http://dx.doi.org/10.3341/jkos.2015.56.6.803
Original Article
가쪽눈꺼풀판띠고정술의 임상적 효과
Clinical Effectiveness of the Lateral Tarsal Strip Procedure
나건후⋅이준식⋅이 화⋅백세현
Kun Hoo Na, MD, Joon Sik Lee, MD, Hwa Lee, MD, PhD, Se Hyun Baek, MD, PhD
고려대학교 의과대학 안과학교실
Department of Ophthalmology, Korea University College of Medicine, Seoul, Korea
Purpose: To evaluate the clinical indications and efficacy of the lateral tarsal strip procedure.
Methods: The medical records of patients who underwent the lateral tarsal strip procedure between September 2008 and February 2014 were retrospectively reviewed. We examined age, gender, diagnosis, procedures simultaneously performed with the lateral tarsal strip, duration of observation, postoperative complications and cases requiring revision surgery. Patients with- out recurrence or undercorrection of eyelid/lateral canthal area lesions, surgical complication and not requiring revision surgery until final visit were considered as successful cases.
Results: One hundred eighty-three eyes of 129 patients were included in this study. The mean patient age was 61.6 years and average follow-up duration was 9.2 months. Diagnoses of eyes were lower lid laxity (39.9%), involutional entropion (24.0%), low- er lid retraction (14.8%), cicatricial ectropion (6.6%), lateral canthal deformity (5.5%), involutional ectropion (3.8%) and paralytic ectropion (2.7%). Surgical procedures simultaneously conducted with lateral tarsal strip in 167 eyes of 183 eyes were endo- scopic dacryocystorhinostomy (30.5%), lower retractor tightening (19.2%), medial spindle procedure (13.8%), mid-lamellar lengthening (12.6%), lower blepharoplasty (10.8%), Quickert suture (4.2%) and Hotz’s operation (3.0%). Successful results were obtained in 116 of 129 patients (89.9%).
Conclusions: The lateral tarsal strip procedure can successfully correct lower lid laxity and be used in various clinical indications with or without other surgical procedures.
J Korean Ophthalmol Soc 2015;56(6):803-810 Key Words: Lateral tarsal strip, Lid laxity
■Received: 2014. 9. 12. ■ Revised: 2015. 1. 8.
■Accepted: 2015. 5. 12.
■Address reprint requests to Se Hyun Baek, MD, PhD
Department of Ophthalmology, Korea University Guro Hospital,
#148 Gurodong-ro, Guro-gu, Seoul 152-703, Korea Tel: 82-2-2626-1260, Fax: 82-2-857-8580 E-mail: [email protected]
