D I A B E T E S & M E T A B O L I S M J O U R N A L
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
γ-Linolenic Acid versus α-Lipoic Acid for Treating Painful Diabetic Neuropathy in Adults: A 12-Week, Double-Placebo, Randomized, Noninferiority Trial
Jong Chul Won1, Hyuk-Sang Kwon2, Seong-Su Moon3, Sung Wan Chun4, Chong Hwa Kim5, Ie Byung Park6, In Joo Kim7, Jihyun Lee8, Bong Yun Cha9, Tae Sun Park10
1 Division of Endocrinology and Metabolism, Department of Internal Medicine, Cardiovascular and Metabolic Disease Center, Inje University Sanggye Paik Hospital, Inje University College of Medicine, Seoul,
2 Division of Endocrinology and Metabolism, Department of Internal Medicine, Yeouido St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul,
3Department of Internal Medicine, Dongguk University College of Medicine, Gyeongju,
4 Division of Endocrinology and Metabolism, Department of Internal Medicine, Soonchunhyang University Cheonan Hospital, Soonchunhyang University College of Medicine, Cheonan,
5Division of Endocrinology and Metabolism, Department of Internal Medicine, Sejong General Hospital, Bucheon,
6 Division of Endocrinology and Metabolism, Department of Internal Medicien, Gachon University Gil Medical Center, Gachon University College of Medicine, Incheon,
7 Division of Endocrinology and Metabolism, Department of Internal Medicine, Pusan National University Hospital, Pusan National University School of Medicine, Busan,
8Department of Internal Medicine, Daegu Catholic University School of Medicine, Daegu,
9Division of Endocrinology and Metabolism, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul,
10Division of Endocrinology and Metabolism, Department of Internal Medicine, Chonbuk National University Medical School, Jeonju, Korea
Background: This study was a multicenter, parallel-group, double-blind, double-dummy, randomized, noninferiority trial to evaluate the efficacy and safety of γ-linolenic acid (GLA) relative to α-lipoic acid (ALA) over a 12-week treatment period in type 2 diabetes mellitus (T2DM) patients with painful diabetic peripheral neuropathy (DPN).
Methods: This study included 100 T2DM patients between 20 and 75 years of age who had painful DPN and received either GLA (320 mg/day) and placebo or ALA (600 mg/day) and placebo for 12 weeks. The primary outcome measures were mean changes in pain intensities as measured by the visual analogue scale (VAS) and the total symptom scores (TSS).
Results: Of the 100 subjects who initially participated in the study, 73 completed the 12-week treatment period. Per-protocol analyses revealed significant decreases in the mean VAS and TSS scores compared to baseline in both groups, but there were no significant differences between the groups. The treatment difference for the VAS (95% confidence interval [CI]) between the two groups was −0.65 (−1.526 to 0.213) and the upper bound of the 95% CI did not exceed the predefined noninferiority margin (δ1=0.51). For the TSS, the treatment difference was −0.05 (−1.211 to 1.101) but the upper bound of the 95% CI crossed the non- inferiority margin (δ2=0.054). There were no serious adverse events associated with the treatments.
Conclusion: GLA treatment in patients with painful DPN was noninferior to ALA in terms of reducing pain intensity measured by the VAS over 12 weeks.
Keywords: Diabetic neuropathies; Gamma-linolenic acid; Thioctic acid
Corresponding author: Tae Sun Park https://orcid.org/0000-0001-7216-8468 Division of Endocrinology and Metabolism, Department of Internal Medicine, Chonbuk National University Medical School, 20 Geonji-ro, Deokjin-gu, Jeonju 54907, Korea E-mail: [email protected]
https://doi.org/10.4093/dmj.2019.0099 pISSN 2233-6079 · eISSN 2233-6087
INTRODUCTION
The occurrence of type 2 diabetes mellitus (T2DM) is increas- ing worldwide [1], and in Korea, one in every seven adults aged 30 years or older has diabetes [2]. Diabetic sensorimotor distal symmetric polyneuropathy, or diabetic peripheral neu- ropathy (DPN), is the most common neuropathy associated with diabetes as well as the most common complication in dia- betes patients. Approximately one in every three T2DM pa- tients in Korea has DPN [3], and 42.3% of those with DPN ex- perience painful symptoms or are taking medication(s) for their current pain [4]. Although many available guidelines rec- ommend anticonvulsants and antidepressants as first-line treatments for painful DPN, there are unmet needs in terms of efficacy and tolerability, and these treatment modalities modu- late the pain rather than favorably influencing the underlying neuropathic processes [5]. Additionally, the painful symptoms of DPN may vary with the course of nerve damage, the pres- ence of comorbidities, and/or ethnic and cultural differences [6], which creates therapeutic challenges regarding the man- agement of painful symptoms [5].
A novel treatment option, γ-linolenic acid (GLA), is an n-6 polyunsaturated fatty acid that is converted from dietary lino- lenic acid (primrose oil), and as an essential component of structural phospholipids in neural cell membranes, is neces- sary for the maintenance of normal nerve membrane structure and function [7]. For example, decreases in the production and increases in the destruction of GLA are associated with im- paired nerve conduction in patients with T2DM [8,9]. Thus, based on the pathogenetic mechanisms of DPN, GLA has been developed as a potential disease-modifying therapeutic drug [10,11], along with other potential treatment modalities such as α-lipoic acid (ALA) [12,13], aldose reductase inhibitors [14], vascular endothelial growth factors [15], and protein ki- nase C-β inhibitors [16]. These treatment options were de- signed to favorably influence the underlying pathophysiology of DPN rather than merely provide symptomatic relief for DPN patients. GLA treatment corrects impaired nerve func- tion in animal models of diabetes [17] and is beneficial for neurophysiological parameters, thermal thresholds, and clini- cal sensory symptoms in patients with T2DM [8]. A previous study of 934 Korean patients with painful DPN found that 40.2% (n=396) were prescribed ALA and 17.2% (n=169) were prescribed GLA [3]. Although the efficacies of oral and intra- venous ALA have been established by meta-analyses of clinical
trials [18,19], the efficacy of GLA for improving the symptoms of patients with painful DPN has yet to be determined.
Thus, the primary aim of the present study was to investigate the noninferiority of the efficacy of GLA (Evoprim; Dalim Bio- tech, Seoul, Korea) relative to ALA (Lipo-A HR; Dalim Bio- tech) as an active comparator. GLA was orally administered for 12 weeks as a treatment for the neuropathic symptoms of T2DM patients with painful DPN.
METHODS
Study population
Subjects were eligible for the present study if they agreed to participate, were between 20 and 75 years of age, had T2DM with glycosylated hemoglobin (HbA1c) levels ≤11.0% at the time of screening, had an average visual analogue scale (VAS) score ≥4.0 for the 24-hour average pain score (0 to 10 numeri- cal rating scale), and a diagnosis of DPN after a thorough eval- uation for other causes of neuropathy at the screening. The ex- clusion criteria consisted of the following: a confounding neu- rological disease or neuropathy caused by progressive or de- generative disorders that may have interfered with the assess- ment of DPN severity; uncontrolled hypertension (systolic or diastolic blood pressure levels ≥160 or ≤100 mm Hg or ≥95 or ≤60 mm Hg, respectively); an amputated foot or leg; a clini- cally significant cardiac, pulmonary, gastrointestinal, hemato- logical, or other endocrinological disease (e.g., abnormal thy- roid function test even though taking medication); organ transplants; aspartate aminotransferase or alanine aminotrans- ferase levels >3 times normal levels; serum creatinine levels
>2.0 mg/dL; drug or alcohol abuse within the last year; use of an investigational drug within the last 6 months; severe or ana- phylactic reactions; pregnant or lactating women; and/or cor- ticosteroid or local anesthetic therapies within the last 2 months. Subjects were enrolled at 11 sites in the Republic of Korea and the study was carried out from January 26, 2016 to July 25, 2018 (ClinicalTrials.gov number, #NCT03914404). All study procedures were conducted in accordance with the Dec- laration of Helsinki and ICH Good Clinical Practice, and were approved by Institutional Review Board at all sites (IRB No.:
CUH 2015-06-001, XC15MSMV0063K, 1528, GAIRB2015- 237, XC15MSMV0063S, D-1506-022-041, CR-15-069-L, 110757-201507-HR-01, SCHCA 2015-06-021-007, 4-2015- 0628, SGPAIK 2017-08-01). Written informed consent was obtained from all patients.
