31 서 론
전립선특이항원 (prostate specific antigen; PSA)은 전립선
상피세포에서 생산되는 물질로 이의 혈중농도는 전립선비 대증, 요폐, 전립선염, 전립선 마사지 후, 경요도 전립선절제 술 후, 전립선 조직생검 후 등과 같은 양성질환 및 특정상황 에서도 증가되지만 전립선암에서 특징적으로 증가하므로
Elevation of Serum Prostate Specific Antigen in Subclinical Prostatitis: The Role of Pathology of Inflammation
Sung On Lee, In Rae Cho, Keon Cheol Lee, Han Seong Kim1 From the Departments of Urology and 1Pathology, Inje University College of Medicine, Gimhae, Korea
Purpose: We evaluated the correlation of the pathologic diagnosis, in- cluding the grade or location of the inflammation on a prostate biopsy specimen, to the serum prostate-specific antigen (PSA) level.
Materials and Methods: 172 patients (the patients' PSA was≥4ng/ml) who received prostate biopsy at our department from January 2000 to August 2003 were retrospectively studied. The pre-biopsy PSA and pathol- ogy, including the diagnoses and inflammatory patterns, were analyzed.
The pathologic patterns of inflammation were divided as acute or chronic by the predominant inflammatory cell type; especially, the chronic inflam- mation was divided by grade or location, and then this was reviewed by 1 pathologist. Chronic Inflammation was graded as I, II or III according to the severity of inflammation. The PSA levels were compared among the grades. The presence or absence of chronic inflammation was checked in the periglandular, stromal and perivascular areas, respectively. The PSA levels were compared between the presence and absence of inflammation at each location.
Results: Among 172 patients, the number of patients with prostate cancer was 37 (21.5%), and 68 patients had only BPH (39.5%), 27 had only prostatitis (15.7%) and 40 patients had benign prostatic hyperplasia (BPH) with prostatitis (23.3%). The number of patients with any prostatitis was 67 (39.0%). The age of the patients was 68.4±8.7 years (45-91), the serum PSA was 13.30±14.38ng/ml (4.30-102.48), and the prostate size was 49.5±
21.1ml (20-126). One case of BPH with prostatitis had a PSA level above 100ng/ml. Among the 67 specimens that showed prostatitis, 16 patients had histologically acute inflammation (23.9%) and 51 patients had chronic inflammation (76.1%). The PSA levels of the acute or chronic inflammation patients were 24.04±25.95ng/ml (4.46-102.48) and 9.93±4.73ng/ml (4.3- 21.12, p=0.047), respectively. The PSA levels were not different among the 3 grades of chronic inflammation. In periglandular, stromal and perivas- cular locations, the PSA levels were not different between the presence and absence of chronic inflammation.
Conclusions: About 39% of the prostate biopsy specimens showed pros- tatitis. The PSA level was higher for the acute inflammation than for the chronic inflammation. However, there was no difference in PSA levels among the each of the grades or locations of chronic prostatic inflam- mation. (Korean J Urol 2006;47:31-36)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Key Words: Prostatitis, Prostate-specific antigen, Pathology
대한비뇨기과학회지 제 47 권 제 1 호 2006
인제대학교 의과대학
비뇨기과학교실, 1병리학교실
이승언․조인래․이건철․김한성1
접수일자:2005년 7월 12일 채택일자:2005년 8월 19일
교신저자: 조인래
인제대학교 일산백병원 비뇨기과
경기도 고양시 일산서구 대화동 2240
ꂕ 411-806 TEL: 031-910-7230 FAX: 031-910-7239 E-mail: ircho@ilsanpaik.
ac.kr
본 논문은 2004년도 인제대학교 학술연구 비 보조에 의한 것임.
전립선암의 진단 및 추적 검사에 유용하게 이용되고 있다.1 PSA를 상승시키는 원인 중의 하나인 전립선염은 임상 및 조직검사표본에서 흔히 접할 수 있는 질환인데 전립선염에
서 혈청 PSA가 상승하는 기전은 정확히 알려지지는 않았지 만, Brawer 등2은 염증세포가 전립선 선조직과 전신 순환계 사이의 해부학적 장벽을 파괴하여 PSA가 상승한다는 누출 현상 (leak phenomenon)을 제시하여 전립선염에서의 PSA 상승을 설명하였다.
