical removal of the entire mass was performed using the intraoral approach.
235
A B C
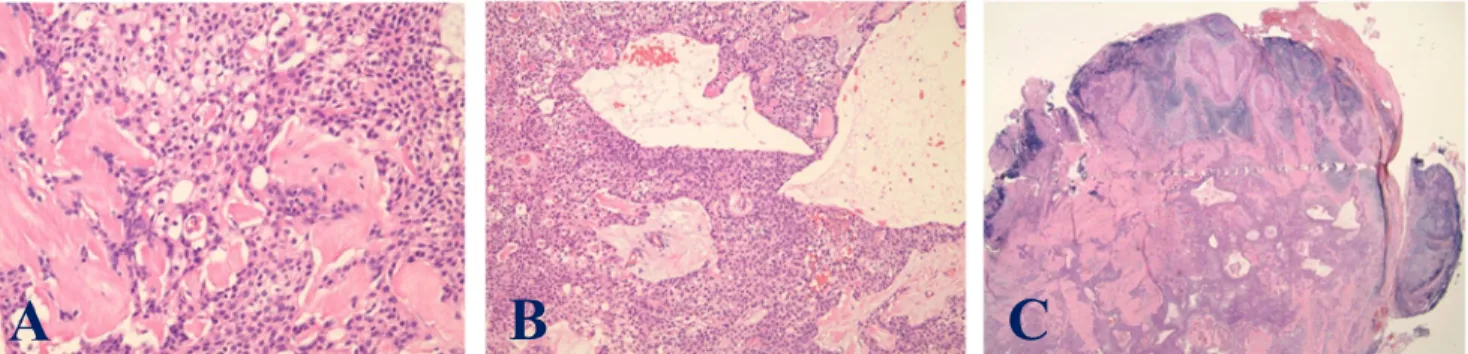
Fig. 4. Hematoxylin and eosin staining Microscopic examination of the excised mass. A: Proliferation of plasmacytoid myoepithelial cells with intervening areas of hyalinized stroma. B: Well-circumscribed, non-encapsulated lesion with biphasic growth of epithelial and myoepithelial cells forming ductal structures. C: Large cystic dilation surrounded by a proliferation of ductal epithelial cells
3. Histopathological examination
Histopathological examination revealed a well-circumscribed, non-encapsulated lesion with biphasic growth of epithelial and myoepithelial cells, forming ductal structures and pushing on the peripheral lymphoid structure. The abluminal myoepithelial cells showed plasmacytoid and spindle-cell architecture. Large cystic dilations surrounded by a proliferation of ductal epithelial cells were also noted. The proliferated myoepithelial cells merged into areas of densely hyalinized stroma at some places. The diagnosis Based on the findings was pleomorphic adenoma of the minor salivary glands (Fig. 4).
4. Follow-up
The patient was followed up for 9 months. Uneventful healing of the surgical site was observed and no evidence of recurrence.
5. Comments
In this case the tumor developed at a rare intraoral location. The tumor lies in the left pterygomaxillary region.
Ⅱ. DISCUSSION
Minor salivary glands are mucous glands scattered across the upper respiratory tract. Most minor salivary glands are found in the palate, whereas others are distributed at the inner surface of the lips; around the opening of the parotid duct; in the submucosa of the uvula, mucous membrane of the cheek, floor of the mouth, palatoglossal folds, and superior pole of the tonsils (Weber’s glands); on the inferior surface of the tongue; near the frenulum of the tongue;
within the palatine tonsil; and in other uncommon places, such as the pterygomaxillary area.7-9)
Pleomorphic adenomas are benign heterogeneous (myoepithelial and epithelial) tumors of salivary gland origin and are considered a benign mixed tumor.
Pleomorphic adenomas arising in the pterygomaxillary area are rare and the most common site is the palate. It usually appears as a firm, rubbery, submucosal mass. In the present patient, based on clinical examination alone, we placed pleomorphic adenoma at the top of our deferential diagnosis list.10,11)
Pleomorphic adenoma is known to have some degree of recurrence either due to spillage, inadequate removal, or enucleation at the time of operation, but there are no reports of distant metastasis. In the literature, a recurrence rate of 2%–44% has been reported. Wide local excision is
236 the treatment of choice for pleomorphic adenoma with the removal of the periosteum and/or bone if they are involved.2,4,7)
Rarely, malignant lesions develop within this tumor (e.g.;
carcinoma ex pleomorphic adenoma). The most common clinical features for identifying malignancy include an infiltrative growth pattern, vascular permeation, perineural invasion, and marked cytologic atypia with abnormal mitotic figures.12-14)
REFERENCES
1. Thakur JS, Mohindroo NK, Mohindroo S, Sharma DR, Thakur A: Pleomorphic adenoma of minor salivary gland with therapeutic misadventure: A rare case report. BMC Ear Nose Throat Disord 2010;10:2.
2. Neville BW, Damm DD, Allen CM, Bouquot JE. 2nd ed. Philadelphia, WB Saunders, 2002, Oral and Maxillofacial Pathology, pp. 410–413.
3. Mubeen K, Vijayalakshmi KR, Patil AR, Giraddi GB, Singh C; Benign pleomorphic adenoma of minor salivary gland of palate. J Dent Oral Hyg. 2011;3:82–8.
4. Dalati T, Hussein MR; Juvenile pleomorphic adenoma of the cheek: A case report and review of literature.
Diagn Pathol 2009;4:32.
5. Varghese BT, Sebastian P, Abraham EK, Mathews A: Pleomorphic adenoma of minor salivary gland in the parapharyngeal space. World J Surg Oncol 2003;
1:2.
6. Hirabayashi S, Yanai A, Muraishi Y: Huge pleomorphic adenoma of the upper retromolar area. Ann Plast Surg 1997;38:184–186.
7. Tian Z, Li L, Wang L, Hu Y, Li J: Salivary gland neoplasms in oral and maxillofacial regions: A 23-year retrospective study of 6982 cases in an eastern Chinese population. Int J Oral Maxillofac Surg 2009;39:235–242.
8. Kaminski M, Janicki K:A case of giant pleomorphic adenoma of the cheek with two malignant centers.
Otolaryngol Pol 2002;56:385–387.
9. Ledesma-Montes C, Garces-Ortiz M: Salivary gland tumours in a Mexican sample. A retrospective study. Med Oral 2002;7:324–330.
10. Kondo T. A case of lipomatous pleomorphic adenoma in the parotid gland. Diagn Pathol 2009;4:16.
11. Lopes MA, Kowalski LP: A clinicopathologic study of 196 intraoral minor salivary gland tumours. J Oral Pathol Med 1999;28:264–267.
12. Lewis JE, Olsen KE, Sebo TJ: Carcinoma ex pleomorphic adenoma: Pathologic analysis of 73 cases. Hum Pathol 2001;32:596–604.
13. Czader M, Eberhart CG, Cummings C, Westra WH:
Metastasizing mixed tumor of the parotid: Initial presentation as a solitary kidney tumor and ultimate carcinomatous transformation at the primary site.
Am J Surg Pathol 2000;24:1159–1164.
14. Rao PK, Shetty SR, Hegde D: Ectopic pleomorphic adenoma. N Am J Med Sci 2012;4:190–192.