접수일:2011년 4월 6일, 수정일:2011년 4월 14일, 승인일:2011년 4월 15일
책임저자:박 경 운 463-707 경기도 성남시 분당구 구미동 300 분당서울대병원 진단검사의학과
혈액형 검사이상을 동반한 Good’s Syndrome 1예
정소이3ㆍ이 경1ㆍ김미정1ㆍ장호은1ㆍ송상훈1ㆍ김홍빈2ㆍ박경운1ㆍ송정한1ㆍ한규섭3
분당서울대병원 진단검사의학과1, 내과2, 서울대병원 진단검사의학과3
= Abstract =
A Case of Good’s Syndrome with Weak ABO Reverse Type
Soie Chung3, Kyung Lee1, Mi Jung Kim1, Ho Eun Chang1, Sang Hoon Song1, Hong Bin Kim2, Kyoung Un Park1, Junghan Song1, Kyou Sup Han3
Departments of Laboratory Medicine1, Internal Medicine2, Seoul National University Bundang Hospital, Seongnam, Department of Laboratory Medicine, Seoul National University Hospital3, Seoul, Korea
Good’s syndrome (thymoma with immunodeficiency) is a rare cause of combined B-cell and T-cell immunodeficiency in adults. We present here a case of Good’s syndrome involving a 52 year-old man with an ABO blood group abnormality. He had undergone surgery for thymoma with myasthenia gravis 27 years ago. He also had a history of pulmonary tuberculosis, herpes zoster and pure red cell aplasia. On admission, he was suspected of having pneumonia, and S. pneumoniae was isolated from blood culture. The immunoglobulin levels were markedly decreased. Lymphocyte subset analysis revealed the absence of CD19+ B cells. The result of ABO typing showed a normal strong reaction on the cell typing, but a relatively weak reaction on the serum typing. Therefore, we performed ABO genotyping to confirm his ABO type, which was revealed to be B/O1. This case suggests that ABO typing should be performed when the diagnosis of Good’s syndrome is made.
Moreover, Good’s syndrome (thymoma with hypogammaglobulinemia) should be considered and evaluated for in patients with a weak ABO reverse type. (Korean J Blood Transfus 2011;22:54-58)
Key words: Good’s syndrome, Immunodeficiency, Weak ABO reverse type
Introduction
About 5∼10% of patients with thymoma have an immunodeficiency which is called as Good’s syn-
drome.1) It is characterized by hypogammaglobu- linemia and reduced or absent B lymphocytes. The common clinical features include recurrent sinopul- monary infection secondary to encapsulated organisms, such as Haemophilus influenza and Streptococcus
Table 1. Lymphocyte subset results Test
Absolute counts
(/µl)
Events
(%) Specificity CD3 3,615 95 T cell
CD4 1,119 29 Helper/Inducer T CD8 2,378 62 Suppressor/Cytotoxic T
CD19 7 0 B cell
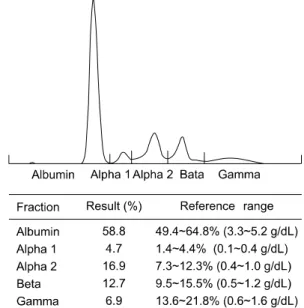
CD16+CD56 152 4 NK cell Fig. 1. Serum protein electrophoresis.
pneumoniae.2) Opportunistic pathogens such as cyto- megalovirus, herpes simplex virus, varicella-zoster virus, and human herpes virus 8 can also cause in- fection in these patients. In addition, patients with Good’s syndrome often have autoimmune conditions such as myasthenia gravis, pure red cell aplasia, per- nicious anemia, diabetes mellitus, and idiopathic thrombocytopenia. Anemia and leukopenia occur in more than 50% of patients, and both benign and malignant monoclonal gammopathy have been de- scribed in Good’s syndrome. Concerning immunologic problems, hypogammaglobulinemia, few or absent B cells, abnormal CD4+ to CD8+ T-cell ratio, CD4+
lymphopenia, and impaired T-cell mitogenic response were observed in many patients. Here, we present a case of Good’s syndrome involving a 52 year-old man with ABO blood group abnormality.
