혈액투석치료시간외 영상학적 감시
심동재1, 김일중2
가톨릭대학교 의과대학 인천성모병원 영상의학과1, 가톨릭대학교 의과대학 부천성모병원 영상의학과2
Imaging Surveillance Outside Dialysis Sessions
Dong Jae Shim1, Il Jung Kim2
1Department of Radiology, Incheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
2Department of Radiology, Bucheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
서 론
지속적인 혈액 투석이 가능하도록 혈관접근로(Vascular access)의 관리는 투석환자의 삶의 유지에 매우 중요하다. 투석 과정에서 이학 적 검사를 포함하여 다양한 방법으로 혈관접근로의 이상유무에 대해 평가하게 되며 이상이 의심되는 경우 객관적 평가로서 초음파 및 혈 관조영검사를 하게 된다. 초음파를 이용한 정기적 감시 프로그램의 효용성에 대해서는 아직까지 충분한 근거가 쌓이지 않아 논란의 여 지가 있다[14]. 현재까지 연구에서는 정기적 감시와 선제적인 혈관 접근로 협착 치료는 혈전 생성의 위험을 감소시키나 혈관접근로 수 명 연장에 도움이 되지 않는 것으로 제시되며 European society for vascular surgery (ESVS)에서도 AVF의 경우 선제적 치료가 추천되나 AVG에서는 초음파감시와 선제적 치료를 추천하지 않는다[57]. 초 음파는 정기적 감시에서도 중요한 역할을 하나 치료를 위한 시술 전 의 구조적 상태와 기능평가에도 매우 유용하게 활용되어 검사법에 대해 정확한 이해가 중요하다[1]. 혈관조영술은 치료를 전제로 하지 않는 진단 목적으로 추천되지 않으나 혈관접근로에서 협착부위를 확
인할 수 있는 표준 검사법으로 여겨진다[5]. 전산화단층촬영은 중심 정맥관 협착이 의심될 때 활용도가 높다. 자기공명혈관촬영도 가능 하나 비용효과 측면에서 불리하여 널리 활용되지는 않는다.
정기적 감시의 구체적 방법에는 Monitoring과 Surveillance 두 가 지가 있다. Monitoring은 혈관접근로 이상을 정기적 이학적 검사 를 통해 시행하고 이상 소견이 있을 때 특수 검사를 추천하는 것이 고 Surveillance는 정기적으로 도관 내 혈류를 측정하는 특수 장비를 이용하여 검사하는 것을 말한다[8]. 혈관접근로의 혈류를 측정하는 surveillance는 AVG는 매달, AVF는 3 개월에 한번이 추천된다[5]. 개 별 검사법에서 구체적인 방법을 알아보기로 한다.
본 론
1. 초음파 검사
초음파는 비침습적인 방법으로 가장 먼저 추천되는 영상 검사법 이다. 협착부위의 발견과 정도의 측정, 혈전 유무를 진단하는데 매우
Received: May 15, 2019, Revised: Jun 5, 2019, Accepted: Jun 27, 2019 책임저자 : 심동재
우 21431, 인천시 부평구 동수로 56, 가톨릭대학교 의과대학 인천성모병원 영상의학과 Tel: 032-280-5236, Fax: 032-280-5230, E-mail: inharad@naver.com
대 한 투 석 혈 관 학 회 지 : 제 2 권 제 2 호
Journal of Korean Dialysis Access 2019;2(2):27-30
Review Article
Imaging surveillances take important part in keeping a patency of vascular access before hemodialysis failure.
However, there are still controversies over the usefulness of regular surveillance for improving access longevity. Better understanding of surveillance indication, interval, and imaging method is crucial for reducing costs and improving vascular access survival. This review will address recent issues about imaging surveillance outside dialysis sessions.
