Duodenal Loop Obstruction as an Unusual Cause of Acute Pancreatitis: A Case Series
Hyeonmin Lee, Yonghyeok Choi, Hyewon Jeong, Jae Kyu Lim, Taeyoung Jung, Joung-Ho Han, and Seon Mee Park Department of Internal Medicine, Chungbuk National University College of Medicine, Cheongju, Korea
Duodenal loop obstruction is an unusual cause of acute pancreatitis. Increased intraluminal pressure hinders pancreatic flow, causing dilatation of the pancreatic duct and inducing acute pancreatitis. We experienced three cases of acute pancreatitis that resulted from duodenal loop obstruction after (1) an esophagectomy with gastric pull-up procedure for esophageal cancer, (2) a gastrectomy with Billroth I reconstruction for gastric cancer, and (3) a gastrojejunostomy for abdominal trauma. An abdominal CT scan revealed a distended duodenal loop, dilated pancreatic duct, and inflamed pancreas with fluid collection. Acute pan- creatitis with duodenal loop obstruction was diagnosed by abdominal pain, elevated serum amylase/lipase, and abdominal CT findings. Immediate decompression with a nasogastric tube was performed, and all patients showed improvement within one week after admission. Each patient was followed up for more than two years without recurrence. Our findings suggest the usefulness of nasogastric tube decompression as the first line of treatment for acute pancreatitis related to duodenal loop obstruction. (Korean J Gastroenterol 2016;68:326-330)
Key Words: Pancreatitis, acute; Duodenal obstruction; Decompression
Received July 4, 2016. Revised September 27, 2016. Accepted October 4, 2016.
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2016. Korean Society of Gastroenterology.
교신저자: 박선미, 28644, 청주시 서원구 충대로 1, 충북대학교 의과대학 내과학교실
Correspondence to: Seon Mee Park, Department of Internal Medicine, Chungbuk National University College of Medicine, 1 Chungdae-ro, Seowon-gu, Cheongju 28644, Korea. Tel: +82-43-269-6019, Fax: +82-43-273-3252, E-mail: [email protected]
Financial support: None. Conflict of interest: None.
INTRODUCTION
Acute pancreatitis caused by duodenal loop obstruction rarely develops after abdominal surgery,1 ventral2,3 or in- ternal hernia,4 or gastric distension with binge eating.5 Afferent loop obstruction (ALO), which is the most common cause of duodenal loop obstruction, develops after gas- trectomy with Billroth II anastomosis.1 However, it is possible for a functional blind duodenal loop to appear after Roux-en-Y gastrectomy, gastric bypass surgery, biliary diversion, and in- ternal hernia.1 In addition, a markedly distended stomach triggers acute pancreatitis with duodenal compression.5
