Introduction
Stroke causes damage to most of the functioning in the upper extremities and causes severe dis- abilities in the tasks involving the upper extremities such as eating, dressing, personal care, and most ac- tivities of daily living (ADL). According to a study by American Heart Association Statistics Committee and Stroke Statistics Subcommittee (2010), approx- imately 25∼74% of 50 million stroke survivors re- quire assistance with ADL. In addition to post-stroke medical management to prevent further cerebral damage, stroke rehabilitation is utilized to achieve better recovery in the first few months and to re- duce disability in the following years (Yoo et al, 2014). Motor function progressively declines post-stroke and the ultimate goal of rehabilitation becomes maintenance of function and acquisition of
ADL skills.
There are several methods in the rehabilitation of the upper extremities such as bilateral arm training (Stoykov et al, 2009), constraint-induced movement therapy (CIMT) (Hayner et al, 2010), continuous passive motion for the paretic shoulder (Bressel and McNair, 2002), circuit class training (Pang et al, 2006), and an intervention for the somatosensory functions of the paretic arm (de Diego et al, 2013).
Currently in Republic of Korea, post-stroke re- habilitation is centered on treating external symptoms and is dependent on a traditional biomedical model that focuses on one-on-one treatment between the therapist and the patient. It has been reported that functional impairment not only affects motor control and ADL but also affects psychological factors and quality of life in chronic stroke patients (Kim et al, 2014). In order to improve social relationships and
Corresponding author: Yong-Jin Jeon [email protected]
This work was supported by the National Research Foundation of Korea Grant funded by the Korean Government (NRF-2013S1A5B8A01055336).
Effects of a Group Exercise Program for the Upper Extremities on Sensory and Motor Function and Activities of Daily Living in
Chronic Stroke Patients: A Case Series
Myung-sook Ko1, MSc, PT, Yong-jin Jeon2, PhD, PT
1Dept. of Physical Therapy, The Graduate School, Yonsei University
2Dept. of Physical Therapy, School of Medical & Public Health, Kyungdong University
Abstract
1)The purpose of this study was to identify the effects of an upper extremities group exercise program based on motor learning in chronic stroke patients and to assess improvements in upper sensory motor function and activities of daily living (ADL). Five chronic stroke patients participated for the duration of 25 weeks. On the assessment of motor and process skills, there was a statistically significant improvement in motor area functioning in 4 of the subjects. In process area functioning, there was a statistically significant change in 3 of the subjects. Therefore, further studies are needed to assess sensorimotor area and ADL changes in chronic stroke patients to reduce medical cost and assess for positive psychological changes.
Key Words: Activities of daily living; Chronic stroke; Motor function; Sensory; Upper extremities group exercise program.
the psychological impact of disability, such as de- pression, support for task-specific circuit training has been growing since the first pilot study by Dean et al (2000).
In more recent studies by Langhammer and Stanghelle (2000), a task-oriented “motor relearning program” was shown to be more effective in the re- covery of independent ADL compared to the Bobath approach. Basedon motor learning theory, a new therapeutic approach for CIMT was introduced. The overall aim was to prevent learned nonuse and to improve functional abilities of the paretic upper ex- tremity through self-directed exercises. Winstein et al (2014) noted that in order for motor learning to occur, task-specific practice must be carried out.
Furthermore, Page et al (2005) has demonstrated that even the mental practice of cognitively rehearsing ADL activities can enhance motor function on the affected side.
In a similar context, Carr and Shepherd (2011) ap- plied a group circuit program that includes task-spe- cific exercises. It has been reported that this method is effective because the tasks are composed of ex- ercises more relevant to ADL. Furthermore, Pang et al (2006) have reported improved motor function and frequency of use in the upper extremities after a series of range of motion (ROM) exercises, which include repetitive movement of the wrist, functional electrical stimulation, and upper extremity group therapy with task-specific activities. In the past, the majority of task-specific group exercise programs has focused on lower extremity functioning and gait and there is a lack of research on the rehabilitation methods for the upper extremities in chronic stroke patients.
It is also important to consider sensory deficits in the rehabilitation of stroke patients. For example, hand function contains movement as well as sensa- tion (Floel et al, 2004). However, sensory deficit has not been emphasized in its importance even though its adverse effects have been known. According to Bobath, a patient with severe sensory deficit also
has a poor prognosis for functional recovery (Langhammer and Stanghelle, 2000).