* This study was supported in part by Alumni of Department of Ophthalmology, Korea University College of Medicine in 2014.
ⓒ2015 The Korean Ophthalmological Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
가쪽눈꺼풀판띠고정술은 Anderson에 의해 1970년대 소 개되어 현재까지 가장 널리 이용되는 눈구석성형술의 하나 로 가쪽눈구석인대를 단축시켜 눈꺼풀의 수평 강화를 통해
눈꺼풀의 수평이완이나 눈꺼풀겉말림을 교정하기 위해 시 행된다.1-3
수술 시간이 짧고 방법이 비교적 간단하여 단독으로 혹 은 다른 수술과 함께 다양한 질환에서 행해지고 있다. 아래 눈꺼풀 이완이 동반된 코눈물관폐쇄 환자에서 내시경적 눈 물주머니코안연결술과 가쪽눈꺼풀판띠고정술을 함께 시행 하였을 때 눈물펌프 기능이 호전될 수 있으며, 안쪽눈구석 의 이완이 없는 퇴행성 눈꺼풀겉말림 환자에서 단독으로 시행 시에도 훌륭한 교정효과가 보고된 바 있다.4-6 또한 무 안구 안와에서 의안의 무게로 발생하는 아래눈꺼풀의 수평 이완과 이와 동반되는 결막낭의 수축에 대한 치료에도 이 용될 수 있다.1
A B
C D
E F
G H
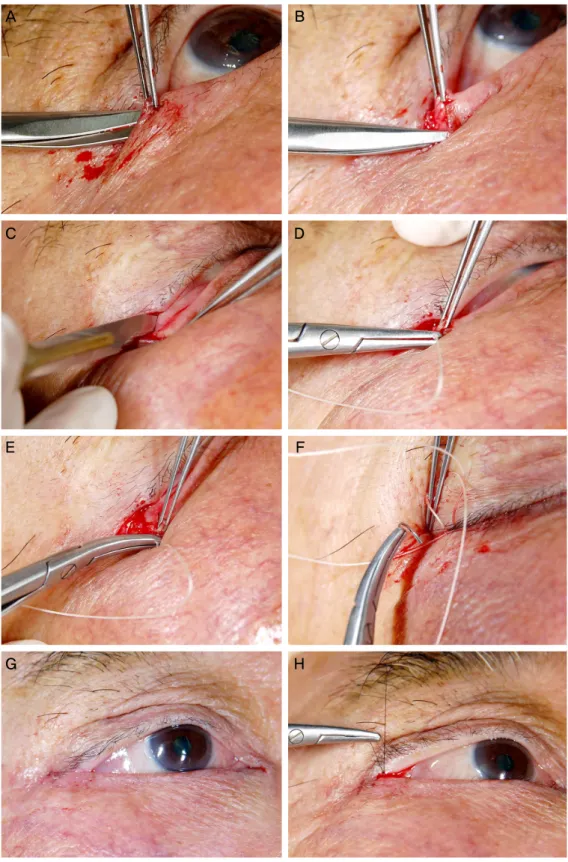
Figure 1. The lateral tarsal strip procedure. (A) After lateral canthotomy, the inferior crus of the lateral can-
thal tendon was released. (B) The tarsal strip was designed by separating the anterior lamella from the tarsus.(C) The palpebral conjunctiva overlying the tarsal strip was gently peeled with a No.15 blade. (D) The su- perolateral aspect of the tarsal strip was fully passed by vicryl suture on a P-2 semicircular needle. (E, F) The needle was rotated through the periosteum at the lateral orbital rim just above to the insertion of lateral canthal tendon and passed from posterolateral portion of the upper eyelid. (G) The tarsal strip was engaged with the suture and secured to the lateral orbital rim. (H) The skin was approximated with interrupted 7-0 silk sutures.
Table 1. Demographics of the patients undergoing lateral tar-
sal strip procedurePatients (eyelids) 129 (183)
Male gender (n, %) 59 (44.7)
Bilateral cases (n, %) 54 (41.9)
Age (years) 61.6 ± 17.2 (7-90)
Follow-up duration (months) 9.2 ± 12.9 Values are presented as mean ± SD unless otherwise indicated.
Figure 2. (A) A 67-year-old woman presents with involutional
entropion and laxity of the right lower eyelid. (B) After tight- ening of inferior retractor and lateral tarsal strip procedure, she demonstrates normal eyelid contour.국내에서도 Ahn and Chung7이 9명 11안에 대해 가쪽눈 꺼풀판띠고정술의 임상경험을 보고한 바 있으며 특정 눈꺼 풀질환 및 눈물길질환에 대한 치료방법으로서 가쪽눈꺼풀 판띠고정술의 효과를 보고한 문헌들이 있었다.8-12 하지만 아직까지 국내에서 많은 예로 보고된 적이 없기에, 본 저자 들은 가쪽눈꺼풀판띠고정술을 받았던 환자들의 의무기록 을 후향적으로 조사하여 각각의 임상적 적응증과 그 효과 에 대해 알아보고자 하였다.
대상과 방법
2008년 9월부터 2014년 2월까지 본원 안과에서 가쪽눈 꺼풀판띠고정술을 시행 받았던 환자 129명 183안을 대상으 로 의무기록을 후향적으로 조사하였다.
모든 환자의 수술은 동일한 술자에 의해 이루어졌다.