Increased intraluminal pressure of the duodenum and pancreatic duct inhibits pancreatic juice drainage and in- duces acute pancreatitis.1 Ileus and acute pancreatitis are closely related; both are causes and results, and vice versa.6 To date, surgical treatment has been the most common method for ALO. Recently, however, non-surgical methods like endoscopy-assisted nasojejunal tube drainage,7,8 so- nography-guided percutaneous tube enterostomy,9 or metal stent insertion at the stenotic segment have gained popularity.10
We experienced three cases of acute pancreatitis asso- ciated with duodenal loop obstruction. These patients first
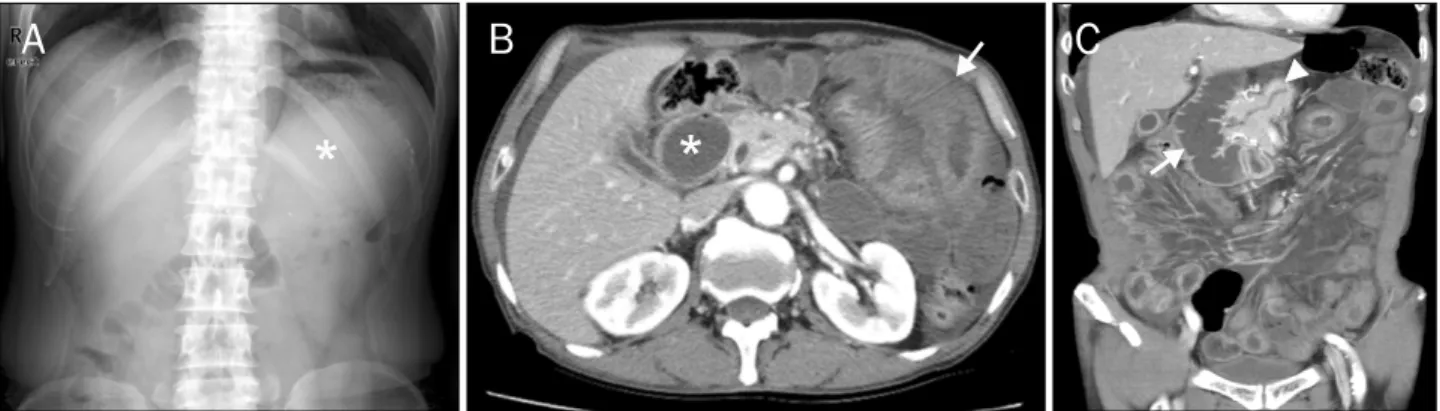
Fig. 1. Plain abdomen and abdominal CT images of Case 1. (A) Suspicious distended stomach filled with fluid (asterisk) without abnormal bowel gas. (B) Axial view. Dilatation of the duodenum (asterisk) and diffuse small bowel wall thickening (arrow). (C) Coronal view. Distended duodenal loop (arrow) and mild pancreatic duct dilation (arrowhead).
presented with mechanical symptoms, such as vomiting and abdominal distension, followed by abdominal pain. Each pa- tient had undergone gastrectomy with Billroth I re- construction, esophagectomy with a gastric pull-up proce- dure, and gastrojejunostomy two years, two years, and 11 years prior, respectively. The symptoms of all patients showed improvement after nasogastric tube decom- pression, fluid replacement, and pain control. Herein, we re- port a case series and provide literature review.
CASE REPORTS
1. Case 1
A 68-year-old man presented to the emergency depart- ment with severe abdominal pain that lasted for 12 hours.
Two years prior, he had undergone a distal esophagectomy with gastric pull-up procedure and a pyeloplasty for esoph- ageal cancer. He denied drinking alcohol or smoking. A phys- ical examination revealed a distended abdomen, epigastric tenderness, and hypoactive bowel sounds. Vital signs were within normal limits. Laboratory data were as follows:
Amylase 997 IU/L, lipase 1,070 IU/L, white blood cells 12,230/mm3, CRP 0.13 mg/dL, AST 48 IU/L, ALT 6 IU/L, ALP 66 IU/L, GGT 36 IU/L, PT 103.7%, total bilirubin 0.64 mg/dL, BUN 20.3 mg/dL, and creatinine 0.73 mg/dL. Plain abdomi- nal film revealed no abnormal bowel gas and suspicious flu- id-filled stomach (Fig. 1A). An abdominal CT scan revealed a massive dilation of the esophagus, stomach, and duode- num, a diffuse small bowel wall thickening, a mild edematous change of the pancreas, and a mild pancreatic duct dilation (Fig. 1B-C). Acute pancreatitis due to duodenal loop ob-
struction was diagnosed. Intravenous fluid replacement and abdominal decompression with a nasogastric tube were im- mediately provided. A total of 1,000 mL of greenish semisolid material and food particles were evacuated. Soon thereafter, his abdominal pain subsided. An oral diet was started on the 3rd hospitalization day, upon which, serum amylase and li- pase levels decreased to 114 IU/L and 184 IU/L, respec- tively. On the 4th hospitalization day, he was discharged; he was then followed up for two years without relapse.