Despite these studies, many researchers have tra- ditionally focused on motor functioning and have ne- glected to incorporate a consideration of the sensory deficits that occur with stroke. In order to examine the specific influences of sensory motor functions and their effects on ADL during upper extremity group exercises, the present study added outcome measures to evaluate cutaneous senses and changes in upper extremity motor function. Unfortunately, the literature offers only a few studies on the effective- ness of grip strength and the Korean Instrumental Activities of Daily Living for task-oriented training (Choi and Shin, 2014; Pand et al, 2006), whereas studies investigating tactile sensation and quality of performance of personal or instrumental ADL are still lacking. Therefore, the purpose of this study was to identify the effects of an upper extremity group exercise program based on motor learning in chronic stroke patients and to assess improvements in upper tactile sensation, motor function and quality of performance in personal and instrumental ADL.
Methods
Subjects
Seven stroke hemiplegic stroke patients enrolled in the study. Of these, two patients were disqualified during the duration of the study due to a low par- ticipation rate (<90%). Clear information regarding the purpose and method of this study was explained and voluntary consents were provided by the subjects. Inclusion criteria for the subjects were: (1) a stroke diagnosis; (2) ability to clearly communicate with no cognition problems, having scored higher than 24 on the Korean Mini-Mental Status Examination; (3) chronic illness with stroke for more than 12 months; (4) fully discharged from a re- habilitation program. Exclusion criteria were: (1) pre- vious participation in an exercise class for an upper
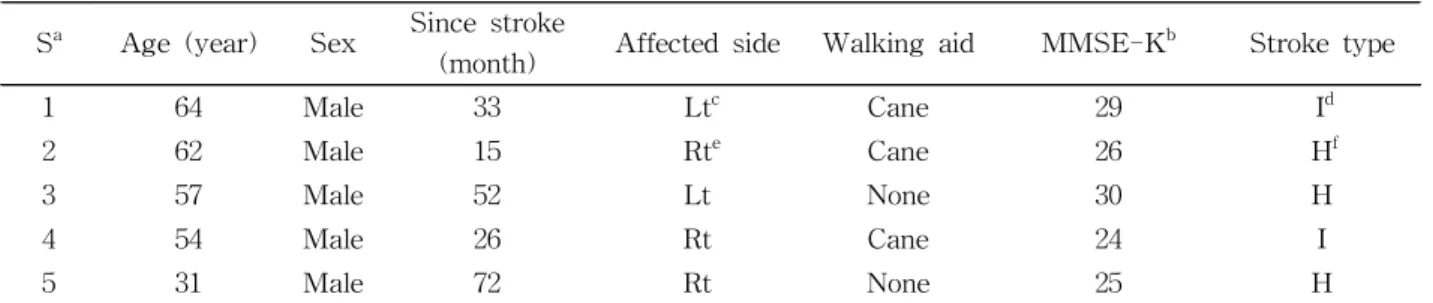
extremity group exercise program prior to the begin- ning of the study; (2) any medical conditions that would severely limit participation in the exercise program or that may interfere with outcome assess- ments performed in the study (Leroux, 2005); (3) di- agnosis of other musculoskeletal disorders that may affect the study. The research study included weekly meetings for 25 weeks. General characteristics of the subjects are shown in Table 1.
Evaluation and tools
All evaluations were conducted at baseline, 10 weeks and 25 weeks on completion of the inter- vention by a trained evaluator. The evaluator has performed treatment and stroke assessment for 15 years.
Two-point discrimination (2PD)
The Disk-Criminator (Pressure perceptor, NK Biotechnical Corporation, Minnesota, USA) was used to assess 2PD. Moving-2PD (M2PD) was tested first, followed by static-2PD (S2PD) testing. Stimuli were given to the affected palmar side of the distal phalanx index. Scores were given in millimeters within the two points that were perceived on at least 7 of 10 trials. The test-retest reliability of the S2PD is similar to that of Klingels et al (2010), with an interclass correlation coefficient (ICC) of .78 in uni- lateral cerebral palsy children.
Manual function test (MFT)
The MFT is used to assess changes in upper ex- tremities motor function in stroke patients. There are
8 sub-tests of the assessment that include examining gross upper limb motor function (4 items), grasping (2 items), and in-hand manipulation (2 items). One point is given to each item completed and 0 points are awarded if the item cannot be completed for a total maximum score of 32 points. The test-retest reliability of this test is excellent, with an ICC of .95 (Miyamoto et al, 2009).