1:100,000 epinephrine이 혼합된 2% lidocaine을 가쪽눈구 석, 아래눈꺼풀, 가쪽안와 가장자리에 깊숙이 주사한 후 가 쪽눈구석절개술을 시행하였다. 이후 가쪽눈구석인대의 아 래갈래를 절단하여 아래눈꺼풀이 가쪽안와 가장자리로부 터 떨어지도록 하였다. 눈꺼풀의 앞층판과 뒤층판을 분리 하여 눈꺼풀판띠를 만든 후 눈꺼풀테를 제거하고 눈꺼풀판 띠 안쪽의 결막상피를 칼로 긁어내었다. 분리된 눈꺼풀판 띠를 붙잡을 때 가쪽아래눈꺼풀이 자유롭게 움직임을 확인 한 뒤 4-0 vicryl로 눈꺼풀판띠를 골막에 고정시켰다. 봉합 시 바늘로 눈꺼풀판띠의 상외측면을 전층으로 통과시키고 가쪽눈구석인대의 부착부위 바로 위쪽의 가쪽안와 가장자 리의 안쪽면에서 골막을 통과시켰다. 이후 봉합사가 가쪽 윗눈꺼풀의 후면을 지나게 한 뒤 봉합하였다. 피부와 가쪽 눈구석을 7-0 black silk로 봉합하였다(Fig. 1).
환자의 나이, 성별, 수술 시의 진단, 함께 시행된 수술, 술 후 경과관찰 기간, 합병증, 재수술 여부, 수술의 결과를 분 석하였다. 마지막 방문 시점까지 재수술 없이 눈꺼풀 또는 눈구석인대병변의 재발, 부족교정이 나타나지 않고 가쪽눈 꺼풀판띠고정술로 인한 술 후 합병증이 발생하지 않은 경 우를 성공의 기준으로 하였다.
결 과
총 129명(183안)이 연구에 포함되었고, 평균 나이는 61.6 세(7-90세), 성별 분포는 남성 59명, 여성 70명이었다. 양측 아래눈꺼풀에 수술을 시행한 경우는 54명(41.9%)이었으며 수술 후 평균 9.2개월 추적관찰을 시행하였다(Table 1). 가 쪽눈꺼풀판띠고정술이 시행된 183안의 임상적 진단은 눈꺼 풀수평이완(39.9%)이 가장 많았고, 퇴행성 눈꺼풀속말림
(24.0%) (Fig. 2), 아래눈꺼풀뒤당김(14.8%) (Fig. 3), 반흔성 눈꺼풀겉말림(6.6%), 가쪽눈구석인대변형(5.5%), 퇴행성 눈꺼풀겉말림(3.8%), 마비성 눈꺼풀겉말림(2.7%) (Fig. 4) 순이었다(Table 2).
가쪽눈꺼풀판띠고정술과 함께 다른 수술을 같이 시행 받은 환자는 183안 중 167안(91.3%)이었다. 이 중 내시경적 눈물 주머니코안연결술(30.5%)을 가장 많이 시행하였고, 아래눈꺼 풀당김기재부착술(19.2%), 안쪽방추형결막절제술(13.8%), 중 간층판연장술(12.6%), 아래눈꺼풀 성형술(10.8%), Quickert 봉합술(4.2%), 호쯔씨수술(3.0%)순이었다(Table 3).
총 129명 중 116명(89.9%)에서 성공적인 수술 결과를 보 였으며, 13명의 환자들에 대해서는 만족스럽지 못한 결과
A
B
Figure 3. (A) A 43-year-old woman with thyroid eye disease
demonstrates lower eyelid retraction of both eyes. (B) Eyelid position has been corrected with mid-lamellar lengthening and lateral tarsal strip procedure.Table 2. Clinical indications of the lateral tarsal strip procedure
Diagnosis Eyelids (%)
Lower lid laxity 73 (39.9)
Involutional entropion 44 (24.0)
Lower lid retraction 27 (14.8)
Cicatricial ectropion 12 (6.6)
Lateral canthal deformity 10 (5.5)
Involutional ectropion 7 (3.8)
Paralytic ectropion 5 (2.7)
Others* 5 (2.7)
Total 183
*Others include skin defect of lower eyelid secondary to tumor ex- cision, ectropion resulting from traumatic lower eyelid laceration, cicatricial entropion.
Figure 4. (A) A 69-year-old woman presents with paralytic ec-
tropion of the left eye. (B) Left lower eyelid has been in nor- mal position after lateral tarsal strip.Table 3. Surgical procedures simultaneously performed with
the lateral tarsal strip procedureEyelids (%)
Endoscopic DCR 51 (30.5)
Inferior retractor tightening 32 (19.2)
Medial spindle procedure 23 (13.8)
Mid-lamellar lengthening 21 (12.6)
Lower blepharoplasty 18 (10.8)
Quickert suture 7 (4.2)
Hotz’s operation 5 (3.0)
Others* 10 (6.0)
Total 167
DCR = dacryocystorhinostomy.