Key Words: Arteriovenous fistula, Duplex doppler ultrasonography, Hemodialysis
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © The Korean Society for Dialysis Access | eISSN: 2635-8603
대한투석혈관학회지 : 제 2 권 제 2 호 2019
28
효과적이다[5]. 그러나 시술자의 경험에 의존하는 부분이 크고 이후 혈관 촬영술을 이용한 치료와 중심정맥관 협착의 진단에도 제한적이 다[5].
초음파의 탐색자(probe or transducer)는 715 MHz의 선형(high
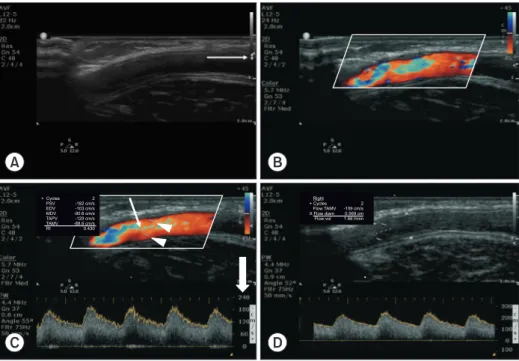
frequency linear array)을 선택하고 제조업체에서 제공하는 vascular setting으로 설정하고 검사하게 된다. 영상의 범위는 혈관접근로가 매 우 표피에 위치함을 고려할 때 23 cm내외로 적절히 설정하고 초점 (focus)을 혈관에 맞추도록 한다. 도플러검사를 할 때는 steering기능 을 이용하여 각도를 주는 것이 필요하며 속도를 정확하게 측정하기 위해서는 cursor의 방향을 혈관에 수평으로 angle을 조정하되 60도 이하의 각도를 취하도록 해야한다[9]. 60도가 넘어가면 속도가 지나 치게 과장되기 때문이다. Peak systolic velocity (PSV)를 측정하기 위 해서는 도플러 range와 baseline을 적절히 조정하여 파형이 모두 포함 되도록 해야 한다. Gain을 높이면 느린 혈류도 포착할 수 있으나 주 위에 인공물이 증가할 수 있다. Sample volume은 혈관의 전체 지름을 포함하도록 조절하여야 한다. 중심부로만 설정하면 상대적으로 속도 가 느린 혈관벽 쪽의 유속이 빠지게 되어 평균속도가 높게 측정되어 결과적으로 혈류량이 과장되게 된다. 또 파형이 기준치(baseline) 이 하가 많이 포함되는 경우 평균 유속이 감쇄 될 수 있으므로 기준치 이상으로 일정한 파형이 나오는 곳에서 측정해야 한다(Fig. 1). 혈류 량 측정 시 환자는 편안한 상태이어야 하고 일정한 패턴이 나오는 지
세 번 이상 측정하는 것이 좋다[9].
자가동정맥루(AVF)에서는 초음파 검사 시 협착이 가장 호발하 는 문합부 주위를 먼저 검사한다. 동맥부위의 협착여부와 문합부 수 cm 이전에서 파형 도플러 검사로 수축기 최고 속도(Peak systolic velocity)와 이완기말 속도(End diastolic velocity)를 측정한다. 문합부 에서는 협착유무와 주위 혈종, 가성 동맥류 등을 확인한다. 정맥부위 에서는 피부로부터의 깊이, 정맥직경, 협착여부, 가성동맥류, 감염 등 을 확인하고 협착이 있는 경우 협착 수cm이전 부위와 최고속도를 측 정하여 PSV비를 산출한다. 혈류량을 측정은 측정부위의 직경과 도 플러검사에서 평균속도(Timeaveraged mean velocity, TAMV)를 측 정하여 산출할 수 있는 데 TAMV는 대부분의 초음파 장비에서 측정 할 수 있으면 초음파 장비에 따라 혈관직경을 입력하는 경우 자동으 로 혈류량이 제공되기도 하며 그렇지 않은 경우 계산을 할 수도 있 다. 혈류량 계산식은 Volume flow (ml/min)=crosssectional area (cm2)
×mean velocity (cm/sec)×60, Cross sectional area=Diameter2×π/4, Mean velocity=average velocity over several cardiac cycle의 공식에 의해 산출할 수 있다(Fig. 2). 직접 혈관접근로에서 측정할 수도 있으 나 단면적측정과 도플러 각도에 따라 차이가 많이 날 수도 있어 재연 성이 높은 방법으로 최근에는 근위부 상완동맥(brachial artery) 혈류 량에서 반대편 상완동맥의 것을 빼는 방법을 이용하기도 한다[5]. 상 완동맥이나 쇄골하동맥은 혈관접근로와 비교하여 일정한 원형을 갖
A B
C D
2 -109 cm/s 0.569 cm 1.66 l/min Right + Cycles
Flow TAMV X Flow diam Flow vol 2
-182 cm/s -103 cm/s -90.6 cm/s -129 cm/s -88.6 cm/s 0.430 + Cycles
PSV EDV MDV TAPV TAMV RI