Assessment of motor and process skill (AMPS)
The AMPS is used to assess a person’s ability in executing ADL or instrumental activities of daily liv- ing (IADL). During AMPS observation, a person performs 2∼3 ADL tasks from a variety of tasks in the assessment. The person’s skill in completing each goal-directed action is assessed in terms of in- dependence, safety, difficulty and efficiency in the context of ADL task performance. The person is rated on 16 motor ADL and 20 process ADL items.
The motor and process scores are then analyzed us- ing the many-faceted Rasch analysis, which converts raw scores into equal interval measures of ability (person ability measures), which are then expressed in log-odds units (logits). The person’s ability scores on the ADL motor and ADL process scales can also be evaluated relative to motor and process cut-off measures. The cut-off measures are 2.0 logits for the ADL motor scale and 1.0 logits for the ADL process scale. People who have ability measures be- low the cut-off measure on either the ADL motor or ADL process scales have demonstrated observable motor or process deficits that have impacted their Sa Age (year) Sex Since stroke
(month) Affected side Walking aid MMSE-Kb Stroke type
1 64 Male 33 Ltc Cane 29 Id
2 62 Male 15 Rte Cane 26 Hf
3 57 Male 52 Lt None 30 H
4 54 Male 26 Rt Cane 24 I
5 31 Male 72 Rt None 25 H
asubject, bKorean mini-mental state examination, cleft, dischemic, eright,fhemorrhagic.
Table 1. Characteristics of the subjects
ability to perform ADL tasks in an effective manner.
The test-retest reliability of the motor and process function areas when the two tasks were instructed were an ICC of .91 and .85, respectively. When only one task is given, ICC was .81 and .71 respectively.
There is typically higher reliability when two or more tasks are performed (Kirkley and Fisher, 1999).
Subjects were assessed based two tasks they se- lected among the therapist’s suggested tasks such as washing dishes, putting jam on sandwich, cooking ramen, vacuuming house, or making coffee.
Upper extremity group exercise program The group exercise program was composed of 7 stroke patients led by 1 occupational therapist and 1 physical therapist and assisted by 4 physical therapy and occupational therapy students. The students who participated were well educated in the purpose of the group exercise program, the motor functioning of the subjects, and the applied methods of the therapies prior to the study.
Because of the frailty of most members the group, all exercises were done in a seated position. Simple, portable, and inexpensive equipment was used and consisted of therabands (color-coded resistance rang- ing from 205 pounds to 9 pounds) and weighted hand-sized balls and putty. Each exercise session had a brief (5∼10 minutes) warm-up and cool-down period in which the subjects performed upper-ex- tremity stretches and active or self-assisted ROM exercises. The 6 workstations incorporated into the circuit were: (1) functional ADL training, (2) task
specific training, (3) upper extremity ROM, (4) sen- sory stimulation, (5) strength training, and (6) CIMT.
For further details on the training protocol see Appendix 1. Among the 6 workstations, 3 work- stations were trained by therapist’s presentation.
Subjects participated in upper extremity exercises for 10 minutes in one of three different workstations fol- lowed by 3 minutes of rest. During this progressive circuit exercise, subjects received demonstration and knowledge of results by the therapist and rests were utilized to provide additional feedback as well as to discuss difficulty levels. Each exercise was begun with one set of 5 repetitions and gradually pro- gressed to three sets of 15 as tolerated. The exercise program was conducted once a week for 25 weeks for 100 minutes each session. The structure of ther- apy was as follows.
Analysis methods
In this study, Treatment outcomes was used to ver- ify the changes in the factors (2PD and MFT) base- line, 10 weeks and 25 weeks. A multi-faceted Rasch computer program was used to derive AMPS IADL motor and process ability measures (Fisher, 1997).