*Others include external DCR, bicanalicular tube intubation, skin graft after tumor excision, fornix reconstruction using acellular dermis matrix allograft, lateral tarsorrhapy, root-z epicanthoplasty.
를 얻었다(Table 4). 이 13명의 환자들 중 병변이 재발한 경 우가 6명(46.2%), 부족교정 3명(23.1%), 상처 벌어짐 2명 (15.4%), 가쪽 눈구석변형이 발생한 경우가 2명(15.4%) (Fig. 5)이었다. 상처 벌어짐이 발생한 2명에 대해서는 재봉 합술을 시행하였고, 가쪽눈구석변형이 발생한 2명, 병변이 재발한 환자 중 4명, 부족교정된 환자 중 한 명에게 가쪽눈 꺼풀판띠고정술을 다시 시행하였다.
고 찰
본 연구를 통해 가쪽눈꺼풀판띠고정술은 단독으로 또는 다른 수술과 함께 시행되어 코눈물관폐쇄, 퇴행성 눈꺼풀 속말림, 아래눈꺼풀뒤당김, 눈꺼풀겉말림 등의 다양한 적응 증에 이용될 수 있음을 알 수 있었다.
아래눈꺼풀은 눈물샘으로부터 눈물점에 이르는 눈물층
A A
B B
Table 4. Characteristics of patients with poor surgical outcomes after the lateral tarsal strip procedure
Case Age/sex Diagnosis Previous surgery Treatment Outcome
1 72, M Paralytic ectropion None Lateral tarsal strip Wound dehiscence
2 49, M Lower lid retraction Lower blepharoplasty Lateral tarsal strip Mid-lamellar lenghthening Lower blepharoplasty
Recurrent lower lid retraction
3 64, M Lower lid laxity None Lateral tarsal strip
Lower blepharoplasty
Recurrent lower lid laxity 4 39, M Lower lid retraction Reconstruction of
orbital wall fracture
Lateral tarsal strip Mid-lamellar lenghthening
Recurrent lower lid retraction 5 46, F Lower lid laxity in
anophthalmic socket
Evisceration Lateral tarsal strip Fornix reconstruction
Recurrence of lower lid laxity and fornix contraction
6 69, M Cicatricial ectropion Lower blepharoplasty Lateral tarsal strip Recurrent ectropion 7 64, F Lateral canthal deformity Lateral canthal surgery Lateral tarsal strip Undercorrection 8 61, M Cicatricial ectropion Four lid blepharoplasty Lateral tarsal strip
Medial spindle procedure
Recurrent ectropion
9 66, F Lower lid laxity None Lateral tarsal strip Lateral canthal deformity (webbing)
10 68, M Involutional entropion None Lateral tarsal strip
Inferior retractor tightening
Wound dehiscence
11 59, F Lower lid retraction None Lateral tarsal strip
Mid-lamellar lenghthening
Lateral canthal deformity (rounding)
12 75, F Paralytic ectropion None Lateral tarsal strip
Medial spindle procedure
Undercorrection