Fig. 1. Doppler US surveillance of arteriovenous graft (AVG). A 73-year-old woman with brachio-axillary AVG had undergone 7 times balloon angioplasty and a stent-graft placement for 2 years follow-up. (A) Two-dimensional gray-scale image should be adjusted for optimal image acquisition regarding depth (mostly within 2 cm) and focus (white arrow). Examiner should try to find any stenosis within graft and anastomosis. (B) Optimal site for flow-measurement can be evaluated on color Doppler image. (C) Spectral image (or pulse wave image) can be obtained after placing flow-measuring cursor within the graft with appropriate angle (arrow, parallel to flow) and sample volume (arrow heads, covering full diameter). Range (solid arrow) and baseline of pulse wave should be also adjusted appropriately. Applying automatic measurement function of US system, peak systolic velocity and time-average mean velocity (white underline) can be obtained. (D) Volume flow (white underline) can be calculated by measuring diameter of fistula or by using formula (in this presenting case: 0.569 cm×0.569 cm×π/4×109 cm/s×60=1.66 L/min).
심동재 외 : 혈액투석치료시간외 영상학적 감시 29
고 상대적으로 직선의 경로이며 난류가 없어 정확한 혈류량 측정에 유리하다[9].
인조혈관동정맥루에서 50%의 협착을 시사하는 소견은 PSV≥400 cm/sec, PSV ratio≥2 or 3이다. 자가 동정맥루에서 50% 이상의 협착 을 시사하는 소견 또한 graft 와 같으나 PSV 비는 문합부 혹은 협착 부위 PSV와 요골 동맥 PSV를 비교하게 된다. 유출정맥에서의 협착 소견은 PSV ratio 의 증가(≥2 or ≥3) 이다. 인조혈관동정맥루에서도 동맥 문합부의 인접 근위부에서 정맥 문합부 이후의 유출정맥까지 자가정맥과 동일하게 시행하면 된다[1].
혈류 계산을 통해 풍선혈관확장술이 필요한 경우는 European Best Practice Guideline Recommendation은 forearm fistula의 경우 blood flow가 300 ml/min 이하, Graft의 경우 blood flow가 600 ml/
min 이하 이거나 매월 추적검사에서 20% 이상의 유량 감소가 있 는 경우이다[10]. ESVS에서는 AVF에서는 blood flow <500 ml/min, AVG에서는 <600 ml/min일 때 협착과 연관이 있는 소견이나 반드시 다른 임상 소견과 연관되어 intervention을 고려해야 하며 volume 감 소의 경우 33%이상되야 한다고 제시하고 있다[5]. NKFK/DOQI 지 침에서는fistula Blood flow <400500 ml/min, graft Blood flow <600 ml/min 이거나 Flow가 1000 ml/min 이상이나 4개월에 걸쳐 25% 이 상 감소하는 경우이다[1,4]. 이러한 혈류 감소 소견이 있더라도 한 가 지 비정상 결과에 의해 시술을 고려해서는 안되고 시간에 따른 경향 성 파악이 더 효과적임을 유의해야 한다[4]. 초음파에서 확인할 사 항은 1. 상완동맥 또는 쇄골하 동맥의 혈류량(volume flow), 2. 투석 접근로를 포함한 유입동맥에서부터 유출 정맥까지의 전경로의 개 존 여부, 3. 혈전, 진성 또는 가성동맥류, 체액 저류 유무, 4. 비정상 적인 혈류 속도 또는 맥박, 5. 심부정맥으로 유출되는 정상적 혈류 방향 여부, 6. 도관의 직경, 깊이, 7. 천자부위의 혈전 또는 내막 날
개(flap), 8. Bmode에서의 협착 정도와 최고혈속도(PSV), pre/post
stenosis, PSV ratio이다[1]. 초음파 소견은 믿을 만한 혈류량 계산법이 고 dilution method와도 일치하며 혈관조영술과도 잘 연관되는 것으 로 알려져 있다[3].