Results
Two-point discrimination (2PD) and manual function test (MFT)
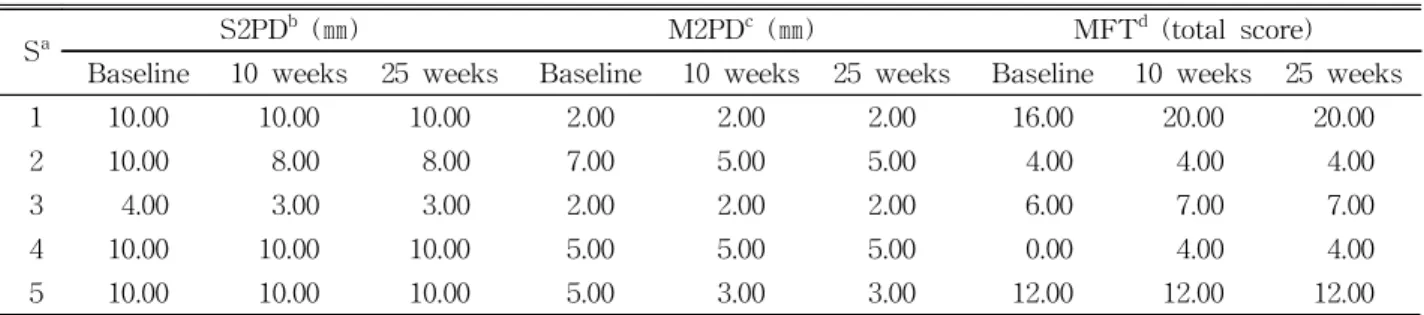
The changes in the 2PD and MFT at baseline, 10 weeks and 25 weeks are shown in (Table 2).
Sa S2PDb (㎜) M2PDc (㎜) MFTd (total score)
Baseline 10 weeks 25 weeks Baseline 10 weeks 25 weeks Baseline 10 weeks 25 weeks
1 10.00 10.00 10.00 2.00 2.00 2.00 16.00 20.00 20.00
2 10.00 8.00 8.00 7.00 5.00 5.00 4.00 4.00 4.00
3 4.00 3.00 3.00 2.00 2.00 2.00 6.00 7.00 7.00
4 10.00 10.00 10.00 5.00 5.00 5.00 0.00 4.00 4.00
5 10.00 10.00 10.00 5.00 3.00 3.00 12.00 12.00 12.00
asubject, bstatic-two-point discrimination, cmoving-two-point discrimination, dmanual function test.
Table 2. Subject scores on the 2PD and MFT
Assessment of motor and process skills (AMPS)
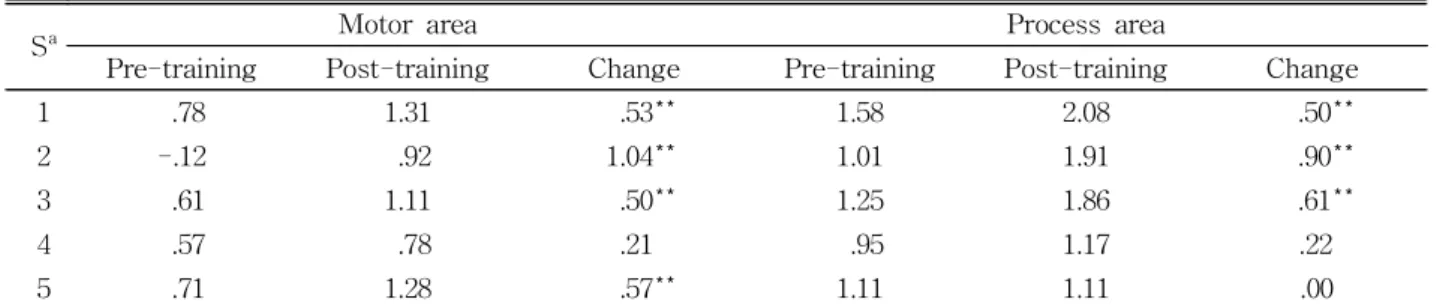
The change of ADL independence in local com- munity before and after therapy, as shown in (Table 3). Scores on the AMPS for ADL at baseline and 25 weeks post-therapy are shown in Table 4. In the motor area, there were statistically significant changes of more than .5 logit, while for 1 subject there was a statistically insignificant change of .21 logit. In the process area, 3 subjects showed statisti- cally significant changes of more than .5 logit, while no significant changes were observed in 2 of the subjects (Table 4).
Discussion
This study aimed to identify the effects of an up- per extremity group exercise program based on the motor learning of chronic stroke patients and to as- sess improvements in upper tactile sensation, motor function, and quality of performance in personal and
instrumental ADL. The results of our study show that the participants showed the significant improve- ment of motor and process skills in ADL.