Case Report
A request for lymphocyte subset was submitted to laboratory. The patient was a 52 year-old man with complicated past medical history. He had surgery for thymoma with myasthenia gravis 27 years ago. He had been diagnosed as having pulmonary tuberculosis and treated with medication 10 years ago. He had
antithymoglobulin and prednisolone treatment history for pure red cell aplasia 3 year ago. Just 1 year be- fore, he developed herpes zoster. At current admission, he was suspected of having pneumonia the etiology of which was S. pneumoniae isolated from multiple blood cultures. Initial laboratory studies showed following results: Hb (13.9 g/dL), WBC [17.40×
109/L; metamyelocytes (2%), neutrophils (61%), lymphocytes (26%), monocytes (10%), eosinophils (1%)], platelets (270×109/L), and C-reactive protein (25 mg/dL). IgG, IgA, and IgM were markedly decreased (352 mg/dL, <24.9 mg/dL, and <17.1 mg/dL, respectively). Lymphocyte subset analysis revealed the absence of CD19+ B cells (Table 1).
T-SPOT.TB Test (Oxford Immunotec Ltd, Abing- don, UK) was negative. Serum protein electropho- resis and immunofixation electrophoresis was perfor- med (Fig. 1). The gamma region was scanty and
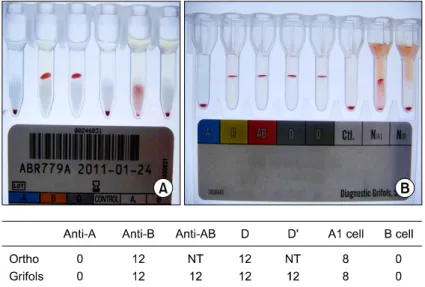
Fig. 2. ABO typing using Gel cards. (A) Ortho BioVue ABD card. (B) Grifols DG Gel ABO/Rh.
Fig. 3. Electropherogram of ABO genotyping.
there was no evidence of monoclonal gammopathy.
We performed ABO typing and agglutination re- actions were interpreted according to American Asso- ciation of Blood Banks (AABB) standards.3) We observed several large agglutinates against anti-B (score of 10) and no agglutination against anti-A in the ABO cell typing (Millipore UK Ltd, Living- stone, UK). Also, we found medium-size aggluti- nates with clear background against A1 cells (score of 8) and no agglutination against B cells in the ABO serum typing (Ortho-Clinical Diagnostics, Raritan, NJ, USA). In the ABD card, cell typing showed 1 solid agglutinate (score of 12) against anti- B and serum typing showed several large agglutinates (score of 8) against A1 cells using two different commercial gel cards Ortho BioVue ABD card (Ortho-Clinical Diagnostics, Raritan, NJ, USA) and Grifols DG Gel ABO/Rh (Diagnostic Grifols, Bar- celona, Spain) (Fig. 2). The result of serum typing was, notably, relatively weak. Then, we performed
ABO genotyping using the SNaPshot multiplex kit (Applied Biosystems, Foster City, CA, USA) accor- ding to our previously described methods.4) The ABO genotype of the patient revealed to be B/O1 (Fig. 3).
After antibiotic treatment for pneumonia, the in- fections signs were resolved. The patient was given
intravenous immunoglobulin (IVIG) infusion and recommended to repeat monthly IVIG infusions and discharged.
Discussion
The weak ABO reverse is not rare in blood bank.
In newborn anti-A and anti-B are usually unde- tected.5) However, hypogammaglobulinemia in elderly or immunocompromised patient resulting in de- creased antibody titer is the most common cause.5) The decreased anti-A or anti-B titer was also reported in patients with X-linked Wiskott-Aldrich syndrome or after massive plasma exchange.
Although there had been reports of patients with Good’s syndrome, the case with weak ABO reverse has not been noted. The early study in 1956 con- cerning acquired hypogammaglobulinemia documented reduced blood group isohemagglutinins and specific antibody values.6) The patient blood was type B and Rh positive, but there were no anti-A isoagglutinin.
Furthermore, there are 2 case reports of common variable immunodeficiency diagnosed by ABO discrepancies.7,8) Both of the patients had cell types of A+ but the anti-B isohemmaglutinins were absent.
The weak reaction of serum typing in our case is consistent with these previous case reports of other primary immunodeficiency diseases.
However, when evaluating immunodeficiencies in- cluding Good’s syndrome, ABO testing is not routinely performed. This might render the lives of patients when the patients need urgent transfusion.