Study design and medication Study design
The present study was a multicenter, double-blind, double- dummy, randomized, active-controlled, noninferiority trial that compared GLA (twice daily) and placebo (once daily) to ALA (once daily) and placebo (twice daily) to investigate changes in VAS and total symptom scores (TSS) between base- line and the end of the 12-week study period (Supplementary Fig. 1). All subjects engaged in a wash-out period for 2 weeks during which all current medications for the treatment of DPN (anticonvulsants, tricyclic antidepressants, serotonin–norepi- nephrine reuptake inhibitors, norepinephrine reuptake inhibi- tors, tramadol, opioids, steroids, topical analgesics containing lidocaine or capsaicin, and other prohibited medications) were discontinued. Both placebos used in this trial were prescribed twice daily to all subjects during the wash-out period. Subse- quently, eligible subjects were randomly assigned to receive the following treatments twice daily over 12 consecutive weeks:
GLA and placebo or ALA and placebo.
At the randomization visit after the 2-week wash-out period, the subjects were required to have a VAS score ≥4.0. A total of 124 patients were scheduled for randomization into two groups. Site investigators responsible for obtaining and analyz- ing data for the primary and secondary outcomes were blinded to the patient randomization procedure. Due to the nature of the study, all subjects and clinical staff were also blinded to the study group assignments. A treatment duration of 12 weeks was selected because there is a significant increase in the levels of plasma GLA and its metabolite dihomo-γ-linolenic acid (DGLA) after 4 weeks of treatment [20]. Additionally, a plateau in the TSS response is observed after 5 weeks of oral ALA treatment, which has a slower onset of efficacy [21].
Study medication
The study medication (Evoprim, 735 mg soft capsules; Dalim Biotech) contained 450 mg of evening primrose oil, which cor- responds to 40 mg of GLA per capsule; the dosages consisted of four capsules taken twice daily (320 mg/day of GLA) 30 minutes before breakfast and dinner. The active control medi- cation was 600 mg/day of ALA (Lipo-A HR, 828 mg tablets;
Dalim Biotech); the dosage consisted of one tablet taken once daily 30 minutes before breakfast. The placebo capsules and tablets for GLA and ALA were identical in appearance to the Evoprim capsules and Lipo-A HR tablets, respectively. Treat- ment duration was 12 weeks and treatment compliance was
defined as the intake of at least 80% of the trial medications.
No other agents for the treatment of DPN were allowed, but all subjects were advised to continue medication with any anti-di- abetic drug or drug for managing hypertension or dyslipid- emia during the study period.
Assessment of diabetic neuropathy
At the screening visit, all subjects were evaluated for DPN with the Michigan Neuropathy Screening Instrument questionnaire (MNSIQ) and physical examination (MNSIE) as well as the current perception threshold (CPT) test, which was measured using a Neurometer CPT device (Neurotron Inc., Baltimore, MD, USA). After completion of the MNSIQ, trained techni- cians examined the subjects for deformities, dry skin, callus, infections, ulcerations, vibration senses on the interphalangeal joints of both great toes, muscle strength reflexes using a ham- mer at the Achilles tendon on both ankles, and the monofila- ment test at the dorsum of both great toes [22]. The CPT was assessed as previously described [23]. Briefly, small electrodes were taped to the test sites (index fingers and great toes) and the responses to three different stimuli (2,000, 250, and 5 Hz) were recorded with increasing currents at each frequency.
Diagnosis of DPN
DPN was diagnosed based on the presence of either of the fol- lowing criteria: (1) an MNSIE score ≥2 or (2) symptoms of pain, burning, tingling, and/or loss of sensation and abnormal CPT results of the peroneal nerve at any frequency (reference ranges: 2.0 to 5.26 mA at 2,000 Hz, 0.62 to 2.11 mA at 250 Hz, and 0.3 to 1.73 mA at 5 Hz) [24]. These criteria are based on the recommendations of the Toronto Diabetic Neuropathy Ex- pert Group [25].
Assessment of outcomes and safety Primary outcome measures
The primary outcome measures included scores on the VAS and TSS, which were assessed as previously described [4,21].
The VAS and TSS scores were measured at screening, at base- line prior to the initiation of the study treatment, and after 4 and 12 weeks of treatment. The VAS is an 11-point numeric rating scale ranging from 0 to 10 (0=no pain and 10=the worst pain imaginable) that is based on the most recent 24-hour av- erage experience of pain. The TSS is a summation of symptom scores for stabbing pain, burning pain, paresthesia, and numb- ness by frequency (occasionally, often, or continuous) and in-
tensity (not present, mild, moderate, or severe) on which scores range from 0 to 14.64.
Secondary outcome measures
The MNSIQ and MNSIE scores, CPT test, modified Brief Pain Inventory for DPN (mBPI-DPN), and EuroQol-5 dimensions (EQ 5D) were conducted as previously described [4,22]. All neurological assessments were performed by trained investiga- tors under supervision of the study physician, who was a certi- fied endocrinologist with the medical board of internal medi- cine.
Safety analyses
Safety measures included the frequencies of treatment-emer- gent adverse drug reactions (TEADRs) and the monitoring of serious adverse events (SAEs) or other signs, including systolic and diastolic blood pressure levels, heart rate after 5 minutes of sitting at rest, body weight, and standard laboratory parame- ters; each of these variables was measured at the beginning and end of the study. Adverse events were monitored throughout the entire study, TEADRs were determined by study investiga- tors, and SAEs were defined by the protocol.
Laboratory assays
At each study site, blood samples were collected from the sub- jects following a 12-hour overnight fast via punctures of the forearm vein, and laboratory measurements were performed immediately after centrifugation and clotting. At each site, fast- ing serum glucose, creatinine, and lipid levels were measured using kits according to the manufacturer’s instructions. Low density lipoprotein cholesterol (LDL-C) levels were calculated using the Friedewald formula [26] and HbA1c levels were measured using high-performance liquid chromatography; all measurements were performed at baseline and at the final visit.
Sample size calculation
The sample size calculation was based on the primary efficacy variable (i.e., TSS scores) and the noninferiority of the GLA treatment group compared to the ALA treatment group. Based on the assumptions that the difference of the GLA treatment group was 3.776, the difference of the ALA treatment group was 2.7, and the common standard deviation (SD) was 1.76 with a noninferiority margin of δ2=0.054, 60 patients per group would have had a statistical power of 80% to confirm noninfe- riority using a two-sided significance level of P<0.05. The non-
inferiority margin was estimated based on a previous trial of ALA in Korea [27].
Statistical analysis
All randomized subjects that received at least one of the inves- tigation products were included in the present analyses. Addi- tionally, analyses based on the per-protocol (PP) set were per- formed to examine the robustness of the efficacy outcomes analysis; subjects who had major protocol deviations such as noncompliance with the study drug or the use of a prohibited medication were excluded from the PP analysis. Analyses based on the intent-to-treat set were performed to examine the degrees of robustness of the demographic information and the safety analysis. Independent t-tests for mean changes in values between the GLA and ALA groups and paired t-tests for changes between the baseline and 12-week assessments within each group were conducted to assess the efficacy outcomes and safety factors. Categorical variables, including demographic information and adverse events, were evaluated with chi- squared tests or Fisher’s exact tests. Additionally, 95% confi- dence intervals (CI) for treatment differences on the VAS and TSS (GLA-ALA) at week 12 were estimated; if the upper bounds of the 95% CI did not exceed the predefined noninferi- ority margins (δ1=0.51 and δ2=0.054, respectively), it was con- cluded that GLA was not inferior to ALA. All statistical analy- ses were conducted using SAS version 9.3 (SAS Institute, Cary, NC, USA).