Task-specific exercise programs based on strengthening, motor learning theory, and constraint induced movement therapy have been used to im- prove upper extremity function with verified ther- apeutic benefits (Hayner et al, 2010). Our study ex- amined the effects of upper extremity exercises in a group setting composed of functional ADL, ROM, CIMT, strengthening, and sensory stimulation for ADL tasks and senses that are closely related to up- per extremity motor function improvement. According to our study, AMPS values showed significant im- provements in subjects 1, 2, and 3 after upper ex- tremity motor training. Furthermore, MFT perform- ance increased in subjects 1 and 3 in addition to the AMPS values. However, in subjects 2 and 5, there were no significant changes in their MFT scores, al- though motor areas of the AMPS showed an increase. This may be due to how the dominant side is affected by stroke and its further effects on ADL.
Sa Motor area Process area
Pre-training Post-training Change Pre-training Post-training Change
1 .78 1.31 .53** 1.58 2.08 .50**
2 -.12 .92 1.04** 1.01 1.91 .90**
3 .61 1.11 .50** 1.25 1.86 .61**
4 .57 .78 .21 .95 1.17 .22
5 .71 1.28 .57** 1.11 1.11 .00
asubject, **statistically significant changes: logit≥.5.
Table 4. Changes in AMPS measurements for each subject (Unit: logit) Independent
(cut-off ability measure)
Motor area (2.0) Process area (1.0)
Pre-training Post-training Pre-training Post-training
1 .78 1.31 1.58* 2.08*
2 -.12 .92 1.01* 1.91*
3 .61 1.11 1.25* 1.86*
4 .57 .78 .95 1.17*
5 .71 1.28 1.11* 1.11*
*independent (cut-off ability measure).
Table 3. The change of ADL independence in local community before and after therapy
There was no difference between the superficial senses and upper extremity functioning. Thus, the main finding of this current study was that there were significant differences in the motor and process areas on the AMPS.
Our upper extremity group exercise program has progressive intensity and task specificity depending on the workstations. The three different workstations provided meaningful tasks relevant to the patients’
needs and were goal-oriented. Therefore, the exercise program was based on the preceding evidence of practice intensity and task specificity (Kwakkel, 2006;
Leroux, 2005) as the main component in improving sensory-motor functioning in the upper extremities and in ADL. Among rehabilitation methods utilized in this study, CIMT, a motor learning practice, has re- ceived a great deal of attention due to results that show meaningful gains even in chronic strokes of more than 6 months from the incident (Mark and Taub, 2004). In particular, modified CIMT, a low in- tensity form of CIMT, consists of immobilization of the intact side with a padded mitt during 0 to 90%
of waking hours and between 0 to 3 hours of training. This restraint is suggested to overcome the learned non-use of the affected arm in chronic hemi-paretic patients and to prevent compensatory strategies with the intact side in acute stroke pa- tients (Wu et al, 2010). In addition, electrostimulation of peripheral nerves and muscles can be applied dur- ing training as well as during functional training for simple movements (e.g., wrist extension) that are trained in a nonfunctional manner (Pomeroy et al, 2006).
Our study showed differential effects of treatment depending on the severity of upper-extremity impairment. Those who were moderately impaired tended to benefit the most see Table 3. Those with severe impairment, on the other hand, did not im- prove in functional abilities despite a significant in- crease in AMPS scores. Previous studies in acute and chronic stroke have also found that those with less severe impairment in the upper extremities ben-
efit more from treatment. Additionally, interventions are typically designed to decrease impairments in so- matosensory functions of the paretic arm by ex- posure to texture, shape, temperature or position (Conforto et al, 2010). Identification of the number of touches, lines, numbers and letters written on the arm and hand or discrimination of objects placed in hand. According to Krakauer (2006), variable practice rather than massed practice provides the benefit of increased generalization in learning new tasks.
Generalization is critical in the rehabilitation and treatment of somatosensory deficits because it may positively influence motor output (Conforto et al, 2010). Furthermore, upper extremity exercises includ- ing strength exercises for the paretic arm and func- tional task training have been previously studied.
Our study also included evidence-based activities for upper extremity training, which included the techni- ques mentioned above.