그러나 전립선염에서 염증양상에 따른 PSA의 변화를 분 석한 논문은 빈약한 실정이며3 무증상 혹은 경미한 임상증 상을 가지는 전립선염 환자에서 염증의 부위나 정도에 따 른 PSA 변화를 고찰한 국내 보고는 없는 실정이다.
이에 저자들은 전립선염의 조직학적 양상이 PSA 증가와 어떠한 연관이 있는지를 알기 위해 혈중 PSA가 높아서 전 립선생검을 받았던 환자들을 후향적으로 검토하여 생검조 직의 병리소견에서 염증 유무 및 조직학적 양상을 분석하여 각각의 경우에서 PSA에 미치는 영향을 비교 분석하였다.
대상 및 방법
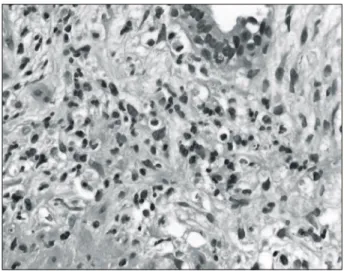
2000년 1월부터 2003년 8월까지 본원 비뇨기과에 내원하 였던 환자 중에서 혈중 PSA가 4ng/ml 이상으로 전립선생검 Fig. 1. Acute prostatic inflammation. Some neutrophiles are clus-
tered in the periglandular stromal tissue (H&E, x400).
A
C
B
Fig. 2. (A) Mild (grade I) chronic prostatic inflammation. A few mononuclear lymphoid cells are noted in the periglandular tissue
(H&E, x200). (B) Moderate (grade II) chronic prostatic inflam- mation. A moderate number of mononuclear cells are found in the periglandular and perivascular areas (H&E, x200). (C) Severe (grade III) chronic prostatic inflammation. The periglandular tis- sue is infiltrated by mononuclear chronic inflammatory cells (H&E, x200).
을 받은 180명 중에서 방광염이나 전립선염으로 치료 받았 던 환자들을 제외한 172명을 대상으로 후향적으로 분석하 였다. PSA는 Modular E-170TM(Roche, Basel, Swiss)을 사용 하여 Electro-Chemi-Luminescence-Immuno-Assay 방법으로 측정하였고, 전립선 조직검사는 환자가 측와위를 취한 상 태에서 경직장초음파 유도하에 18gauge 침을 장착한 생검 총을 이용하여 시행하였으며, 분석에 포함된 전립선생검은 초생검이었으며, 병리소견은 1명의 병리학자가 분석하였 다. 또한 이 중에서 전립선암은 없으면서 전립선비대증의 유무에 관계없이 전립선염 소견을 보인 무증상 전립선염 (NIH 분류 category IV) 67명을 선별하여 생검 전 PSA치와 생검으로 얻은 전립선조직의 염증소견을 분석하였다.
전립선염은 조직학적으로 급성 (다핵 백혈구의 침윤)과 만성 (대식세포, 림프구, 형질세포 등의 침윤)으로 구분하였 고 (Fig. 1), 만성인 경우 염증의 정도를 Irani 등3이 제안한 four-point scale에 근거하여 grade 0 (염증세포의 침윤이 없 는 경우), grade I (기질 내에 군데군데 소수의 림프구침윤만 보일 경우), grade II (중등도의 염증세포 침윤을 보이지만 림프 여포의 형성이 없는 경우), grade III (광범위한 염증세
포의 침윤을 보이면서 융합되어 림프 여포를 형성하는 경 우)의 4단계로 구분하였고 (Fig. 2), 염증이 존재하지 않는 grade 0 외에 3가지 grade에 따른 각각의 PSA치를 비교분석 하였다.
염증의 부위별 분석에서는 peri-gland, stroma, peri-vessel 등 세 군데로 구분하여 (Fig. 3) 각 부위에서 염증의 유무를 조사하여 각 부위별 염증 존재의 유무에 따라 PSA가 차이 가 있는지를 비교하였다. 통계적 유의성은 Student's t-test (unpaired)와 ANOVA를 이용하였고, p값이 0.05 미만인 경 우를 유의하다고 판정하였다.
결 과
172명 중 전립선암이 21.5%, 전립선비대증만 있는 경우가 39.5%, 전립선염만 있는 경우가 15.7%, 전립선염과 전립선 비대증이 병발된 경우가 23.3%로 무증상 전립선염 환자는 39.0% (67명)였다. 이 중 전립선염 소견을 보인 67명 환자들 의 평균 나이는 68세 (45-91), 혈청 PSA는 13.30ng/ml (4.30- 102.48), 전립선 크기는 49.5ml (20-126) 였다 (Table 1). PSA
A
C
B
Fig. 3. (A) Periglandular chronic inflammation of the prostate (H&E, x200). (B) Stromal chronic inflammation of the prostate (H&E, x200). (C) Perivascular chronic inflammation of the prostate (H&E, x200).