RESULTS
The subject distribution throughout the trial is shown in Sup- plementary Fig. 2 [28]. Of the 124 subjects that were initially screened for this study, 24 were ineligible for randomization;
three patients did not meet the inclusion criteria, seven met the exclusion criteria, and 14 withdrew their consent. Thus, a total of 100 subjects entered the run-in phase. Of the 100 sub- jects who were randomly assigned to a group, 73 completed the trial and 27 (27%) discontinued participation during the treatment period. Of these 27 subjects, eight were withheld from the study due to the inclusion/exclusion criteria, seven withdrew consent, five did not comply with the treatment, five were taking prohibited medications during the trial period, one discontinued participation due to a dosing error, and one discontinued participation due to adverse events (Supplemen- tary Fig. 2).
Primary outcomes
The demographic and clinical characteristics of the subjects are shown in Table 1. There were no significant differences be- tween the groups in any of the baseline parameters or the mean VAS and TSS scores at baseline (total scores and individ- ual sub-scores) (Table 2). The outcomes were analyzed using a PP approach; i.e., only data from patients who continued with the randomized treatment were considered for the present analyses [29].
After the 12-week treatment period, there were significant reductions in the mean VAS score of each group compared to baseline (all P<0.001) but the scores of the two groups did not significantly differ from each other (P=0.137) (Table 3). In the GLA group, the mean VAS score at baseline was 5.26±1.17, compared to 2.94±1.71 after 12 weeks of treatment. In the ALA group, the mean VAS score at baseline was 5.58±1.35, compared to 3.92±2.12 after 12 weeks of treatment. The differ- Table 1. Baseline demographics and characteristics
Characteristic GLA (n=48) ALA (n=52) P value
Male sex 29 (60.4) 26 (50.0) 0.296
Age, yr 60.35±9.03 60.96±8.94 0.736
Duration of diabetes, yra 9.63±8.16 12.81±8.92 0.066 BMI, kg/m2 25.02±3.19 25.26±3.71 0.729 Systolic BP, mm Hg 126.69±12.65 128.94±9.82 0.320 Diastolic BP, mm Hg 75.63±8.32 75.37±7.08 0.867 FPG, mg/dL 129.71±30.52 134.71±46.92 0.526
HbA1c, % 6.96±0.88 7.25±1.17 0.169
BUN, mg/dL 15.68±4.41 16.26±6.38 0.593
S-Cr, mg/dL 0.84±0.21 0.83±0.22 0.882 Total cholesterol, mg/dL 146.50±27.23 158.90±35.57 0.055 Triglycerides, mg/dL 137.02±75.97 153.21±104.71 0.376 HDL-C, mg/dL 49.67±12.14 51.83±14.24 0.418 LDL-C, mg/dL 69.52±27.84 77.34±30.17 0.182
Statin 33 (68.75) 39 (75.00) 0.487
OHA 44 (91.67) 51 (98.08) 0.192
OHA+Insulin 6 (12.50) 12 (23.08) 0.169
Insulin 8 (16.67) 13 (25.00) 0.307
Values are presented as number (%) or mean±standard deviation.
GLA, γ-linolenic acid; ALA, α-lipoic acid; BMI, body mass index; BP, blood pressure; FPG, fasting plasma glucose; HbA1c, glycosylated he- moglobin; BUN, blood urea nitrogen; S-Cr, serum creatinine; HDL- C, high density lipoprotein cholesterol; LDL-C, low density lipopro- tein cholesterol; OHA, oral hypoglycemic agent.
aDuration of diabetes is from the time of diagnosis.
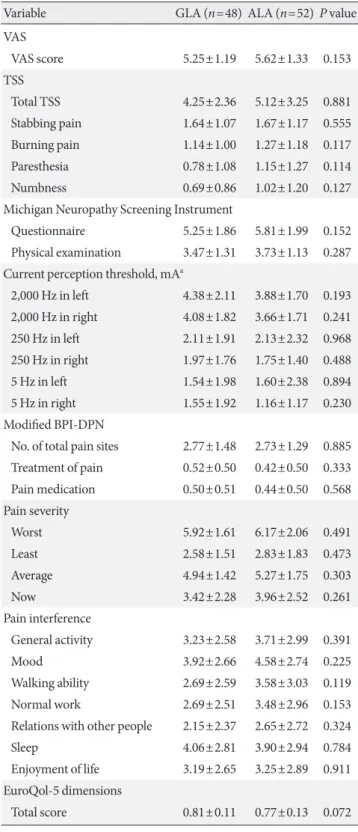
Table 2. Baseline primary and secondary outcome measures
Variable GLA (n=48) ALA (n=52) P value
VAS
VAS score 5.25±1.19 5.62±1.33 0.153
TSS
Total TSS 4.25±2.36 5.12±3.25 0.881
Stabbing pain 1.64±1.07 1.67±1.17 0.555 Burning pain 1.14±1.00 1.27±1.18 0.117 Paresthesia 0.78±1.08 1.15±1.27 0.114
Numbness 0.69±0.86 1.02±1.20 0.127
Michigan Neuropathy Screening Instrument
Questionnaire 5.25±1.86 5.81±1.99 0.152 Physical examination 3.47±1.31 3.73±1.13 0.287 Current perception threshold, mAa
2,000 Hz in left 4.38±2.11 3.88±1.70 0.193 2,000 Hz in right 4.08±1.82 3.66±1.71 0.241 250 Hz in left 2.11±1.91 2.13±2.32 0.968 250 Hz in right 1.97±1.76 1.75±1.40 0.488 5 Hz in left 1.54±1.98 1.60±2.38 0.894 5 Hz in right 1.55±1.92 1.16±1.17 0.230 Modified BPI-DPN
No. of total pain sites 2.77±1.48 2.73±1.29 0.885 Treatment of pain 0.52±0.50 0.42±0.50 0.333 Pain medication 0.50±0.51 0.44±0.50 0.568 Pain severity
Worst 5.92±1.61 6.17±2.06 0.491
Least 2.58±1.51 2.83±1.83 0.473
Average 4.94±1.42 5.27±1.75 0.303
Now 3.42±2.28 3.96±2.52 0.261
Pain interference
General activity 3.23±2.58 3.71±2.99 0.391
Mood 3.92±2.66 4.58±2.74 0.225
Walking ability 2.69±2.59 3.58±3.03 0.119 Normal work 2.69±2.51 3.48±2.96 0.153 Relations with other people 2.15±2.37 2.65±2.72 0.324
Sleep 4.06±2.81 3.90±2.94 0.784
Enjoyment of life 3.19±2.65 3.25±2.89 0.911 EuroQol-5 dimensions
Total score 0.81±0.11 0.77±0.13 0.072 Values are presented as mean±standard deviation.
GLA, γ-linolenic acid; ALA, α-lipoic acid; VAS, visual analogue scale;
TSS, total symptom score; BPI, brief pain inventory; DPN, diabetic peripheral neuropathy.
aPeroneal nerve, lower leg.
ences in the least-squares mean±SD of the VAS score after 12 weeks of treatment were −2.31±1.92 in the GLA group and
−1.66±1.81 in the ALA group. The treatment difference be- tween the two groups was −0.65 (95% CI, −1.526 to 0.213), and therefore, the upper bound of the 95% CI did not exceed the predefined noninferiority margin (δ1=0.51), which suggests the noninferiority of GLA compared to ALA in terms of the VAS score.