Unlike the MFT that separately assesses the function of the affected side, the AMPS focuses on how well the task is carried out, allowing for the use of the dominant hand during the task (Wittenberg et al, 2003). Therefore, improvements in ADL may be due to improvement of the affected dominant side. Additionally, subject 2 showed greater improvements in AMPS scores compared to subject 5 and this may be due to a shorter pathologic dura- tion of 15 months compared to the longer period for other subjects. This result converges with findings from other studies where the average level of func- tional ability is maintained between 6 months to 3 years post-stroke. Beyond 3 to 5 years, slight de- creases have been noted in other studies, most likely due to increasing age and comorbidities. These re- sults also agree with previous studies that have found that task-oriented activities generalize into abilities in ADL (Yoo et al, 2014).
Subject 1, he appeared to be a good candidated for intensive group training. There were no change in S2PD and M2PD, but MFT and AMPS showed sig- nificant improvement. It is thought that the func-
tional improvement of MFT and AMPS in subject 1 is due to the mass practice in the most optimal up- per extremity function that has helped motor learning (Krakauer, 2006). In subject 2, who was of 15 months post-stroke, there was significant improve- ment in motor and process areas as well as on the 2PD. It is thought that the functional improvement is due to practice intensity and task specificity brought about improvement in sensorimotor function and ADL (Kwakkel, 2006; Leroux, 2005). This supports the claim that subacute patients experience a faster recovery rate compared to chronic patients. Subject 3 had the best sensorimotor function in initial assess- ment among the subjects. He showed signigicant im- provement in various outcome measures. It seems that the undamaged hand sensory function affected the improvement of motor function (Conforto et al, 2010). Subject 4 on the other hand may have had greater difficulty due to a severe deficit in sensory and motor function. Despite the result that there was no improvement on the MFT, this subject showed AMPS improvements and this may be due to the AMPS’s focus on how well one can accomplish a given task while allowing the use of the less af- fected side (Wittenberg et al, 2003). Therefore, it may be assumed that long-term upper extremity training resulted in changes not only in motor func- tion of the affected side but also in the use of the compensated extremity. In subject 5, who was 31 years old and hemiplegic and independent walk.
Although we can predict the result of a good prog- nosis, there was no signigicant change in outcome measures. These results indicate that the duration of 72 months since stroke affects the improvement of upper extremity function and that the functional re- covery of stroke patients is concerned with the du- ration of stroke (Duncan, 1997).
According to a review by Steultjens et al (2003) sensorimotor training is not effective for improving ADL, extended ADL, social participation, or arm and hand function. Nottingham extended the ADL scale, which improved in the control group than the circuit
training group at 12 weeks (van de Port et al, 2012).
These results converge with the current study.
Successful ADL rehabilitation in patients with sensory deficits as severe as those in this study has not been reported previously. These results are preliminary. Limitations were that the sample size was small and in this case series there was no con- trol group. Increased numbers of subjects are needed in future studies and in long-term follow-up studies to clarify the efficacy of the upper extremity group exercise therapy program. Further study needs to in- volve various outcome measures as well such as the Stroke Impact Scale and the EuroQol, which can evaluate the cost-effectiveness of task-oriented cir- cuit class training when compared with individual care for patients.
Conclusion
This study investigated the effect of upper ex- tremity group exercise program in chronic stroke patients. Our results showed that upper extremity group exercise program is feasible and beneficial for improving motor and process skills in ADL. This finding may provide an excellent model for upper extremity rehabilitation programs for the stroke pop- ulation in the community. Therefore, upper extremity group exercise program may be used as a training suitable for chronic stroke patients purposes in in- dependent ADL performance. Future study is re- quired to further assess sensorimotor areas and pos- itive psychological changes.
References
American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics--2010 update: A report from the American Heart Association.
Circulation. 2010;121(7):e46-e215.
Bressel E, McNair PJ. The effect of prolonged static and cyclic stretching on ankle joint stiffness, torque relaxation, and gait in people with stroke.
Phys Ther. 2002;82(9):880-887.
Carr JH, Shepherd RB. Enhancing physical activity and brain reorganization after stroke. Neruol Res Int. 2011;2011:515938.
Choi SJ, Shin WS. The effect of patient-selected, task-oriented training on activities of daily liv- ing, quality of life, and depression in stroke patients. J Korean Soc Phys Med. 2014;9(2):
213-222.