치를 10, 10-100, 100 ng/ml 이상으로 분류한 결과에서 전립 선염과 전립선비대증이 병발된 1명에서는 PSA치가 100ng/
ml 이상이었다 (Table 2).
무증상 전립선염 67명 중 조직학적으로 16명 (23.9%)이 급성, 51명 (76.1%)이 만성이었고 이들의 PSA치는 각각 24.04±25.95ng/ml (4.46-102.48)와 9.93±4.73ng/ml (4.3-21.12) 로 급성인 경우가 만성인 경우보다 더 높았다 (p=0.047). 51 명의 만성염증 중 15명이 grade I, 24명이 grade II, 12명이 grade III였고, 각 군 간의 PSA치 비교에서 의의있는 차이는 없었다 (p=0.979, Table 3). 또한 염증의 부위별 분석에서 각 각의 부위별 염증의 유무에 따른 PSA의 차이는 없었다 (Table 4).
고 찰
PSA는 gamma-semino protein으로 Hara 등4이 정장액에서 분리한 이후 Wang 등5이 분자량 33,000 (Gel filtration)-34,000 (SDS-PAGE) dalton의 항원을 정상인과 전립선비대증 및 전 립선암 환자의 조직에서 정제하고 전립선에 대한 특이성이 있음을 처음으로 발견하여 전립선암에 대한 종양지표 (tumor marker)로서의 가능성을 보고하였다. 이후 Papsidero 등6이 전립선암 환자의 혈청에서 PSA의 존재를 확인한 이 후 임상에 도입되어 최근 20년간 초기 전립선암의 진단과 전립선암 환자의 추적관찰에 이용되고 있다. 하지만 PSA는 전립선 상피세포에서 분비되는 serine protease로서7 전립선 뿐만 아니라 요도주위선, 유선조직, 유방암조직, 양수 등에 서도 분비되며8 종양 특이지표가 아닌 관계로 전립선암뿐 만 아니라 전립선비대증, 전립선염 등의 양성전립선 질환 과 전립선생검, 직장수지검사, 급성요폐, 사정 등에 의해서 도 영향을 받는다.9,10
Dalton 등11이 급성전립선염이 있는 2명의 환자 (PSA: 10.3, 22.6ng/ml)에서 항생제 사용 후 PSA가 정상화 (PSA: 2.6, 0.6 ng/ml)된 증례를 처음 발표한 후 급성전립선염 환자에서 Table 1. The patients’ demographic characteristics for each patho-
logical diagnosis that was obtained from the prostate biopsy specimens
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Pathologic No. of Prostatic
Age (yr) PSA (ng/ml)
diagnosis patients (%) volume (ml)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Prostatic
37 (21.5) 72.8±7.6 187.01±542.59 43.1±17.9 carcinoma
BPH 68 (39.5) 68.1±8.2 5.17±18.22 54.9±26.0 Prostatitis 27 (15.7) 66.4±9.3 10.64±5.97 42.7±15.3 Prostatitis
40 (23.3) 69.8±8.0 15.10±17.83 54.0±23.4 +BPH
Any pro-
67 (39.0) 68.4±8.7 13.30±14.38 49.5±21.1 statitis
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Total 172 (100) 69.2±8.4 51.41±259.35 50.2±22.9 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ PSA: prostate-specific antigen, BPH: benign prostatic hyperplasia
Table 2. Stratification of PSA levels for each pathological diagnosis ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
PSA levels 4-10 10-100 100≤
Total
(ng/ml) (%) (%) (%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Prostatic
10 (11.1) 17 (24.3) 10 (83.3) 37 (21.5) carcinoma
BPH 42 (46.7) 25 (35.7) 1 (8.3) 68 (39.5) Prostatitis 16 (17.8) 11 (15.7) 0 (0.0) 27 (15.7) Prostatitis+BPH 22 (24.4) 17 (24.3) 1 (8.3) 40 (23.3) Any prostatitis 38 (42.2) 28 (40.0) 1 (8.3) 67 (39.0) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Total 90 70 12 172