2. Case 2
A 48-year-old man presented to the emergency depart- ment with severe abdominal pain that lasted for approx- imately 4 hours. Two years prior, he had undergone a subtotal gastrectomy with Billroth I reconstruction for early gastric cancer. He denied consuming alcohol or smoking. A physical examination revealed a distended abdomen, epigastric ten- derness, and hypoactive bowel sounds. Vital signs were with- in normal limits. Intravenous fluid replacement was immedi- ately initiated, and a nasogastric tube was positioned.
Laboratory data were as follows: White blood cell count 13,130/mm3, CRP 0.13 mg/dL, AST 51 IU/L, ALT 39 IU/L, ALP 66 IU/L, GGT 31 IU/L, PT 116.5%, total bilirubin 0.77 mg/dL, BUN 11.1 mg/dL, creatinine 0.59 mg/dL, amylase 1,037 IU/L, and lipase 3,500 IU/L. Plain abdominal film re- vealed suspicious distended stomach filled with fluid without abnormal bowel gas (Fig. 2A). An abdominal CT scan revealed massive a dilation of the stomach and duodenum, as well as a diffuse swelling of the pancreas with peripancreatic fluid collection (Fig. 2B, C). Acute pancreatitis due to duodenal loop obstruction was diagnosed. Nasogastric tube decom-
Fig. 2. Plain abdomen and abdominal CT images of Case 2. (A) Suspicious distended stomach filled with fluid (asterisk) without abnormal bowel gas. (B) Axial view. A massive duodenal dilatation with a large volume of food inside (arrow). (C) Coronal view. Dilatation of the stomach (asterisk) and duodenal loop with abrupt luminal narrowing of the proximal jejunum (arrowhead). Swelling of the pancreas with peripancreatic fluid collection (arrow) is suggestive of acute pancreatitis.
Fig. 3. Plain abdomen and abdominal CT images of Case 3. (A) Linear air at right upper quadrant area (arrow), suspicious fluid-filled stomach (asterisks), and gaseous distended colonic loop and small bowels at right sided abdomen (arrowheads). (B, C) Axial views. Marked dilation of the stomach and duodenum (asterisks) and dilation of the pancreatic duct (arrow) with fluid collection (arrowhead). (D) Coronal view. A distended duodenal loop with abrupt luminal narrowing of the proximal jejunum (arrow) and fluid collection at the pancreatic tail (arrowhead). Plain abdominal film was revealed.
pression was provided, and a total of 1,500 mL of greenish semisolid material and food particles were evacuated. Soon thereafter, his abdominal pain subsided. An oral diet was started on the 3rd hospitalization day, upon which, serum amylase and lipase levels decreased to 59 IU/L and 65 IU/L, respectively. After conservative treatment, laboratory find- ings normalized, and his symptoms were resolved. On the 4th hospitalization day, he was discharged; he was then followed up for two years without relapse.
3. Case 3
A 68-year-old man presented to the emergency depart- ment with severe abdominal pain that lasted for one day.