Conforto AB, Ferreiro KN, Tomasi C, et al. Effect of somatosensory stimulation on motor function af- ter subacuted stroke. Neurorehabil Neural Repair.
2010;24(3):263-272.
Dean CM, Richards CL, Malouin F. Task-related cir- cuit training improves performance of locomotor tasks in chronic stroke: A randomized, controlled pilot trial. Arch Phys Med Rehabil. 2000;81(4):
409-417.
de Diego C, Puig S, Navarro X. A sensorimotor stimulation program for rehabilitation of chronic stroke patients. Restor Neurol Neurosci. 2013;31 (4):361-371. http://dx.doi.org/10.3233/RNN-120250 Desveaux L, Beauchamp M, Goldstein R, et al.
Community-based exercise programs as a strat- egy to optimize function in chronic disease: A systematic review. Med Care. 2014;52(3):216-226.
http://dx.doi.org/10.1097/MLR.0000000000000065 Duncan PW. Synthesis of intervention trials to im-
prove motor recovery following stroke. Top Stroke Rehibil. 1997;3:1-20.
Fisher AG. Multifaceted measurement of daily life task performance: Conceptualizing a test of in- strumental ADL and validating the addition of personal ADL tasks. Phys Med Rehabil State Art Rev. 1997;11:293-303.
Floel A, Nagorsen U, Werhahn KJ, et al. Influence of somatosensory input on motor function in pa- tients with chronic stroke. Ann Neurol. 2004;
56(2):206-212.
Gialanella B, Santoro R, Ferlucci C. Predicting out- come after stroke: The role of basic activities of daily living predicting outcome after stroke. Eur J Phys Rehabil Med. 2013;49(5):629-637.
Hayner K, Gibson G, Giles GM. Comparison of con- straint-induced movement therapy and bilateral treatment of equal intensity in people with chronic upper-extremity dysfunction after cere- brovascular accident. Am J Occup Ther. 2010;64 (4):528-539.
Kim DH, Oh MH, Park GA, et al. Effect of stroke patient’s ADL and self-esteem on the caregiving burden of caregivers. Journal of Rehabilitation Research. 2014;18(2):247-266.
Kirkley KN, Fisher AG. Alternate forms reliability of the assessment of motor and process skills. J Outcome Meas. 1999;3(1):53-70.
Klingels K, De Cock P, Molenaers G, et al. Upper limb motor and sensory impairments in children with hemiplegic cerebral palsy. Can they be measured reliably? Disabil Rehabil. 2010;32(5):
409-416. http://dx.doi.org/10.3109/09638280903171469 Krakauer JW. Motor learning: Its relevance to stroke recovery and neurorehabilitation. Curr Opin Neurol. 2006;19(1):84-90.
Kwakkel G. Impact of intensity of practice after stroke: Issues for consideration. Disabil Rehabil.
2006;28(13-14):823-830.
Langhammer B, Stanghelle JK. Bobath or motor re- learning programme? A comparison of two dif- ferent approaches of physiotherapy in stroke re- habilitation: A randomized controlled study. Clin Rehabil. 2000;14(4):361-369.
Leroux A. Exercise training to improve motor per- formance in chronic stroke: Effects of a com- munity-based exercise program. Int J Rehabil Res. 2005;28(1):17-23.
Mark VW, Taub E. Constraint-induced movement therapy for chronic stroke hemiparesis and other disabilities. Restor Neurol Neurosci. 2004;22(3-5):
317-336.
Miyamoto S, Kondo T, Suzukamo Y, et al. Reliability
and validity of the manual function test in pa- tients with stroke. Am J Phys Med Rehabil.
2009;88(3):247-255. http://dx.doi.org/10.1097/PHM.
0b013e3181951133
Page SJ, Levine P, Leonard AC. Effects of mental practice on affected limb use and function in chronic stroke. Arch Phys Med Rehabil. 2005;86 (3):399-402.
Pang MY, Harris JE, Eng JJ. A community-based upper-extremity group exercise program im- proves motor function and performance of func- tional activities in chronic stroke: A randomized controlled trial. Arch Phys Med Rehabil. 2006;87 (1):1-9.
Pomeroy VM, King L, Pollock A, et al.
Electrostimulation for promoting recovery of movement or functional ability after stroke.
Cochrane Database Syst Rev. 2006;19(2):
CD003241.