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ PSA: prostate-specific antigen, BPH: benign prostatic hyperplasia
Table 3. PSA levels for each grade of chronic inflammation ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Grade No. of patients PSA (ng/ml) p-value ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
I (mild) 15 10.06±5.08
II (moderate) 24 9.97±4.80 0.979
III (severe) 12 9.69±4.54
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ PSA: prostate-specific antigen
Table 4. Comparisons of the PSA levels according to the presence or absence of chronic inflammation at each location
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ No. of
PSA (ng/ml) p-value patients
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Periglandular inflammation
(+) 43 13.15±11.49
0.395
(-) 24 16.27±19.56
Stromal inflammation
(+) 40 15.10±17.33
0.546
(-) 27 12.94±9.85
Perivascular inflammation
(+) 36 15.61±17.89
0.404
(-) 31 12.69±10.17
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ PSA: prostate-specific antigen
PSA 증가에 대한 연구가 발표되었고, Neal 등12은 만성전립 선염에서도 혈청 PSA의 변화를 보고하였다. Nadler 등13은 전립선암이 발견되지 않는 환자에서 PSA가 4.0ng/ml 이상 인 군에서 조직학적으로 만성염증이 발견된 경우는 99%로 대조군인 PSA가 4.0ng/ml 이하인 군에서의 77%보다 유의 하게 높았다고 보고하여 만성 염증군에서도 PSA의 증가 가 능성을 보고하였으나 모두 전립선비대증을 가지고 있는 환 자를 대상으로 하였기 때문에 순수하게 만성염증에 의한 PSA 증가로 보기에는 어려운 점이 있었다. 그러나 Pansa- doro 등14은 전립선비대증과 전립선암 발생이 드문 50세 이 전의 전립선염 및 전립선통 환자를 대상으로 PSA가 4.0ng/
ml 이상인 환자가 급성전립선염에서 5/7례 (71%), 만성 세 균성 전립선염에서 2/13례 (15%), 만성비세균성전립선염에 서 2/32례 (6%)로 높게 나타나 PSA의 결과 해석에 만성전립 선염을 염두에 두어야 한다고 주장하였고, 국내에서 Cho 등15은 45세 이하 전립선염 환자 61명과 전립선염의 병력을 가진 전립선통 환자 18명, 총 79명에서 혈청 PSA의 평균은 1.99ng/ml, 2.05ng/ml이고 4.0ng/ml 이상인 경우는 11%였던 반면, 같은 연령층의 대조군 3,988명에서는 혈청 PSA의 평 균치가 0.97ng/ml이었으며 4.0ng/ml 이상인 경우가 0.88%에 불과해 만성전립선염 환자들에서 유의하게 혈청 PSA가 높 았다고 보고하였고, 또한 Cho 등16은 PSA가 증가된 장노년 의 환자에서 전립선염의 동반 가능성을 고려해야 한다고 하였다. Lee 등17은 전립선비대증 진단하에 전립선 수술을 받은 283례를 대상으로 병리조직학적 관찰을 통해 비특이 적 염증군이 274례 (96.8%)이며 이 중 259례는 경도 또는 중 증도, 15례 (5.4%)에서는 고도의 염증소견을 보였다고 하여 전립선비대증에 염증이 동반되어 있는 경우가 매우 흔함을 보고하였다. 본 연구에서도 PSA가 4.0ng/ml 이상인 172명 중에서 전립선암 (21.5%)과 전립선비대증만 있는 경우 (39.5%)도 많은 부분을 차지했지만 전립선염만 있는 경우 가 27명 (15.7%), 전립선염과 전립선비대증이 병발된 경우가 40명 (23.3%)으로 전립선염이 있는 총수는 67명 (39.0%)에 달해 PSA 상승의 많은 부분에서 전립선염이 관여되어 있음 을 확인할 수 있었다.