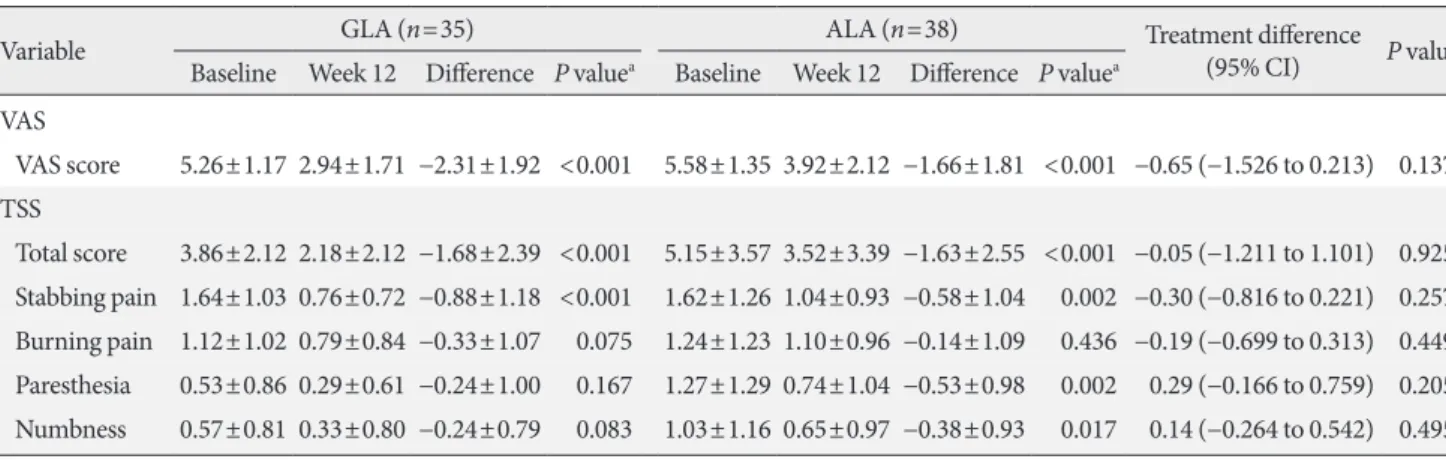
There were also significant reductions in the mean total TSS scores in both groups. In the GLA group, the mean total TSS scores significantly decreased from 3.86±2.12 at baseline to 2.18±2.12 after 12 weeks of treatment (P<0.001). In the ALA group, the mean total TSS scores significantly decreased from 5.15±3.35 at baseline to 3.52±3.39 after 12 weeks of treatment (P<0.001). The differences in the least-squares mean of the to- tal TSS score after 12 weeks of treatment were −1.68±2.39 in the GLA group and −1.63±2.55 in the ALA group, but the dif- ference in changes on the TSS was not significant between the two groups (P=0.925). The treatment difference between the two groups was −0.05 (95% CI, −1.211 to 1.101), and therefore, the upper bound of the 95% CI crossed the noninferiority margin (δ2=0.054), which suggests that treatment with GLA did not satisfy the criteria for noninferiority compared to treat- ment with ALA in terms of the TSS. After 12 weeks of treat- ment, the TSS sub-scores for stabbing pain exhibited signifi- cant reductions in both groups (both P<0.001), whereas only the ALA group showed significant reductions in the sub-scores for paresthesia (P=0.167 for GLA, P=0.002 for ALA) and numbness (P=0.083 for GLA, P=0.017 for ALA) compared to
baseline. The changes in the sub-scores for burning pain were not significant in either group (P=0.075 for GLA, P=0.436 for ALA) (Table 3). A response analysis after 12 weeks of treat- ment revealed that the percentages of clinical responders (a decrease in VAS or TSS score ≥40%) were 60.0% in the GLA group and 42.1% in the ALA group for the VAS and 60.0% in the GLA group and 44.7% in the ALA group for the TSS; there were no significant differences between the two groups (χ2, P=0.127 and P=0.192, respectively).
Secondary outcomes
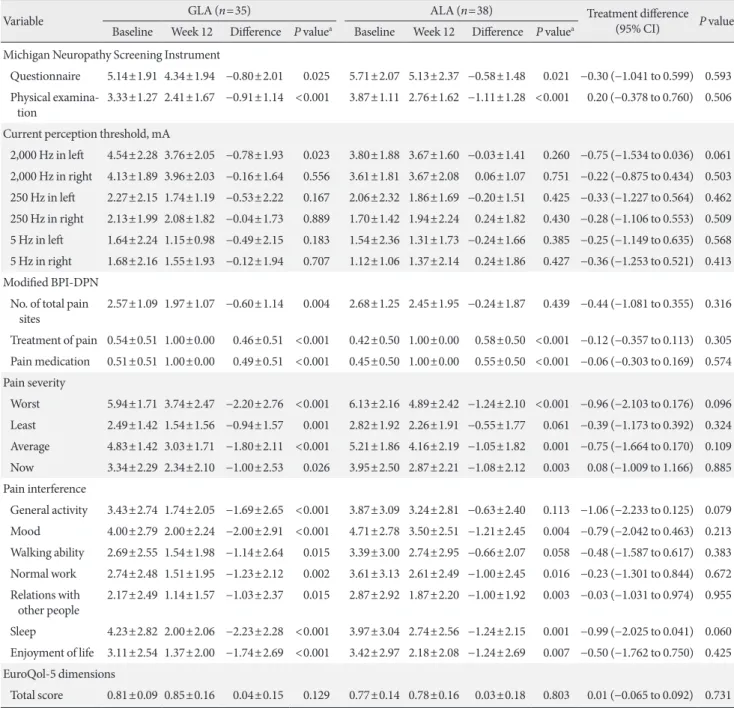
The mean levels of the subjects on the MNSIQ and MNSIE, all CPT measures, scores on the mBPI-DPN and EQ 5D at base- line, and scores on the mBPI-DPN and EQ 5D after 12 weeks treatment are provided in Table 4. There were no significant differences between the two groups at baseline, but there were similar significant improvements in the MNSIQ and MNSIE in both groups after 12 weeks of treatment. Of the mBPI-DPN measures, the items for pain severity (worst, average, and cur- rent pain) and pain interference (mood, normal work, rela- tionship, sleep, and enjoyment of life) significantly improved in both groups, whereas only the GLA group exhibited signifi- cant improvements in the total number of pain sites, the weak- est pain (pain severity item), general activity, and walking (pain interference item). There were no significant changes in any of the CPT measures, except at 2,000 Hz in the GLA group, or the mean EQ 5D scores from baseline to after 12 weeks of treatment in either group.
Table 3. Changes in primary outcomes from baseline to week 12
Variable GLA (n=35) ALA (n=38) Treatment difference
(95% CI) P valueb Baseline Week 12 Difference P valuea Baseline Week 12 Difference P valuea
VAS
VAS score 5.26±1.17 2.94±1.71 −2.31±1.92 <0.001 5.58±1.35 3.92±2.12 −1.66±1.81 <0.001 −0.65 (−1.526 to 0.213) 0.137 TSS
Total score 3.86±2.12 2.18±2.12 −1.68±2.39 <0.001 5.15±3.57 3.52±3.39 −1.63±2.55 <0.001 −0.05 (−1.211 to 1.101) 0.925 Stabbing pain 1.64±1.03 0.76±0.72 −0.88±1.18 <0.001 1.62±1.26 1.04±0.93 −0.58±1.04 0.002 −0.30 (−0.816 to 0.221) 0.257 Burning pain 1.12±1.02 0.79±0.84 −0.33±1.07 0.075 1.24±1.23 1.10±0.96 −0.14±1.09 0.436 −0.19 (−0.699 to 0.313) 0.449 Paresthesia 0.53±0.86 0.29±0.61 −0.24±1.00 0.167 1.27±1.29 0.74±1.04 −0.53±0.98 0.002 0.29 (−0.166 to 0.759) 0.205 Numbness 0.57±0.81 0.33±0.80 −0.24±0.79 0.083 1.03±1.16 0.65±0.97 −0.38±0.93 0.017 0.14 (−0.264 to 0.542) 0.495 Values are presented as mean±standard deviation.
GLA, γ-linolenic acid; ALA, α-lipoic acid; CI, confidence interval; VAS, visual analogue scale; TSS, total symptom score.
aAnalyzed by paired t-tests between baseline and week 12 in each group, banalyzed by independent t-tests assessing changes in values between the groups.