13 61, M Cicatricial entropion None Lateral tarsal strip
Hotz’s operation
Undercorrection
의 순환작용에 있어 중요한 역할을 한다.13 아래눈꺼풀의 일차적인 지지구조는 눈꺼풀판인대 복합체이고 이차적인 지지구조에는 아래눈꺼풀의 전후 균형을 유지시키는 아래 눈꺼풀 당김근육, 눈꺼풀과 안와 내용물을 감싸주는 눈둘 레근, 그리고 눈꺼풀이 뒤로 기울어지지 않게 하는 안구 그 자체가 포함된다.14 가쪽눈구석인대와 안쪽눈구석인대가 퇴 행성으로 약화되거나 지방이 침윤되면 아래눈꺼풀의 위치 이상과 수평이완이 발생하게 되며, 아래눈꺼풀과 주변구조 물이 외상, 종양, 염증 등의 이유로 손상이 되어 기능을 하 지 못할 때에도 아래눈꺼풀이 정상적인 위치에서 벗어나게
된다.15-17 이렇게 유발된 아래눈꺼풀의 위치 이상으로 눈물
흘림, 이물감, 광시증 등의 증상이 나타나게 된다.18,19 가쪽눈구석인대는 눈꺼풀의 위치와 탄력성을 결정하는 중요한 구조물로 아래눈꺼풀의 퇴행성 수평이완은 눈꺼풀 판의 이완이나 안쪽눈구석의 약화보다는 가쪽눈구석인대 의 약화로 나타나는 경우가 많다. 여러 저자들은 눈꺼풀 수 평이완의 치료에 있어 가쪽눈구석의 수술적 교정을 통한 아래 눈꺼풀의 해부학적인 복구가 중요함을 강조하였으며, 눈꺼풀의 위치 이상을 교정함과 동시에 눈꺼풀 단축을 통 한 눈물펌프의 호전을 도모할 수 있다고 하였다.2,3,20-26 가쪽 눈구석인대를 단축시키는 방법으로 눈꺼풀의 수평 강화가 이루어지면 눈둘레근의 감소된 긴장도를 보상하여 눈을 감 을 때 더 효과적으로 눈물이 눈물점 안으로 진입할 수 있게 되어 눈물펌프의 기능이 호전되고 눈물주머니를 잡아 당기
는 힘이 증가하여 발생하는 압력 차가 형성되어 눈물이 눈 물주머니 안으로 들어가는 데 도움을 준다.27 또한 가쪽눈 구석인대의 위치를 올려줌으로써 중력에 의한 눈물 배출도 원활해질 것이다. 가쪽눈구석의 각도가 뚜렷해져 특히 동 양인에서의 미용적인 효과도 기대할 수 있겠다. 본 연구자들 은 가쪽눈꺼풀판띠고정술을 시행함으로써 눈꺼풀의 수평이 완을 성공적으로 교정하였으며, 단독으로 또는 다른 수술과 병합하여 다양한 눈꺼풀 및 눈구석질환에 적용시켰다.
코눈물관폐쇄 환자에서 눈물주머니코안연결술이 성공적 으로 시행되었음에도 눈물흘림이 지속될 때에는 눈물펌프 의 기능이 원활하지 않음을 고려해야 하며 아래 눈꺼풀의 수평강화술을 시행함으로써 눈물펌프의 기능 회복이 이루 어질 수 있다.28,29 따라서 코눈물관폐쇄 환자에서 눈물점겉 말림의 평가와 함께 눈꺼풀수평이완을 확인하는 것은 매우 중요하며, 필요시 가쪽눈꺼풀판띠고정술을 함께 시행한다 면 눈물흘림에 대한 더욱 효과적인 치료가 이루어질 것이 다.4,5 본 연구에서 가쪽눈꺼풀판띠고정술과 함께 시행하였 던 수술들 중 내시경적 눈물주머니코안연결술이 가장 많았 으며, 수술 전 눈꺼풀당겼다놓기검사(snap back test) 및 눈 꺼풀잡아당기기검사(distraction test)를 통해 눈꺼풀수평이 완이 있음을 확인하였다.
퇴행성 눈꺼풀속말림을 일으키는 주요 기전으로 눈꺼풀 의 수평이완, 아래눈꺼풀당김기의 약화 또는 부착부파열, 안와사이막앞 눈둘레근의 연축과 상방이동이 제시되고 있
Figure 5. Postoperative complications after lateral tarsal strip
procedure. (A) Rounding deformity of the lateral canthus of the right eye. (B) W ebbing of the lateral canthal area of the left eye.다.30-34 이러한 해부학적 요인들 중에서 아래눈꺼풀당김기
의 약화 혹은 부착부 파열이 퇴행성 눈꺼풀속말림의 일차 적인 원인으로 생각되고 있으나 눈꺼풀의 수평이완 또한 중요한 요인으로 작용하며 여러 해부학적 원인들에 대한 복합적 교정을 통해 안검내반증을 더욱 효과적으로 치료할 수 있다.35-37 또한 퇴행성 눈꺼풀속말림의 교정을 위하여 가 장 많이 이용되는 아래눈꺼풀당김기재부착술을 시행 시 눈 꺼풀의 수평이완이 있으면 과교정되어 눈꺼풀겉말림이 발 생할 수 있으므로 눈꺼풀속말림에 대한 수술을 계획하기 전 눈꺼풀의 수평이완에 대한 평가가 반드시 이루어져야 하며 이에 대한 치료가 함께 시행되어야 한다.