Pansadoro 등14은 급성 세균성 전립선염을 가진 7명의 환 자 중 5명 (71%)에서, 만성 세균성 전립선염을 가진 환자에 서는 13명 중 2명 (15%)에서 PSA가 증가되었다고 하였고, Yamamoto 등18은 급성 세균성 전립선염 환자 10명 중 6명 (60%)에서, 만성 전립선염 환자 10명 중 1명 (10%)에서 PSA 수치가 증가되었다고 하였다. 본 연구에서는 임상적인 급, 만성 구분이 아닌 조직학적인 급, 만성을 구분하였고 또한 이미 PSA 수치가 상승된 환자들에서 조직학적 병명을 구분 하였기에 급성과 만성의 어느 정도 비율에서 PSA 수치가
증가하는지는 확인하지 못하였다. 그러나 조직학적으로 급 성인 경우가 만성인 경우보다 PSA 수치가 더 높으므로 급 성인 경우에서 보다 많은 환자들이 PSA 증가를 보이리라고 추측할 수 있다. 또한 조직학적으로 급성인 경우는 만성인 경우보다 상대적으로 유병기간이 짧거나 최근 악화되는 양 상이었거나 하여 원래 갖고 있던 만성에 급성이 새로이 추 가되었거나 하는 상황일 수 있으므로 이러한 상황에서 PSA 상승을 보다 많이 보일 수 있고 상승된 PSA의 해석에도 이 를 고려해야 하겠다.
이러한 전립선염이 어떻게 PSA를 증가시키는가에 대하 여 Kohnen과 Drach19는 전립선상피의 파열과 PSA의 상승을 관찰하였고, Brawer 등2은 조직검사상 염증세포가 전립선 선조직과 전신 순환계 사이의 해부학적 장벽을 파괴하여 PSA가 상승한다는 누출현상을 처음 제시하였다. Hasui 등20 은 전립선염의 증상이 없었던 42명의 전립선비대증 환자들 을 대상으로 경요도 전립선 절제술을 시행한 검체에서 전 립선염의 정도와 PSA의 상관관계를 조사하였는데 선상피 세포를 면역화학적으로 염색했을 때 오히려 염증이 있는 선상피세포는 PSA 항원에 음성이었고, 염증이 없는 선상피 세포는 양성이었다. 이로써 전립선염이 PSA의 생산을 증가 시키는 것이 아니라 선상피세포에 저장되어 있는 PSA를 세 포고사로 인한 누출 (apoptosis leak)을 유발하고, 혈류증가 와 혈관투과성의 증가로 인한 간질조직 내의 혈류로 나오 게 한다는 누출현상을 뒷받침하였고, Kessaris 등21에 의해 서도 유사한 실험으로 재확인되었다.
따라서 전립선염은 PSA를 증가시키는데 염증을 보다 세 분하여 PSA 변화를 관찰하고자 하는 시도가 있어 왔다.
Irani 등3은 혈중 PSA의 증가를 보여 전립선생검을 시행한 66명을 대상으로 조직학적으로 염증의 정도를 four-point scale에 따라 분류하여 각 grade별 PSA 수치를 비교한 결과 염증의 정도와는 연관성이 없었고, 염증의 침윤도 (inva- siveness)가 증가함에 따라 혈중 PSA치가 증가됨을 발표하 였다. 이후 Schatteman 등22도 Irani 등3과 동일한 결과를 발 표하여 PSA는 염증의 정도보다는 침윤도에 연관이 있다고 주장하였다. 본 연구에서도 염증의 정도에 따른 PSA 차이 는 없었다. 염증의 침윤도에 따른 PSA 변화는 본 연구에서 조사하지 않아서 염증의 침윤도와 PSA의 상관관계는 확인 할 수 없었다. 그러나 본 연구에서 시행한 각 부위별 염증의 유무에 따른 혈중 PSA의 비교에서 세 부위 모두 염증의 유 무에 따른 PSA 수치의 차이가 없었는데, 특히 염증의 침윤 도와 관계있는 periglandular에서도 염증의 유무에 따른 PSA 차이가 없었으므로 염증의 침윤도가 PSA와 연관이 있다는 기존의 보고3,22와 상충되는 부분이 있으므로 추가적인 연구 가 필요하다고 생각한다.
한편 전립선암이나 전립선비대증에서 염증이 동반되는 빈도가 높아 특히 전립선의 만성 염증이 전립선암을 유발 하는 관여할 수 있다는 주장이 있다.23 그러나 이를 증명하 기 위해서는 추가적인 연구가 필요한 실정이다.
결 론
혈청 PSA가 4ng/ml 이상으로 전립선생검을 시행받은 172 명의 환자 중 전립선염은 39% (67명)에서 발견되었다. 이들 무증상 전립선염 환자들에서 PSA치는 조직학적으로 급성 염증인 경우가 만성염증인 경우보다 더 높았지만, 염증의 정도에 따른 PSA치의 차이는 없었고 각 부위별 염증의 유 무에 따른 PSA 차이도 없었다. 이상에서 PSA가 증가된 장 노년 환자들에서 무증상 전립선염에 대한 고려가 필요하다 고 생각한다.