Table 4. Changes in secondary outcomes from baseline to week 12
Variable GLA (n=35) ALA (n=38) Treatment difference
(95% CI) P valueb Baseline Week 12 Difference P valuea Baseline Week 12 Difference P valuea
Michigan Neuropathy Screening Instrument
Questionnaire 5.14±1.91 4.34±1.94 −0.80±2.01 0.025 5.71±2.07 5.13±2.37 −0.58±1.48 0.021 −0.30 (−1.041 to 0.599) 0.593 P hysical examina-
tion 3.33±1.27 2.41±1.67 −0.91±1.14 <0.001 3.87±1.11 2.76±1.62 −1.11±1.28 <0.001 0.20 (−0.378 to 0.760) 0.506 Current perception threshold, mA
2,000 Hz in left 4.54±2.28 3.76±2.05 −0.78±1.93 0.023 3.80±1.88 3.67±1.60 −0.03±1.41 0.260 −0.75 (−1.534 to 0.036) 0.061 2,000 Hz in right 4.13±1.89 3.96±2.03 −0.16±1.64 0.556 3.61±1.81 3.67±2.08 0.06±1.07 0.751 −0.22 (−0.875 to 0.434) 0.503 250 Hz in left 2.27±2.15 1.74±1.19 −0.53±2.22 0.167 2.06±2.32 1.86±1.69 −0.20±1.51 0.425 −0.33 (−1.227 to 0.564) 0.462 250 Hz in right 2.13±1.99 2.08±1.82 −0.04±1.73 0.889 1.70±1.42 1.94±2.24 0.24±1.82 0.430 −0.28 (−1.106 to 0.553) 0.509 5 Hz in left 1.64±2.24 1.15±0.98 −0.49±2.15 0.183 1.54±2.36 1.31±1.73 −0.24±1.66 0.385 −0.25 (−1.149 to 0.635) 0.568 5 Hz in right 1.68±2.16 1.55±1.93 −0.12±1.94 0.707 1.12±1.06 1.37±2.14 0.24±1.86 0.427 −0.36 (−1.253 to 0.521) 0.413 Modified BPI-DPN
N o. of total pain
sites 2.57±1.09 1.97±1.07 −0.60±1.14 0.004 2.68±1.25 2.45±1.95 −0.24±1.87 0.439 −0.44 (−1.081 to 0.355) 0.316 Treatment of pain 0.54±0.51 1.00±0.00 0.46±0.51 <0.001 0.42±0.50 1.00±0.00 0.58±0.50 <0.001 −0.12 (−0.357 to 0.113) 0.305 Pain medication 0.51±0.51 1.00±0.00 0.49±0.51 <0.001 0.45±0.50 1.00±0.00 0.55±0.50 <0.001 −0.06 (−0.303 to 0.169) 0.574 Pain severity
Worst 5.94±1.71 3.74±2.47 −2.20±2.76 <0.001 6.13±2.16 4.89±2.42 −1.24±2.10 <0.001 −0.96 (−2.103 to 0.176) 0.096 Least 2.49±1.42 1.54±1.56 −0.94±1.57 0.001 2.82±1.92 2.26±1.91 −0.55±1.77 0.061 −0.39 (−1.173 to 0.392) 0.324 Average 4.83±1.42 3.03±1.71 −1.80±2.11 <0.001 5.21±1.86 4.16±2.19 −1.05±1.82 0.001 −0.75 (−1.664 to 0.170) 0.109 Now 3.34±2.29 2.34±2.10 −1.00±2.53 0.026 3.95±2.50 2.87±2.21 −1.08±2.12 0.003 0.08 (−1.009 to 1.166) 0.885 Pain interference
General activity 3.43±2.74 1.74±2.05 −1.69±2.65 <0.001 3.87±3.09 3.24±2.81 −0.63±2.40 0.113 −1.06 (−2.233 to 0.125) 0.079 Mood 4.00±2.79 2.00±2.24 −2.00±2.91 <0.001 4.71±2.78 3.50±2.51 −1.21±2.45 0.004 −0.79 (−2.042 to 0.463) 0.213 Walking ability 2.69±2.55 1.54±1.98 −1.14±2.64 0.015 3.39±3.00 2.74±2.95 −0.66±2.07 0.058 −0.48 (−1.587 to 0.617) 0.383 Normal work 2.74±2.48 1.51±1.95 −1.23±2.12 0.002 3.61±3.13 2.61±2.49 −1.00±2.45 0.016 −0.23 (−1.301 to 0.844) 0.672 R elations with
other people 2.17±2.49 1.14±1.57 −1.03±2.37 0.015 2.87±2.92 1.87±2.20 −1.00±1.92 0.003 −0.03 (−1.031 to 0.974) 0.955 Sleep 4.23±2.82 2.00±2.06 −2.23±2.28 <0.001 3.97±3.04 2.74±2.56 −1.24±2.15 0.001 −0.99 (−2.025 to 0.041) 0.060 Enjoyment of life 3.11±2.54 1.37±2.00 −1.74±2.69 <0.001 3.42±2.97 2.18±2.08 −1.24±2.69 0.007 −0.50 (−1.762 to 0.750) 0.425 EuroQol-5 dimensions
Total score 0.81±0.09 0.85±0.16 0.04±0.15 0.129 0.77±0.14 0.78±0.16 0.03±0.18 0.803 0.01 (−0.065 to 0.092) 0.731 Values are presented as mean±standard deviation.
GLA, γ-linolenic acid; ALA, α-lipoic acid; CI, confidence interval; BPI, brief pain inventory; DPN, diabetic peripheral neuropathy.
aAnalyzed by paired t-tests between baseline and week 12 in each group, banalyzed by independent t-tests assessing changes in values between the groups.
Safety
Regarding the laboratory parameters, there were no significant differences between the two groups in terms of body mass in- dex or the levels of HbA1c, fasting glucose, total cholesterol, LDL-C, or triglycerides between baseline and after 12 weeks of treatment. However, high density lipoprotein cholesterol levels
significantly decreased in the GLA group from 49.67±12.14 to 50.05±10.99 (P=0.04) (Table 5). Patients generally tolerated the treatment well, as no new safety concerns or events related to GLA were reported.
The numbers of patients experiencing TEADRs (total of 63 events in 44 subjects), which were defined as any event not
present prior to the initiation of treatment or any event already present that worsened in either intensity or frequency follow- ing exposure to the treatment, were 15 (31.2%) in the GLA group and 29 (55.8%) in the ALA group; the difference be- tween the two groups was significant (P=0.014). Most of the events (n=55, 87.3%) were considered to be transient and mild. The TEADRs that were reported in at least two subjects did not differ in frequency between the two groups (Supple- mentary Table 1). One GLA patient (0.02%) and one ALA (0.02%) patient discontinued the study treatment due to other causes (wrist fracture due to slipping and falling, and back pain due to a sprain, respectively); each adverse event was consid- ered to have an “unlikely” causal relationship with the study medication as judged by the investigator. SAEs occurred in one GLA patient who experienced gastrointestinal bleeding and chondromalacia of the medial femoral condyle in both knees.
DISCUSSION
The present study demonstrated that T2DM patients with DPN who were treated with GLA over 12 weeks showed im- provements in pain severity as measured by the VAS, and that GLA was noninferior to ALA. Additionally, the mean TSS score of the GLA group improved after 12 weeks of treatment, but none of the individual symptoms, except stabbing pain, ex- hibited a significant change compared to baseline. Although none of the TSS measures in the GLA group met the noninfe- riority criteria compared to ALA, the noninferiority of symp- tomatic improvements in DPN due to GLA compared to ALA
was supported by the secondary outcomes for efficacy. The scores on the MNSI, mBPI-DPN, and EQ 5D after 12 weeks of treatment did not differ significantly between the GLA and ALA groups. However, there were no changes in the CPT mea- sures (except at 2,000 Hz for GLA) or mean EQ 5D scores in either group. The overall treatment demonstrated a tolerable safety profile. A total of 55 mild adverse events were observed in 37 patients (22 events in 13 GLA subjects and 33 events in 24 ALA subjects), but all were transient and self-limited.