Steultjens EM, Dekker J, Bouter LM, et al.
Occupational therapy for stroke patients: A sys- tematic review. Stroke. 2003;34(3):676-687.
Stoykov ME, Lewis GN, Corcos DM. Comparison of bilateral and unilateral training for upper ex- tremity hemiparesis in stroke. Neurorehabil Neural Repair. 2009;23(9):945-953. http://dx.doi.
org/10.1177/1545968309338190
van de Port IG, Wevers LE, Lindeman E, et al.
Effects of circuit training as alternative to usual
physiotherapy after stroke: Randomised con- trolled trial. BMJ. 2012;344:e2672. http://dx.doi.
org/10.1136/bmj.e2672
Winstein C, Lewthwaite R, Blanton SR, et al.
Infusing motor learning research into neuro- rehabilitation practice: A historical perspective with case exemplar from the accelerated skill acquisition program. J Neurol Phys Ther.
2014;38(3):190-200. http://dx.doi.org/10.1097/NPT.
0000000000000046
Wittenberg GF, Chen R, Ishii K, et al. Constraint-in- duced therapy in stroke: Magnetic-stimulation motor maps and cerebral activation. Neurorehabil Neural Repair. 2003;17(1):48-57.
Wu CY, Hu HY, Huang N, et al. Determinants of long-term care services among the elderly: A population-based study in Taiwan. PLoS One.
2014;9(2):e89213. http://dx.doi.org/10.1371/journal.
pone.0089213
Yoo DH, Hong DG, Choi SY. Effect of virtual real- ity-based task training on upper extremity function and activities of daily living in stroke patients. Journal of Rehabilitation Research.
2014;18(2):289-308.
This article was received April 2, 2015, was re- viewed April 2, 2015, and was accepted May 2, 2015.
1) Warm up exercise: Extension exercises using ball, steps and wall, upper extremity stretches and active or self-assisted range of motion exercises (5∼10 minutes).
2) Main exercise: Three tasks were selected from the following and conducted for 40 minutes (30 minutes:
3 workstation×10 minutes, with 3 minutes of rest after each lap). This was a progressive circuit and subjects while exercising received feedbacks (visual and auditory) by the therapist. Rests were used to discuss about difficulties and to provide further feedbacks.
(1) Functional activities of daily living training:
Using phone, cooking, drinking beverage from cup, brushing hair, brushing teeth, vacuuming, dressing and undressing, writing a letter (Gialanella et al, 2013) (Figure 1).
(2) Task specific training:
Go-Stop card game, Korean traditional board game, general board game, writing a letter, gardening, typing on a computer, memory game (Wu et al, 2014) (Figure 2).
(3) Passive or self-assisted range of motion for joints with no or minimal active movement:
Using sling and ball (progressed by increasing the weight and increasing repetitions from 2 sets of 10 to 3 sets of 15) (Bressel and McNair, 2002) (Figure 3).
(4) Sensory stimulation:
Guessing the object by proprioception and tactile senses only, various sensory balls touch, grain vibrator on the palmar and extensor muscles of the hand, and various tactile stimuli (de Diego et al, 2013) (Figure 4).
(5) Strength training:
Elastic band (progressed by increasing the resistance of theraband and increasing repetitions from 2 sets of 10 to 3 sets of 15), putty, anti-gravity posture exercise, passive resistance exercise, functional electrical stimulation to wrist extensors (only for those with less than 20 of active wrist extension) (frequency, 100 ㎐; pulse duration, 150 seconds; on time, 10 seconds; off time, 10 seconds; ramp, 1 second; treatment time, 10~15 minutes) (Desveaux et al, 2014) (Figure 4).
(6) Constraint-induced movement therapy:
Rest splint was applied to the less affected arm. Tasks such as getting tea ready, putting on makeup, putting beans inside cup, Wii game, eating fruits, ball rolling were done using only the affected side.
3) Cool-Down exercise: A Cool-Down is performed in a seated position for 5 to 10 minutes and is devoted to flexibility and a range of motion (Leroux, 2005).
Appendix 1. Upper extremities group exercise program description
Figure 1. Functional activities of daily living (preparing a frozen dessert).
Figure 2. Task specific training (playing a game wearing functional electrical stimulation).
Figure 3. Upper extremities range of
motion exercise (sling). Figure 4. Sensory stimulation (proprio- ception).