REFERENCES
1. Stamey TA, Kabalin JN. Prostate specific antigen in the di- agnosis and treatment of adenocarcinoma of the prostate. I.
Untreated patients. J Urol 1989;141:1070-5
2. Brawer MK, Rennels MA, Nagle RB, Schifman R, Gaines JA.
Serum prostate-specific antigen and prostate pathology in men having simple prostatectomy. Am J Clin Pathol 1989;92:760-4 3. Irani J, Levillain P, Goujon JM, Bon D, Dore B, Aubert J.
Inflammation in benign prostatic hyperplasia: correlation with prostate specific antigen value. J Urol 1997;157:1301-3 4. Hara M, Koyanagi Y, Inoue T, Fukuyama T. Some physico-
chemical characteristics of “gamma-seminoprotein”, an anti- genic component specific for human seminal plasma. Nippon Hoigaku Zasshi 1971;25:322-4
5. Wang MC, Valenzuela LA, Murphy GP, Chu TM. Purification of human prostate specific antigen. Invest Urol 1979;17:159-63 6. Papsidero LD, Wang MC, Valenzuela LA, Murphy GP, Chu
TM. A prostate antigen in sera of prostatic cancer patients.
Cancer Res 1980;40:2428-32
7. Lilja H. Structure, function, and regulation of the enzyme activity of prostate-specific antigen. World J Urol 1993;11:
188-91
8. Diamandis EP, Yu H. Nonprostatic sources of prostate-specific antigen. Urol Clin North Am 1997;24:275-82
9. Oesterling JE. Prostate specific antigen: a critical assessment
of the most useful tumor marker for adenocarcinoma of the prostate. J Urol 1991;145:907-23
10. Stamey TA, Yang N, Hay AR, McNeal JE, Freiha FS, Red- wine E. Prostate-specific antigen as a serum marker for adeno- carcinoma of the prostate. N Engl J Med 1987;317:909-16 11. Dalton DL. Elevated serum prostate-specific antigen due to
acute bacterial prostatitis. Urology 1989;33:465
12. Neal DE Jr, Clejan S, Serma D, Moon TD. Prostate-specific antigen and prostatitis I, Effect of prostatitis on serum PSA in the human and nonhuman primate. Prostate 1992;20:105-11 13. Nadler RB, Hymphrey PA, Smith DS, Catalona WJ, Ratiff TL.
Effect of inflammation and benign prostatic hyperplasia on elevated serum prostate specific antigen levels. J Urol 1995;
154:407-13
14. Pansadoro V, Emiliozzi P, Defidio L, Scarpone P, Sabatini G, Brisciani A, et al. Prostate-specific antigen and prostatitis in men under fifty. Eur Urol 1996;30:24-7
15. Cho IR, Kim GJ, Park SS, Choi HS. PSA and prostatitis in men under 45 years old. Korean J Urol 1998;39:633-7 16. Cho IR, Chang YS, Roh JS, Jeon JS, Park SS. Change of PSA
and PSAD after antibiotic treatment in patients with prostatitis.
Korean J Androl 2002;20:100-5
17. Lee SY, Park YY. Clinical characteristics of the associated histopathological findings in benign prostatic hyperplasia.
Korean J Urol 1991;32:915-20
18. Yamamoto M, Hibi H, Miyake K. Prostate-specific antigen levels in acute and chronic bacterial prostatitis. Hinyokika Kiyo 1993;39:445-9
19. Kohnen PW, Drach GW. Patterns of inflammation in benign prostatic hyperplasia: a histologic and bacteriologic study. J Urol 1979;121:755-60
20. Hasui Y, Marutsuka K, Asada Y, Ide H, Nishi S, Osada Y.
Relationship between serum prostate specific antigen and his- tological prostatitis in patients with benign prostatic hyper- plasia. Prostate 1994;25:91-6
21. Kessaris DN, Lee CK, Valderamma E, Moldwin RM. Prostatic specific antigen immunohistochemistry in patients with pro- statitis. J Urol 1994;151(Suppl):404, abstract 707
22. Schatteman PH, Hoekx L, Wyndaele JJ, Jeuris W, Van Marck E. Inflammation in prostate biopsies of men without prostatic malignancy or clinical prostatitis: correlation with total serum PSA and PSA density. Eur Urol 2000;37:404-12
23. Platz EA, De Marzo AM. Epidemiology of inflammation and prostate cancer. J Urol 2004;171(Suppl):36-40