The pathogenesis and natural history of DPN remain largely unknown. However, hyperglycemia-triggered oxidative stress and defects in the microvasculature have complex interactions with neurovascular dysfunction, and both are associated with the progression of nerve damage, which makes it difficult or impossible to identify the favorable functional or structural ef- fects of potential therapeutic modalities [30,31]. More specifi- cally, the Neurological Assessment of Thioctic Acid in Diabetic Neuropathy (NATHAN) 1 trial showed that treatment with ALA (600 mg, once daily) slowed the progression of neuro- pathic deficits rather than improving these deficits, and that there were modest changes in measures of DPN in a placebo group after 4 years [30]. Another randomized trial observed improvements in neuropathic symptoms and neuropathic def- icits, such as summed median and sural sensory nerve con- duction velocities, in a placebo group after 1 year of observa- tion, and reported that these changes were associated with im- provements in metabolic variables, including glycemic control and serum triglyceride levels [32]. However, this study did not report differences in blood glucose or triglyceride levels be- Table 5. Changes in BMI, HbA1c, glucose, and lipid profiles
Variable GLA (n=48) ALA (n=52)
P valueb
Baseline 12 week P valuea Baseline 12 week P valuea
BMI, kg/m2 25.02±3.19 25.18±3.23 0.715 25.26±3.71 25.51±3.83 0.785 0.743
HbA1c, % 6.96±0.88 7.17±1.06 0.053 7.25±1.17 7.43±1.31 0.469 0.361
FPG, mg/dL 129.71±30.52 142.30±39.39 0.021 134.71±46.92 143.17±40.12 0.274 0.568
Total cholesterol, mg/dL 146.50±27.23 149.75±31.22 0.327 158.90±35.57 163.40±42.35 0.827 0.670 Triglyceride, mg/dL 137.02±75.97 130.10±67.79 0.243 153.21±104.71 150.67±80.20 0.941 0.878
HDL-C, mg/dL 49.67±12.14 50.05±10.99 0.040 51.83±14.24 51.10±14.28 0.353 0.572
LDL-C, mg/dL 69.52±27.84 74.05±28.40 0.217 77.34±30.17 80.66±35.10 0.703 0.407
Values are presented as mean±standard deviation.
BMI, body mass index; HbA1c, glycosylated hemoglobin; GLA, γ-linolenic acid; ALA, α-lipoic acid; FPG, fasting plasma glucose; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol.
aAnalyzed by paired t-tests between baseline and week 12 in each group, banalyzed by independent t-tests assessing changes in values between the groups.
tween the treatment groups or after the intervention.
GLA treatment in T2DM patients via either a dietary sup- plement (primrose oil) or a formulation has beneficial effects on neuropathy symptom scores as well as neurophysiological parameters, such as motor and sensory nerve conduction stud- ies and thermal threshold measurements [8,10,33]. The mech- anisms by which GLA improves neuropathic symptoms and performance in nerve conduction tests are largely dependent on its antioxidative and vasodilatory effects via its metabolites [8,33]. The metabolites of GLA, such as prostaglandin E1 [34], may be responsible for the antinociceptive effects of GLA on diabetes-induced nerve damage due to increases in neuronal phospholipids, free radical scavenging activities, and microcir- culation [7,35].
Furthermore, an animal study that employed a model of streptozotocin (STZ)-induced diabetic neuropathy showed that pretreatment with GLA increased motor nerve conduc- tion velocities in the sciatic-tibial conducting motor system and attenuated the STZ-induced hyperanalgesic response [17].
In that study, STZ-induced hyperalgesia was not dependent on the acute changes in hyperglycemia and the GLA treatments did not improve blood glucose levels; therefore, the antinoci- ceptive effects of GLA were thought be mediated by the neuro- protective, vasodilatory, and antioxidative properties of GLA independent of its effects on hyperglycemia. Collectively, these data suggest that disturbances in the metabolism of polyunsat- urated fatty acids from the n-6 pathway might have important implications for DPN, and that GLA treatment could poten- tially provide a source of essential fatty acids to protect against abnormal fatty acid metabolism. Additionally, these findings suggest that GLA could increase the capacity for antioxidation against impaired endoneurial microenvironments in the dam- aged nerves of T2DM patients.
In line with this observation, pathogenetic-based therapies in patients with DPN have been shown to improve symptom- atic pain scores. For example, the Symptomatic Diabetic Neu- ropathy study (SYDENY 2), which included 181 diabetic pa- tients (type 1 or 2) with symptomatic DPN (TSS >7.5 points), reported that treatment with once-daily oral doses of ALA (600 mg) for 5 weeks reduced pain (TSS: 51% compared to 32% in the placebo group) and significantly improved stabbing and burning pain, scores on the Neuropathy Symptoms and Change (NSC) scale, and patients’ global assessments of effica- cy [21]. Other studies have reported that improvements in neuropathic symptoms and deficits following treatment with
ALA may be related to improvements in nerve blood flow me- diated by antioxidant mechanisms [36,37]. This hypothesis was supported by the Irbesartan and Lipoic Acid in Endotheli- al Dysfunction (ISLAND) study, in which patients with meta- bolic syndrome received oral treatment with 300 mg of ALA [32]. The patients exhibited significant improvements in endo- thelium-dependent flow-mediated vasodilatation of the bra- chial artery accompanied by reductions in plasma levels of in- terleukin-6 and plasminogen activator-1. Therefore, future studies should address whether pathogenetic-based therapies such as ALA or GLA will result in symptomatic relief that is mediated, at least in part, by improvements in the development and/or progression of DPN.
The present noninferiority study demonstrated that GLA was no worse for pain relief (as measured by the VAS and TSS) than ALA as an active comparator according to the noninferi- ority margin. A previous Korean study investigating the effica- cy and safety of ALA in patients with DPN (n=61) found that treatment with oral ALA (600 mg/day) improved TSS scores at 4 weeks (4.4±1.7) and 8 weeks (3.1±1.7, P<0.01) compared to baseline (5.8±1.8), with tolerable safety [27]. Additionally, this study showed that individual symptoms such as pain, burning, paresthesia, and numbness improved after 8 weeks of treat- ment (all P<0.01). Similarly, another Korean study (n=38) showed that TSS scores significantly decreased at 4 weeks after treatment with ALA (600 mg, once daily) and further de- creased after 8 weeks of treatment [38]. Based on the criterion of a change in TSS score ≥30% from baseline, the response rates in these studies were 77.3% and 71.4%, respectively. How- ever, these open-label studies were neither randomized nor placebo-controlled. In the present noninferiority study, a PP analysis was conducted to protect against the risk of type I er- ror that is associated with intention-to-treat analyses [39]. The present results showed that the CIs for the treatment effects were 0.500 (δ1) for the VAS and 0.051 (δ2) for the TSS as pri- mary outcomes; the margins of noninferiority were pre-speci- fied. Thus, based on VAS scores, GLA improved neuropathic symptoms in terms of relative efficacy compared to ALA for the treatment of DPN. There was no placebo arm due to the nature of the present study, thus it was possible to use the lower bound of the 95% CI to establish an efficacy advantage over placebo. As a result, it was confirmed that GLA had a clinically relevant superiority over placebo.
The cutoffs for the response rates of the outcome measures used for interventional studies of painful DPN have yet to be
fully clarified. However, most studies have employed a re- sponse rate ranging from 30% to 50% [40]. In the present study, the response rate was defined as a ≥40% reduction in VAS score after 12 weeks of treatment. The GLA group had a 60.0% response, whereas the ALA group had a 42.1% response (P=0.127). A meta-analysis of intravenous ALA (600 mg/day for 3 weeks; n=1,258) for the treatment of DPN found that TSS scores exhibited a relative decrease of 24.1% from baseline, with 52.7% considered as responsive; i.e., ≥50% improvement in TSS score compared to 36.9% in the placebo group [18]. In that study, the relative difference between scores at baseline and at the end of the 12-week ALA treatment period was 31.7%. Therefore, the effects of ALA on neuropathic symptoms in patients with DPN observed in the present study appear to be comparable to those observed in previous studies. Further studies should be conducted to develop a uniform, validated, and internationally accepted range of outcome measures to compare the efficacies of treatments for painful DPN.