아래눈꺼풀뒤당김은 아래눈꺼풀성형술, 안와골절 정복 술, 의안 수술 후 이차적으로 발생할 수 있으며, 갑상샘눈
병증 환자에서도 나타날 수 있다. 아래눈꺼풀뒤당김을 일 으키는 해부학적인 원인으로 근막초와 안와사이격막 혹은 아래눈꺼풀당김기 사이의 반흔 형성, 안면 중앙부 하강, 그 리고 가쪽눈꺼풀띠이완이 있다.38 눈꺼풀의 수평이완이 동 반되었을 때에는 중력에 의한 영향이 크게 작용하여 아래 눈꺼풀의 경계가 더욱 아래로 후퇴하게 된다. 이때 아래눈 꺼풀은 윗눈꺼풀과 달리 운동성이 적기 때문에 안구의 하 방돌출 발생 시 눈꺼풀뒤당김이 더욱 악화될 수 있다.39 그 러므로 아래눈꺼풀뒤당김 환자에서 아래눈꺼풀의 이완정 도를 평가하여 이에 따라 수술 원칙을 세워야 한다.
눈꺼풀겉말림 중 가장 흔한 형태는 퇴행성 눈꺼풀겉말림 으로 눈꺼풀판-인대걸이의 느슨함, 엘라스틴의 전반적인 감소에 따른 눈꺼풀의 수평이완으로 발생한다.40 얼굴신경 마비로 눈둘레근이 아래눈꺼풀을 지지하지 못하게 되면 눈 꺼풀의 이완으로 눈꺼풀겉말림이 발생하며 반흔성 눈꺼풀 겉말림환자에서도 앞층판의 단축과 함께 눈꺼풀의 수평이 완을 종종 확인할 수 있다. 따라서 눈꺼풀겉말림에 대한 수 술 전 눈꺼풀의 이완에 대한 평가가 필요하다.
가쪽눈꺼풀판띠고정술 시행 후 발생할 수 있는 합병증으 로 눈꺼풀의 수평단축, 상처 벌어짐 등이 발생할 수 있으며, 상처 치유에 상대적으로 오랜 시간이 걸린다는 단점이 보 고된 바 있다.24,41,42 본 연구에서는 13명의 환자들에게 병변 의 재발, 부족교정, 상처 벌어짐, 가쪽눈구석변형 등의 이유 로 만족스럽지 못한 결과가 초래되었고, 이들 중 9명의 환 자들에게 재수술을 시행하였다.
본 연구는 후향적으로 진행되었고, 술 후 평균 추적관찰 기간이 길지 않았으며, 술 후 눈꺼풀의 위치에 대한 객관적 인 평가가 없었다는 한계점이 있다. 추후 가쪽눈꺼풀판띠 고정술의 효과를 객관적으로 평가할 수 있는 지표를 개발 하여 장기간의 추적관찰을 통한 연구가 필요할 것으로 사 료된다.
가쪽눈꺼풀판띠고정술은 눈꺼풀의 수평이완을 성공적으 로 교정할 수 있으며, 단독으로 혹은 다른 수술과 함께 다 양한 적응증에 이용될 수 있다. 코눈물관폐쇄, 퇴행성 눈꺼 풀속말림, 아래눈꺼풀뒤당김, 눈꺼풀겉말림 등의 질환에서 눈꺼풀의 수평이완을 평가하는 것은 매우 중요하며, 이에 대해 가쪽눈꺼풀판띠고정술을 시행함으로써 성공적인 수 술 결과를 얻을 수 있었다. 그러므로 본 연구는 가쪽눈꺼풀 판띠고정술의 임상적 유용성을 판단하는 데 있어 유용한 자료가 될 것이라고 생각한다.
REFERENCES
1) Anderson RL. Tarsal strip procedure for correction of eyelid laxity and canthal malposition in the anophthalmic socket. Ophthalmology
A
B
1981;88:895-903.
2) Anderson RL, Gordy DD. The tarsal strip procedure. Arch Ophthalmol 1979;97:2192-6.
3) Jordan DR, Anderson RL. The lateral tarsal strip revisited. The en- hanced tarsal strip. Arch Ophthalmol 1989;107:604-6.
4) Lee H, Hwang JY, Kim JW, et al. The effectiveness of simultaneous lateral tarsal strip with endonasal dacryocystorhinostomy for the treatment of nasolacrimal duct obstruction and lower lid laxity. J Craniofac Surg 2013;24:980-3.