Eleven years prior, he had undergone cholecystectomy and gastrojejunostomy for abdominal trauma. He denied con- suming alcohol or smoking. Physical examination revealed distended abdomen, epigastric tenderness, and hypoactive bowel sounds. Vital signs were within normal limits. Intrave- nous fluid replacement was immediately initiated, and a na-
sogastric tube was positioned. Laboratory data included the following: White blood cell count 8,770/mm3, CRP 4.10 mg/dL, AST 344 IU/L, ALT 185 IU/L, ALP 339 IU/L, GGT 141 IU/L, PT 94%, total bilirubin 1.08 mg/dL, BUN 7.8 mg/dL, cre- atinine 0.86 mg/dL, amylase 1,006 IU/L, and lipase 1,616 IU/L. Plain abdominal film revealed linear air at the right up- per quadrant area, suspicious fluid-filled stomach, and gas- eous distended colonic loop and small bowels at the right ab- domen (Fig. 3A). An abdominal CT scan revealed a massive distension of the stomach and duodenum, as well as a pan- creatic duct dilatation. Pneumobilia at the dilated intra- hepatic ducts was noted (Fig. 3B-D). There was no evidence of stones or tumors in the biliary tree. Acute pancreatitis due to duodenal loop obstruction was suspected. However, a bili- ary etiology could not be excluded. Nasogastric tube decom- pression and irrigation were initiated. A total of 2,000 mL of greenish semisolid material and food particles were evac- uated and his abdominal pain subsided soon thereafter. An oral diet was started on the 4th hospitalization day, upon which, serum amylase and lipase levels decreased to 29 IU/L and 21 IU/L, respectively. After conservative treatment, the laboratory findings normalized, and his symptoms were resolved. Acute pancreatitis due to duodenal loop ob- struction was finally diagnosed. On the 10th hospitalization day, he was discharged. He has since remained symp- tom-free for three years.
DISCUSSION
Acute pancreatitis caused by duodenal loop obstruction is related to ALO,11 intestinal adhesion,1 hernia,3,4 and eating disorders.5 In most cases, acute pancreatitis related to duo- denal loop obstruction developed after surgery, such as ALO as a consequence of Billroth II reconstructions after gas- trectomy and small intestinal adhesions after Roux-en-Y gas- trectomy, gastric bypass surgery, biliary diversions, internal hernias,1 and fundoplication for gastroesophageal reflux disorder.12 However, in some cases, acute pancreatitis devel- oped without prior surgery and presented as a markedly dis- tended stomach after binge eating5 or with ventral hernias.2 Closed duodenal loop triggering acute pancreatitis, called the “Pfeffer model,” was introduced in 1957.13 Closed duode- nal loop with some modifications is one of the oldest animal models for acute pancreatitis.13,14 It involves ligating the duo-
denal loop, both above and below the pancreatic duct. This model induces increased intrapancreatic duct pressure and reflux of the duodenal contents into the pancreatic duct.
Acute hemorrhagic pancreatitis developed within 24 hours, which was resolved with a release of the duodenal loop.14 Whether mortality in this model is due primarily to pan- creatitis rather than to intestinal ischemia or sepsis is debatable. To overcome this problem, an incomplete closed duodenal loop model has been proposed.15 The mechanism of acute pancreatitis in the blind duodenal loop is said to in- crease the intraluminal pressure, impeding the biliary and pancreatic flows and causing the dilatation of the biliary pan- creatic trees and the development of jaundice, cholangitis, or acute pancreatitis.
Plain abdominal films are mostly unhelpful for diagnosing closed duodenal obstruction due to the isolated distension with little gas within.5 The current cases revealed a resem- blance to the normal plain abdomen due to the little amount of gas that was contained in the fluid-filled stomach and duo- denal loop. Abdominal CT scan is an essential diagnostic tool for acute pancreatitis caused by duodenal loop obstruction.1 Distended duodenal loop, pancreatic swelling, pancreatic duct dilation, and fluid collection are all landmarks of the di- agnosis made on CT.
Ileus and acute pancreatitis are closely related. Acute ileus could be a complication caused by acute pancreatitis.
However, radiologic findings of acute pancreatitis range from unremarkable in mild disease to localized ileus of a segment of the small intestine or the colon cutoff sign in more severe diseases. Localized gastroduodenal distension rarely devel- ops despite severe pancreatitis.16 Our cases presented markedly distended stomach and duodenum with abrupt lu- minal narrowing of the proximal jejunum on the abdominal CT scans. We believed that the acute gastric dilatation was a cause rather than the result of acute pancreatitis.