The present study had several critical limitations that should be considered. First, the lack of homogeneity among the sub- jects in terms of the clinical stage and degree of DPN and co- morbidities, such as glycemic control, concomitant micro-or macrovascular complications, and emotional stress or depres- sion, could be a major confounding factor. For example, estima- tions of the characteristics and/or severity of DPN-related pain vary within individuals during the course of DPN [41,42]. Sec- ond, the reasons for the discrepancies between the effects of GLA and ALA on the mBPI-DPN sub-scores were not fully un- derstood. The differential effects of these antioxidative treat- ment modalities on the pathophysiology of nerve damage and how they result in different intensities of symptom profiles should be addressed in further studies. Third, the natural histo- ry and diabetes duration-dependent symptom phenotypes vary among patients with DPN [25]. The progressive degeneration and loss of peripheral nerve fibers in patients with T2DM re- sults in abnormal excitability or insensitivity, which are associ- ated with various troublesome issues in the lower extremities [25]. Therefore, the present 12-week treatment period with GLA or ALA may have been too short to allow for the achieve- ment of clinically meaningful changes in neuropathic deficits that were observed previous studies [43,44]. Additionally, the favorable effects of 12 weeks of treatment with either GLA or ALA in the present study may not translate to the long-term management of patients with DPN. Finally, the present results regarding the efficacies of the medications for painful DPN were
heterogeneous, and it will be difficult to directly compare these results with those of other studies. It is possible that the difficul- ties in defining and measuring neuropathic endpoints are asso- ciated with the heterogeneity of patients in terms of the diag- nostic definition and clinical stages of DPN, metabolic control status, type of diabetes, the variety and non-identical attributes of symptom phenotypes, and the different treatment modalities for DPN [42]. Nonetheless, the present findings of improve- ments in neuropathic symptoms and the tolerability of the treat- ments in the absence of SAEs are encouraging, because GLA and ALA could be considered pathogenesis-based and symp- tomatic therapies. Additionally, the mechanism(s) of GLA and/
or ALA underlying the improvements in neuropathic symp- toms of GLA and/or ALA are not determined in this study, fur- ther studies through measurement of other serum markers for inflammatory or oxidative stress or using in vivo are needed.
In conclusion, the present trial demonstrated that the mag- nitude of efficacy of GLA treatment on pain severity (as mea- sured by the VAS) over 12 weeks was comparable to that of ALA. Additionally, both treatments were well-tolerated and, therefore, GLA appears to be a reasonable treatment option for Korean patients with painful DPN. The present findings should be further validated by larger well-designed and high quality randomized controlled trials.
SUPPLEMENTARY MATERIALS
Supplementary materials related to this article can be found online at https://doi.org/10.4093/dmj.2019.0099.
CONFLICTS OF INTEREST
This study was supported by a grant from Dalin Biotech Korea Co. Ltd. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manu- script.
AUTHOR CONTRIBUTIONS
Conception or design: J.C.W., C.H.K., T.S.P.
Acquisition, analysis, or interpretation of data: J.C.W., H.S.K., S.S.M., S.W.C., C.H.K., I.B.P., I.J.K., J.L., B.Y.C., T.S.P.
Drafting the work or revising: J.C.W., C.H.K., T.S.P.
Final approval of the manuscript: J.C.W., T.S.P.
ORCID
Jong Chul Won https://orcid.org/0000-0002-2219-4083 Tae Sun Park https://orcid.org/0000-0001-7216-8468
ACKNOWLEDGMENTS
We thank Da-Yeong Jeong (Healthcare Claims & Management Inc., Jeonju, Republic of Korea) of data management and sta- tistical analysis.
REFERENCES
1. Ogurtsova K, da Rocha Fernandes JD, Huang Y, Linnenkamp U, Guariguata L, Cho NH, Cavan D, Shaw JE, Makaroff LE.
IDF diabetes atlas: global estimates for the prevalence of diabe- tes for 2015 and 2040. Diabetes Res Clin Pract 2017;128:40-50.
2. Won JC, Lee JH, Kim JH, Kang ES, Won KC, Kim DJ, Lee MK.
Diabetes fact sheet in Korea, 2016: an appraisal of current sta- tus. Diabetes Metab J 2018;42:415-24.
3. Won JC, Kwon HS, Kim CH, Lee JH, Park TS, Ko KS, Cha BY.
Prevalence and clinical characteristics of diabetic peripheral neuropathy in hospital patients with type 2 diabetes in Korea.
Diabet Med 2012;29:e290-6.
4. Kim SS, Won JC, Kwon HS, Kim CH, Lee JH, Park TS, Ko KS, Cha BY. Prevalence and clinical implications of painful diabetic peripheral neuropathy in type 2 diabetes: results from a nation- wide hospital-based study of diabetic neuropathy in Korea. Di- abetes Res Clin Pract 2014;103:522-9.
5. Boulton AJ, Vinik AI, Arezzo JC, Bril V, Feldman EL, Freeman R, Malik RA, Maser RE, Sosenko JM, Ziegler D; American Di- abetes Association. Diabetic neuropathies: a statement by the American Diabetes Association. Diabetes Care 2005;28:956- 62.
6. Ziegler D, Rathmann W, Meisinger C, Dickhaus T, Mielck A;
KORA Study Group. Prevalence and risk factors of neuropath- ic pain in survivors of myocardial infarction with pre-diabetes and diabetes. The KORA Myocardial Infarction Registry. Eur J Pain 2009;13:582-7.
7. Benatti P, Peluso G, Nicolai R, Calvani M. Polyunsaturated fatty acids: biochemical, nutritional and epigenetic properties. J Am Coll Nutr 2004;23:281-302.
8. Horrobin DF. Essential fatty acids in the management of im- paired nerve function in diabetes. Diabetes 1997;46 Suppl 2:S90-3.
9. Brenner RR. Nutritional and hormonal factors influencing de- saturation of essential fatty acids. Prog Lipid Res 1981;20:41-7.
10. Keen H, Payan J, Allawi J, Walker J, Jamal GA, Weir AI, Hen- derson LM, Bissessar EA, Watkins PJ, Sampson M, Gale EAM, Scarpello J, Boddie HG, Hardy KJ, Thomas PK, Misra P, Ha- lonen JP; The γ-Linolenic Acid Multicenter Trial Group. Treat- ment of diabetic neuropathy with gamma-linolenic acid. The gamma-Linolenic Acid Multicenter Trial Group. Diabetes Care 1993;16:8-15.
11. Cameron NE, Cotter MA. Metabolic and vascular factors in the pathogenesis of diabetic neuropathy. Diabetes 1997;46 Suppl 2:S31-7.
12. Ametov AS, Barinov A, Dyck PJ, Hermann R, Kozlova N, Li- tchy WJ, Low PA, Nehrdich D, Novosadova M, O’Brien PC, Reljanovic M, Samigullin R, Schuette K, Strokov I, Tritschler HJ, Wessel K, Yakhno N, Ziegler D; SYDNEY Trial Study Group. The sensory symptoms of diabetic polyneuropathy are improved with alpha-lipoic acid: the SYDNEY trial. Diabetes Care 2003;26:770-6.
13. Ziegler D, Sohr CG, Nourooz-Zadeh J. Oxidative stress and antioxidant defense in relation to the severity of diabetic poly- neuropathy and cardiovascular autonomic neuropathy. Diabe- tes Care 2004;27:2178-83.
14. Bril V, Hirose T, Tomioka S, Buchanan R; Ranirestat Study Group. Ranirestat for the management of diabetic sensorimo- tor polyneuropathy. Diabetes Care 2009;32:1256-60.