5) Lee H, Lee JS, Chang M, et al. The effectiveness of simultaneous medial spindle and/or lateral tarsal strip procedure in East Asian patients who need endonasal dacryocystorhinostomy. Graefes Arch Clin Exp Ophthalmol 2013;251:2789-96.
6) Kam KY, Cole CJ, Bunce C, et al. The lateral tarsal strip in ec- tropion surgery: is it effective when performed in isolation? Eye (Lond) 2012;26:827-32.
7) Ahn TK, Chung WS. Clinical experience of tarsal strip procedure.
J Korean Ophthalmol Soc 1990;31:1489-94.
8) Kim SW, Lee WS, Rho JH. Lateral tarsal strip procedure combined with quickert sutures in correcting involutional entropion. J Korean Ophthalmol Soc 2012;53:1213-8.
9) Kim KH, Chung IY, Seo SW. The effect of augmented lateral tarsal strip for paralytic ectropion in leprosy patients. J Korean Ophthalmol Soc 2009;50:497-504.
10) Woo JM, Shin DM, Park JM, Ahn HB. The effects of lateral tarsal strip procedure on the functional nasolacrimal duct obstruction. J Korean Ophthalmol Soc 2006;47:1375-80.
11) Ko SJ, Kim SD. Involutional ectropion repair with the modified medial spindle and the lateral tarsal strip procedure. J Korean Ophthalmol Soc 2012;53:187-92.
12) Ryu WY, Suh JY, Ahn HB. Lateral tarsal strip procedure and sili- cone tube intubation on the functional nasolacrimal duct obstruction. J Korean Ophthalmol Soc 2010;51:1174-8.
13) Bergeron CM, Moe KS. The evaluation and treatment of lower eyelid paralysis. Facial Plast Surg 2008;24:231-41.
14) Moe KS, Kao CH. Precaruncular medial canthopexy. Arch Facial Plast Surg 2005;7:244-50.
15) Ousterhout DK, Weil RB. The role of the lateral canthal tendon in lower eyelid laxity. Plast Reconstr Surg 1982;69:620-3.
16) Anderson RL, Hatt MU, Dixon R. Medial ectropion. A new technique. Arch Ophthalmol 1979;97:521-4.
17) Stefanyszyn MA, Hidayat AA, Flanagan JC. The histopathology of involutional ectropion. Ophthalmology 1985;92:120-7.
18) Hill JC. Treatment of epiphora owing to flaccid eyelids. Arch Ophthalmol 1979;97:323-4.
19) Liu D, Stasior OG. Lower eyelid laxity and ocular symptoms. Am J Ophthalmol 1983;95:545-51.
20) Corin S, Veloudios A, Harvey JT. A modification of the lateral tar- sal strip procedure with resection of orbicularis muscle for en- tropion repair. Ophthalmic Surg 1991;22:606-8.
21) Tenzel RR, Buffam FV, Miller GR. The use of "lateral canthal
sling" in ectropion repair. Can J Ophthalmol 1977;12:199-202.
22) Liu D. Lower eyelid tightening: a comparative study. Ophthal Plast Reconstr Surg 1997;13:199-203.
23) Olver JM. Surgical tips on the lateral tarsal strip. Eye (Lond) 1998;12(Pt 6):1007-12.
24) Glat PM, Jelks GW, Jelks EB, et al. Evolution of the lateral cantho- plasty: techniques and indications. Plast Reconstr Surg 1997;100:
1396-405; discussion 1406-8.
25) Naugle TC. Lateral canthoplasty. J Dermatol Surg Oncol 1992;
18:1075-80.
26) Weber PJ, Popp JC, Wulc AE. Refinements of the tarsal strip procedure. Ophthalmic Surg 1991;22:687-91.
27) Becker BB. Tricompartment model of the lacrimal pump mechanism.
Ophthalmology 1992;99:1139-45.
28) Detorakis ET, Drakonaki E, Papadaki E, et al. Watery eye follow- ing patent external DCR: an MR dacryocystography study. Orbit 2010;29:239-43.
29) Hurwitz JJ. Investigation and treatment of epiphora due to lid laxity. Trans Ophthalmol Soc U K 1978;98:69-70.
30) Benger RS, Musch DC. A comparative study of eyelid parameters in involutional entropion. Ophthal Plast Reconstr Surg 1989;5:281-7.