2. 혈관조영술(Angiography or fistulography)
Surveillance에서 정맥 협착이 의심되는 경우 angiography로 협착 의 위치와 정도를 확인할 수 있다. 투석 전후에 투석용 바늘을 이용 하여 시행할 수도 있으나 혈관 풍선 성형술과 함께 시행되기도 한다.
문합부 근처 정맥을 천자하여 말초정맥에서 중심정맥까지 검사하고 동맥 부위까지 영상을 얻고자 할 때는 천자 부위 상방을 압박하고 영 상을 얻을 수 있다[11]. 협착 부위와 혈전 유무 등을 직관적으로 알 수 있다는 장점이 있다. 액와 정맥에서는 근육이나 유방에 의한 가성 협착이 보일 수 있으므로 겨드랑이를 벌리고 검사한다[11]. 검사에서 측부 순환이 관찰되면 협착의 간접적인 증거로 협착부위를 찾기 위 해 다각도로 촬영하도록 한다. Fistulogram에서 이상 소견이 없으나 임상적으로 문제가 있을 때는 유입 동맥까지 반드시 검사해야 한다.
임상적이나 혈류학적 문제는 없고 영상에서만 협착이 있는 경우 풍 선확장술의 적응증이 되지 않는다[11].
3. 자기공명혈관촬영술(Magnetic resonance angiography, MRA)
MR angiography는 비침습적으로 정확히 협착을 진단할 수 있으나 비용이 많이 들고 투석 중에 활용하기 어려워 연구 단계에서만 활용 되고 있다. 특히 조영제를 사용하는 CEMRA는 Gadoliniuminduced nephrogenic systemic fibrosis를 초래할 수 있어 위험과 이득을 잘 따 져 보고 검사 해야겠다[5]. 조영제를 사용하지 않는 NCEMRA의 유
A B C
D E F
LOGIQ
E9 PS
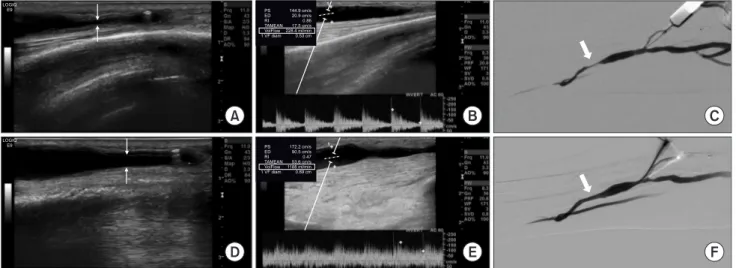
ED RI TAMEAN VolFlow 1 VF diam
172.2 cm/s 90.5 cm/s 0.47 53.6 cm/s 1188 ml/min 0.69 cm
+ + +
1+
+ + +
1+ PS
ED RI TAMEAN VolFlow 1 VF diam
144.9 cm/s 20.9 cm/s 0.86 17.5 cm/s 228.4 ml/min 0.53 cm LOGIQ
E9
Fig. 2. Doppler US before and after angioplasty. A 59-year-old man with radiocephalic arteriovenous fistula (AVF) presented with AVF malfunction. (A) A gray-scale US shows significant focal stenosis at fistula (arrows). (B) Volume-flow measurement using Doppler US demonstrates decreased flow rate (228.4 ml/min, white box). (C) A digital subtraction angiography (DSA) shows focal severe stenosis which corresponds to US finding. (D) A two-dimensional US after balloon angioplasty shows improvement of stenosis (arrows). (E) A Doppler US shows increased flow rate up to 1188 ml/min (white box) at which hemodialysis is possible. (F) A DSA also demonstrates improvement of stenosis (solid arrow).