15. Ropper AH, Gorson KC, Gooch CL, Weinberg DH, Pieczek A, Ware JH, Kershen J, Rogers A, Simovic D, Schratzberger P, Kirchmair R, Losordo D. Vascular endothelial growth factor gene transfer for diabetic polyneuropathy: a randomized, dou- ble-blinded trial. Ann Neurol 2009;65:386-93.
16. Vinik AI, Bril V, Kempler P, Litchy WJ, Tesfaye S, Price KL, Ba- styr EJ 3rd; MBBQ Study Group. Treatment of symptomatic diabetic peripheral neuropathy with the protein kinase C beta- inhibitor ruboxistaurin mesylate during a 1-year, randomized, placebo-controlled, double-blind clinical trial. Clin Ther 2005;
27:1164-80.
17. Nishikant N, Singh J, Sood S, Vijayshanker V. Effect of gamma linolenic acid pretreatment on diabetic neuropathy in rats. Int J Basic Clin Pharmacol 2013;2:320-5.
18. Ziegler D, Nowak H, Kempler P, Vargha P, Low PA. Treatment of symptomatic diabetic polyneuropathy with the antioxidant alpha-lipoic acid: a meta-analysis. Diabet Med 2004;21:114-21.
19. Han T, Bai J, Liu W, Hu Y. A systematic review and meta-analy- sis of α-lipoic acid in the treatment of diabetic peripheral neu-
ropathy. Eur J Endocrinol 2012;167:465-71.
20. Simon D, Eng PA, Borelli S, Kagi R, Zimmermann C, Zahner C, Drewe J, Hess L, Ferrari G, Lautenschlager S, Wuthrich B, Schmid-Grendelmeier P. Gamma-linolenic acid levels corre- late with clinical efficacy of evening primrose oil in patients with atopic dermatitis. Adv Ther 2014;31:180-8.
21. Ziegler D, Ametov A, Barinov A, Dyck PJ, Gurieva I, Low PA, Munzel U, Yakhno N, Raz I, Novosadova M, Maus J, Samigul- lin R. Oral treatment with alpha-lipoic acid improves symp- tomatic diabetic polyneuropathy: the SYDNEY 2 trial. Diabe- tes Care 2006;29:2365-70.
22. Feldman EL, Stevens MJ, Thomas PK, Brown MB, Canal N, Greene DA. A practical two-step quantitative clinical and elec- trophysiological assessment for the diagnosis and staging of di- abetic neuropathy. Diabetes Care 1994;17:1281-9.
23. Park JH, Won JC. Patterns of nerve conduction abnormalities in patients with type 2 diabetes mellitus according to the clini- cal phenotype determined by the current perception threshold.
Diabetes Metab J 2018;42:519-28.
24. Prendergast JJ, Miranda G, Sanchez M. Improvement of senso- ry impairment in patients with peripheral neuropathy. Endocr Pract 2004;10:24-30.
25. Tesfaye S, Boulton AJ, Dyck PJ, Freeman R, Horowitz M, Kem- pler P, Lauria G, Malik RA, Spallone V, Vinik A, Bernardi L, Valensi P; Toronto Diabetic Neuropathy Expert Group. Dia- betic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care 2010;33:
2285-93.
26. Roberts WC. The Friedewald-Levy-Fredrickson formula for calculating low-density lipoprotein cholesterol, the basis for lipid-lowering therapy. Am J Cardiol 1988;62:345-6.
27. Park CY, Kim YS, Oh SJ, Woo JT, Kim SW, Yang IM, Kim JW, Choi YK. Treatment of symptomatic diabetic peripheral neu- ropathy with thioctic acid (Thioctacid(R)). J Korean Diabetes Assoc 2001;2:63-74.
28. Schulz KF, Altman DG, Moher D; CONSORT Group. CON- SORT 2010 statement: updated guidelines for reporting paral- lel group randomized trials. Ann Intern Med 2010;152:726-32.
29. Staszewski S, Keiser P, Montaner J, Raffi F, Gathe J, Brotas V, Hicks C, Hammer SM, Cooper D, Johnson M, Tortell S, Cutrell A, Thorborn D, Isaacs R, Hetherington S, Steel H, Spreen W;
CNAAB3005 International Study Team. Abacavir-lamivudine- zidovudine vs indinavir-lamivudine-zidovudine in antiretrovi- ral-naive HIV-infected adults: a randomized equivalence trial.
JAMA 2001;285:1155-63.
30. Ziegler D, Low PA, Litchy WJ, Boulton AJ, Vinik AI, Freeman R, Samigullin R, Tritschler H, Munzel U, Maus J, Schutte K, Dyck PJ. Efficacy and safety of antioxidant treatment with α-lipoic acid over 4 years in diabetic polyneuropathy: the NA- THAN 1 trial. Diabetes Care 2011;34:2054-60.
31. Tesfaye S, Tandan R, Bastyr EJ 3rd, Kles KA, Skljarevski V, Price KL; Ruboxistaurin Study Group. Factors that impact symptomatic diabetic peripheral neuropathy in placebo-ad- ministered patients from two 1-year clinical trials. Diabetes Care 2007;30:2626-32.
32. Sola S, Mir MQ, Cheema FA, Khan-Merchant N, Menon RG, Parthasarathy S, Khan BV. Irbesartan and lipoic acid improve endothelial function and reduce markers of inflammation in the metabolic syndrome: results of the Irbesartan and Lipoic Acid in Endothelial Dysfunction (ISLAND) study. Circulation 2005;111:343-8.
33. Jamal GA, Carmichael H. The effect of gamma-linolenic acid on human diabetic peripheral neuropathy: a double-blind pla- cebo-controlled trial. Diabet Med 1990;7:319-23.
34. Carter JP. Gamma-linolenic acid as a nutrient. Food Technol 1988;42:72-82.
35. Omran OM. Histopathological study of evening primrose oil effects on experimental diabetic neuropathy. Ultrastruct Pathol 2012;36:222-7.
36. Nagamatsu M, Nickander KK, Schmelzer JD, Raya A, Wittrock DA, Tritschler H, Low PA. Lipoic acid improves nerve blood flow, reduces oxidative stress, and improves distal nerve con- duction in experimental diabetic neuropathy. Diabetes Care 1995;18:1160-7.
37. Coppey LJ, Gellett JS, Davidson EP, Dunlap JA, Lund DD, Yor- ek MA. Effect of antioxidant treatment of streptozotocin-in- duced diabetic rats on endoneurial blood flow, motor nerve conduction velocity, and vascular reactivity of epineurial arte- rioles of the sciatic nerve. Diabetes 2001;50:1927-37.
38. Hahm JR, Kim BJ, Kim KW. Clinical experience with thioctac- id (thioctic acid) in the treatment of distal symmetric polyneu- ropathy in Korean diabetic patients. J Diabetes Complications 2004;18:79-85.
39. Piaggio G, Elbourne DR, Altman DG, Pocock SJ, Evans SJ;
CONSORT Group. Reporting of noninferiority and equiva- lence randomized trials: an extension of the CONSORT state- ment. JAMA 2006;295:1152-60.
40. Veves A, Malik RA. Diabetic neuropathy: clinical manage- ment. Dordrecht: Springer Science & Business Media; 2008.
41. Boulton AJ. Whither clinical research in diabetic sensorimotor
peripheral neuropathy? Problems of end point selection for clinical trials. Diabetes Care 2007;30:2752-3.
42. Dyck PJ, Norell JE, Tritschler H, Schuette K, Samigullin R, Ziegler D, Bastyr EJ 3rd, Litchy WJ, O’Brien PC. Challenges in design of multicenter trials: end points assessed longitudinally for change and monotonicity. Diabetes Care 2007;30:2619-25.
43. Dyck PJ, Davies JL, Litchy WJ, O’Brien PC. Longitudinal as-
sessment of diabetic polyneuropathy using a composite score in the Rochester Diabetic Neuropathy Study cohort. Neurolo- gy 1997;49:229-39.
44. Diabetic polyneuropathy in controlled clinical trials: consensus report of the Peripheral Nerve Society. Ann Neurol 1995;38:
478-82.