31) Haefliger IO, Piffaretti JM. Lid retractors desinsertion in acquired ptosis and involutional lower lid entropion: surgical implications.
Klin Monbl Augenheilkd 2001;218:309-12.
32) Jones LT, Reeh MJ, Tsujimura JK. Senile entropion. Am J Ophthalmol 1963;55:463-9.
33) Collin JR, Rathbun JE. Involutional entropion. A review with eval- uation of a procedure. Arch Ophthalmol 1978;96:1058-64.
34) Park MS, Chi MJ, Baek SH. Clinical study of single-suture inferior retractor repair for involutional entropion. Ophthalmologica 2006;220:327-31.
35) Ho SF, Pherwani A, Elsherbiny SM, Reuser T. Lateral tarsal strip and quickert sutures for lower eyelid entropion. Ophthal Plast Reconstr Surg 2005;21:345-8.
36) Quist LH. Tarsal strip combined with modified Quickert-Rathbun sutures for involutional entropion. Can J Ophthalmol 2002;37:238-44.
37) Rougraff PM, Tse DT, Johnson TE, Feuer W. Involutional en- tropion repair with fornix sutures and lateral tarsal strip procedure.
Ophthal Plast Reconstr Surg 2001;17:281-7.
38) Patipa M. The evaluation and management of lower eyelid re- traction following cosmetic surgery. Plast Reconstr Surg 2000;106:
438-53; discussion 454-9.
39) Chang EL, Rubin PA. Upper and lower eyelid retraction. Int Ophthalmol Clin 2002;42:45-59.
40) McCord CD Jr, Codner MA. Eyelid and periorbital surgery, 1st ed.
St. Louis: CRC Press, 2008;636-42.
41) Oestreicher JH, Tarassoly K. The "mini tarsal strip" lateral cantho- pexy for lower eyelid laser-assisted blepharoplasty-indications, technique and complications in 614 cases. Orbit 2010;29:7-10.
42) Vagefi MR, Anderson RL. The lateral tarsal strip mini-tarsor- rhaphy procedure. Arch Facial Plast Surg 2009;11:136-9.
= 국문초록 =
가쪽눈꺼풀판띠고정술의 임상적 효과
목적: 가쪽눈꺼풀판띠고정술의 임상적 적응증과 그 효과에 대해 알아보고자 하였다.
대상과 방법: 2008년 9월부터 2014년 2월까지 가쪽눈꺼풀판띠고정술을 시행 받았던 환자들의 의무기록을 후향적으로 조사하여 환자 의 나이, 성별, 수술 시의 진단, 함께 시행된 수술, 술 후 추적관찰 기간, 합병증, 재수술 여부를 분석하였다. 마지막 방문 시점까지 재수술 없이 병변의 재발, 부족교정이 나타나지 않고 수술의 합병증이 발생하지 않은 경우를 성공의 기준으로 하였다.
결과: 총 129명(183안)이 연구에 포함되었고 평균연령은 61.6세, 술 후 추적관찰 기간은 평균 9.2개월이었다. 수술 시의 진단은 아래눈 꺼풀수평이완(39.9%), 퇴행성 눈꺼풀속말림(24.0%), 아래눈꺼풀뒤당김(14.8%), 반흔성 눈꺼풀겉말림(6.6%), 가쪽눈구석인대변형(5.5%), 퇴행성 눈꺼풀겉말림(3.8%), 마비성 눈꺼풀겉말림(2.7%) 등이었고 가쪽눈꺼풀판띠고정술과 함께 다른 수술을 시행한 경우는 183안 중 167안(91.3%)으로 내시경적 눈물주머니코안연결술(30.5%), 아래눈꺼풀당김기재부착술(19.2%), 안쪽방추형결막절제술(13.8%), 중간층판 연장술(12.6%), 아래눈꺼풀 성형술(10.8%), Quickert 봉합술(4.2%), 호쯔씨수술(3.0%) 등이었다. 129명 중 116명(89.9%)에서 성공적인 결과를 보였다.
결론: 가쪽눈꺼풀판띠고정술은 아래눈꺼풀수평이완을 효과적으로 교정할 수 있으며, 단독으로 또는 다른 수술과 함께 다양한 적응증 에 이용될 수 있다.
<대한안과학회지 2015;56(6):803-810>