대한투석혈관학회지 : 제 2 권 제 2 호 2019
30
용성에 대해 기대가 있으나 아직까지 보고된 결과는 없다[3].
4. 전산화단층혈관촬영술(Computed tomography angiography, CTA)
CTA는 조영제와 방사선을 이용하기 때문에 다른 방법으로 진단 이 어려울 때만 제한적으로 사용하게 된다. 풍선성형술을 동반한 혈 관조영술보다는 비 침습적인 방법이고 혈관조영술과도 좋은 연관성 을 보인다. 주로는 중심 정맥과 협착이 의심될 때 유용하게 활용될 수 있다[11].
결 론
자가동정맥루의 혈전생성방지와 수명연장을 위해서는 투석기간 외에도 영상검사를 통한 비침습적 정기감시는 유용하다. 아직까지 인조혈관동정맥루에서는 정기감시의 효용성은 제한적이다. 초음파 를 이용한 혈액투석루 검사법에 대한 이해는 정기감시와 혈관확장술 및 수술 후 성숙 평가에 유용할 수 있다.
REFERENCES
1. Roh YN. Ultrasound Evaluation for Hemodialysis Access.
Journal of Korean Dialysis Access. 2018; 1(1): 1-6.
2. Allon M, Robbin ML. Hemodialysis vascular access monitoring: current concepts. Hemodial Int. 2009; 13(2):
153-62.
3. Dolmatch BL, Vazquez MA, Davidson IJ. End-Stage Renal Disease and Dialysis Access: Epidemiology, Natural History,
and Diagnostic Monitoring. In: Geschwind JFH, Dake MD.
Abrams’ Angiography Interventional Radiology. 3rd Ed.
Philadelphia: Lippincott Williams & Wilkins, 2014; 1037-78.
4. NKF KDOQI Guidelines. Clinical Practice Guidelines and Clinical Practice Recommendations 2006 Updates Hemodialysis Adequacy Peritoneal Dialysis Adequacy Vascular Access. Available at: http://kidneyfoundation.
cachefly.net/professionals/KDOQI/guideline_upHD_PD_
VA/va_guide4.htm. Accessed 2 March 2019.
5. Schmidli J, Widmer MK, Basile C, et al. Editor's choice–
vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2018; 55(6): 757-818.
6. The American Society of Nephrology. Interventional nephrology and dialysis access. NephSAP. 2018; 17(2): 117- 96.
7. Ravani P, Quinn RR, Oliver MJ, et al. Preemptive correction of arteriovenous access stenosis: a systematic review and meta-analysis of randomized controlled trials. Am J Kidney Dis. 2016; 67(3): 446-60.
8. Roberts A. Surveillance of Hemodialysis Access. In: Mauro MA, Murphy KPJ, Thomson KR, et al. Image-guided Interventions. 2nd Ed. Philadelphia: Elsevier, 2014; 840-3.
9. Deane C. Ultrasound of hemodialysis access. In: Thrush A, Hartshorne T. Vascular Ultrasound. 3rd Ed. Philadelphia:
Elsevier, 2010; 275-91.
10. Tordoir J, Canaud B, Haage P, et al. EBPG on vascular access. Nephrol Dial Transplant. 2007; 22(suppl_2):ii88- ii117.
11. Korean Society of Interventional Radiology. Interventional Radiology. 2nd Ed. Seoul: Ilchokak, 2014.