Most cases of ALO can be recovered with surgical revision.11 Therefore, we recommend early detection and surgery. However, endoscopic or nasogastric tube decom- pression might be helpful in some cases of ALO. The causes of ALO are diverse: obstruction from adhesions, kinking at the anastomosis, internal hernia, stomal stenosis, malignancy, or inflammation surrounding the anastomosis.7 Among the cases of acute pancreatitis related to ALO, some with an ad- hesive band or internal hernia were resolved with endoscopic
gastrojejunostomy for abdominal trauma. Each had a dis- tended duodenal loop, possibly due to a retrograde reflux of the duodenal contents to the pancreatic duct, which is a phe- nomenon that is similar to a closed duodenal loop animal model.
This case series revealed the different features of acute pancreatitis related to ALO. Our patients had general me- chanical symptoms, such as vomiting and abdominal dis- tension; whereas ALO usually manifested as abdominal pain.
A functional blind duodenal loop and ALO revealed character- istic radiologic images; a proximal dilation of the intestine in the former and an afferent loop dilation and fluid collection in the latter. Responses to the treatment also differed; im- provement with conservative treatment in functional blind duodenal loop and surgical decompression in ALO despite conservative treatment for adhesions or internal hernias. We recommend nasogastric tube decompression to treat acute pancreatitis caused by duodenal loop obstruction.
In conclusion, acute pancreatitis that is related to duode- nal loop obstruction is rare. This case series demonstrates the clinical features and radiologic images of acute pan- creatitis related to a closed duodenal loop due to an adhesive band. Unlike the ALO, functional duodenal loop obstruction improves with conservative management and nasogastric tube decompression.
REFERENCES
1. Vettoretto N, Pettinato G, Romessis M, Bravo AF, Barozzi G, Giovanetti M. Laparoscopy in afferent loop obstruction present-
acute pancreatitis in a patient with an eating disorder: solving a chicken and egg situation. Intern Med 2011;50:571-575.
6. Frick TW, Schretzenmaier M, Hoffmann R, Largiadèr F. Obstruc- tive ileus and acute pancreatitis. Z Gastroenterol 1990;28:206- 207.
7. De Martino C, Caiazzo P, Albano M, et al. Acute afferent loop ob- struction treated by endoscopic decompression. Case report and review of literature. Ann Ital Chir 2012;83:555-558.
8. Kim HJ, Kim JW, Kim KH, et al. A case of afferent loop syndrome treated by endoscopic drainage procedure using nasogastric tube. Korean J Gastroenterol 2007;49:173-176.
9. Kitamura H, Miwa S, Nakata T, et al. Sonographic detection of vis- ceral adhesion in percutaneous drainage of afferent-loop small-intestine obstruction. J Clin Ultrasound 2000;28:133- 136.
10. Burdick JS, Garza AA, Magee DJ, Dykes C, Jeyarajah R.
Endoscopic management of afferent loop syndrome of malig- nant etiology. Gastrointest Endosc 2002;55:602-605.
11. Alawneh I. Afferent loop obstruction after gastrectomy simulat- ing acute pancreatitis. Int Surg 1980;65:415-417.
12. Inoue M, Uchida K, Otake K, Okigami M, Maji T, Kusunoki M.
Development of acute pancreatitis after Nissen fundoplication.
Pediatr Int 2015;57:e48-e49.
13. Pfeffer RB, Stasior O, Hinton JW. The clinical picture of the se- quential development of acute hemorrhagic pancreatitis in the dog. Surg Forum 1957;8:248-251.
14. Ferrie MM, O'Hare R, Joffe SN. Acute and chronic pancreatitis in the rat caused by a closed duodenal loop. Digestion 1978;18:
280-285.
15. Sugimoto M, Takada T, Yasuda H. A new experimental pan- creatitis by incomplete closed duodenal loop: the influence of pancreatic microcirculation on the development and pro- gression of induced severe pancreatitis in rats. Pancreas 2004;
28:e112-e129.
16. Davis S, Parbhoo SP, Gibson MJ. The plain abdominal radiograph in acute pancreatitis. Clin Radiol 1980;31:87-93.