Furthermore, in Good’s syndrome patients, hema- tologic abnormalities are common. In a recent re- view containing collective data of 87 patients with
Good’s syndrome, the incidence of anemia was 85%.9) The incidences of leukopenia, neutropenia, thrombocytopenia were 46.5%, 15.1%, 20% respec- tively. The mechanism of the anemia was pure red cell aplasia in 31 (41.9%) of the patients. Moreover, there is a report of PRCA associated with Good’s syndrome Hb of 3.7 g/dL.10) The patient in our case has normal Hb at the point of diagnosis of Good’s syndrome. However, the time when he was dia- gnosed as PRCA, Hb was 5.8 g/dL. He received pack RBC transfusions back then.
This case suggests that Good’s syndrome (thy- moma with hypogammaglobulinemia) should be considered and evaluated in patients with weak ABO reverse type.
Summary
Good 증후군은 성인에서 발생하는 B 세포와 T 세포 면역 결핍증의 드문 원인질환으로 흉선종과 함께 저감마글로불린혈증이 동반되는 것이 특징 이다. 임상적으로는 반복적으로 Haemophilus in- fluenza, Streptococcus pneumonia 등에 감염되거나 기회감염이 생기면 의심할 수 있다. 또한 다수의 환자에서 빈혈이 동반되며 이중, 30% 정도가 자 가면역질환인 진정적혈구계무형성증인 것으로 밝혀져 있다. 이에 저자들은 B형 Rh 양성인 Good 증후군 환자에서 혈액형 검사상 혈구형 검사는 정상이었으나 혈청형의 반응이 약하게 나온 경우 를 보고하고자 한다. 이는 혈액형 검사이상으로 다른 일차성 면역결핍질환의 하나인 공통 가변성 면역결핍증을 진단하였던 기존의 두 증례보고와 일치하는 소견이다. 결론적으로 흉선종과 반복적 인 세균감염의 병력이 있는 환자에서 혈구형 검 사는 정상이나 혈청형 검사에 이상이 있어 ABO
불일치를 야기하는 경우에 Good 증후군을 의심 할 수 있어야 한다. 또한 Good 증후군을 비롯하 여 면역결핍질환으로 진단이 내려진 환자는 혈액 형을 신중을 기하여 평가하여야 한다.
References
1. Primary immunodeficiency diseases. Report of an IUIS Scientific Committee. International Union of Immunological Societies. Clin Exp Immunol 1999;118 Suppl 1:1-28
2. Kelleher P, Misbah SA. What is Good's syn- drome? Immunological abnormalities in pa- tients with thymoma. J Clin Pathol 2003;56:
12-6
3. Roback J, Combs MR. Technical manual. 16th ed. Bethesda: American Association of Blood Banks, 2008:915-6
4. Hyun J, Chang HE, Heo SR, Song SH, Park KU, Song J, et al. ABO genotyping using a multiplex single-base primer extension reaction.
Korean J Blood Transfus 2007;18:79-88 5. Klein HG, Anstee DJ. Mollison's blood tran-
sfusion in clinical medicine. 11th ed. Malden,
Massachusetts: Blackwell Publishing, Inc., 2005:
122-8
6. Martin CM, Gordon RS, Mccullough NB. Ac- quired hypogammaglobulinemia in an adult;
report of a case, with clinical and experi- mental studies. N Engl J Med 1956;254:449-56 7. Oh SH, Kang CI, Kim J, Park TS. ABO dis- crepancy in a young Korean serviceman with common variable immunodeficiency. Ann Hematol 2010;89:629-30
8. Julius CJ, Wade M, Waheed A, McNeil DL, Kennedy MS. Common variable immunode- ficiency: diagnosis by absent ABO reverse type. Immunohematology 1997;13:80-3 9. Kelesidis T, Yang O. Good's syndrome re-
mains a mystery after 55 years: a systematic review of the scientific evidence. Clin Immunol 2010;135:347-63
10. Kuribayashi K, Fujimi A, Kobune M, Takimoto R, Kikuchi S, Iyama S, et al. Pure red cell aplasia associated with Good's syndrome accom- panied by decreased stem cell factor produc- tion in the bone marrow. Intern Med 2010;49:
377-82