대한방사선의학회지
1998 ; 38: 723- 729
Receiver Operating Characteristic Curve를 이용한 견관절 자기공명영상소견의 분석 1
황윤 준 ·서 진석· 조재 현2
목 적 : 견관절의 회전근개 파열, 전 관절순 파열, 상 관절순 파열, Hill-Sachs 병변의 자 기공명영상 소견을 등급별로 나누어 판정한 후 ROC(receiver operating characteristic) curve를 구하여 견관절에서 자기공명검 사의 유효성을 살펴보았다.
대상 및 방법 : 관절경으로 확진된 38예의 견관절 자기공명영상을 대상으로 회전근개 파 열, 전 관절순 파열, 상 관절순 파열 및 Hill-Sachs 병 변의 유무를 등급별로 나누어 관찰하였 다.
회전근개 파열은 T2강조 영상 및 양자 밀도 영상에서 근개에서 관찰되는 고신호 강도의 유무에 따라 전층의 파열부터 정상까지 5개의 군으로 나누였고, 관절순은 관절와로부터의 분리 유무, 형태상의 변화, 신호 강도의 증가 유무에 따라 전 관절순은 6개 상 관절순은 3개 의 군으로 나누었다. Hill-Sachs 병변은 상완골두의 모양 및 골수 강도의 변화에 따라 4개의 군으로 나누였고, 이들의 소견은 근골격 전문 방사선의 2명이 각기 판정한 후 ROC curve를 작성하고그하방의 면적을구하였다.
결 과 : 회 전근개 파열, 전 관절순 파열, 상 관절순 파열 및 Hill응achs 병 변의 ROC curve 하방의 면적은 각각 82.4%, 88.5%, 62.4%, 91.3% 를 차지하였다.
결 론
:
ROC curve를 이 용한 견관절 자기 공명 검 사의 정 확도는 회 전근개 파열, 전 관절순 파열, 및 Hill-Sachs 병변에서는 비교적 높게 관찰되었으나 상 관절순 파열 시에는 낮은
정확도를보였다.
견관절은 인체에서 가장 운동성이 큰 관절로써 해부학적 구 조상 불안정하고 손상 받기 쉬운 관절이다(1, 2). 견관절 질환 의 진단 방법으로는 관절경 검사가 가장 정확한 것으로 알려져 있고(3-5) 검사와 치료를 동시에 시행할 수 있다는 장점이 있 으나 침습적인 방볍이기 때문에 모든 견관절 질환이 의성되는 환자에게 시행하기는 어렵다.
자기공명영상 방법은 비침습적이며 연 조직간의 대조도가 좋 고 다평면 영상을 얻을 수 있다는 장점이 있어, 최근 들어 표면 코일(surface coi J)의 발달과 함께 견관절 질환의 평가에 많이 이용되고 있다 (6-9).
자기공명영상 방법을 이용하여 보고된 이전 연구들에서의 예 민도와 특이도는 회전근개 파열 시 각각 41-100%와
79 - 100
%(1
0- 14)
, 전 관절순 파열 시 90-100%와50-95% (7
,13
,15
,16)
, 상 관절순 파열 시 75-100%와98-100%(7
,15- 17)
, HiJl-Sachs 병변시 76-97%와54 -91%(7
,18 )
등으로 보고자마다 다양한 결과를 보이고 있다. 이는 사용된 자기공명l 연세대학교 의과대학 진단방사선과학교실 2아주대학교 의과대학 진단방사선과학교실
이 논문은 1997년 9월 4일 접수하여 1998년 2월 4일에 채택되었음.
낌
영상의 적용 방법 (sequence, slice thickness) 의 차이, 손상 부 위의 면적 및 위치, 퇴행성 변화의 동반 유무, magic angle 현 상 등 (19) 의 자기공명영상 7냉물, 그리고 확진 방법의 차이 등 에 기인 한다고볼수있다.
ROC(receiver-operating characteristic) curve는 영상 진 단 방법의 정확도를객관적으로추측할수있는방법 중하나로 알려져 있으며
(20-22 )
, 이를 이용하여 견관절 질환 중 흔하게 관찰되는 회전근개 파열, 전 관절순 파열, 상 관절순 파열,Hill-Sachs 병변의 자기 공명 영상의 정확도를 알아 보았다.
대상및방법
견관절 자기공명영상 검사 후 관절경을 시행하여 확진된
38
명의 환자를 대상으로 하였다. 환자의 나이는 17세에서 62세까 지 였고(평균 34.7세 ), 남자가 31명, 여자가 7명, 우측이 25예,좌측이 13예였다. 환자들의 주된 호소는 습관성 탈구가 17예였 고 통증이나 운동 장애를 보이는 경우가 21예였다.
관절경을 시행하였던 총 38명의 환자 중 기록이 미비했던 경 우를 제외하고 34명의 환자에서 회전근개의 이상 여부를 확인
횡윤준 오I
: Receiver Operating Characteristic
Curve톨 이용한 견관절 자기공명영상 소견의 분석할 수 있었고, 이중 파열이 17예 (전층 파열[full
thickness tearJ
8예, 부분 파열 [partialthickness tear J
9예) , 정상이17
예(퇴행성 변화 l예 포함 )였다. 전 관절순은 총 36예에서 확인 이 되었고, 파열이 17예, 정상이 19예(퇴행성 변화 1예 포함)였 다. 상 관절순과
Hill
-Sachs
병변은 38예 모두에서 확인 되었으 며, 상 관절순의 경우 파열이 10예 정상이 28예였고Hill
-Sachs
병변은 13예에서 존재했고 25예에서는 정상이였다.자기공명영상은 1.
5 Tesla
초전도형 자기 공명 영상 기기(Signa
,GE medical systems
,Milwaukee
, USA) 와 어깨코일(shoulder
coil)을 사용하여multiplanar gradient recalled echo(MPGR
,TR /TE
,500/ 10
,500/25
,flip angle 30')
축상 영상을 얻고, 스핀 에코 (TR/ TE
,2000/20
,2000/70)
사관상 및 사시상 영상을 얻었다.ROC
curve의 작성을 위 해 견관절 질환에서 흔히 발견되는 회전근개 파열, 전 관절순 파열, 상 관절순 파열,Hill
-Sachs
병 변의 자기 공명 영상소견을등급별로분류하였다.회전근개 파 열은총다섯 군으로나누었고 T2 강조영상에서 회전 근개 전 체 두께에 걸쳐 신호강도의 증가가나타나면 ++군,일부분에 서만 관찰되면 +군, 그리고 신호 강도의 증가 여부가 불명확한 경우는 O군으로 나누었고, 양자 밀도 영상에서는 신호 강도가 증가 하였지만T2
강조 영상에서는 증가하지 않은 경우는 군,형태의 이상없이 균질한저 신호강도로관찰될 때는 - 군으로분류하였다.전 관절순 파열은 총 여섯 군으로 나누었다. 관절순이 관찰되 지 않거나 관절와 (glenoid) 로 부터 분리되어 있을 때는
+++
군으로, 형태의 변형 (불규칙한 모양, 분절, 크기의 감소가 있으 면서 관절순의 표면이 불규칙한 경우)이나 관절순 내에 열
(cleft) 이 관찰되면 ++군으로, 그리고 삼각형의 모양을 유지 하지만 관절와관절순 경계부 (glenolabral junction) 에서 관찰 되는선형의 중간신호강도가관절순의 표면까지 나와있는경 우는 +군으로 분류하였다. 관절순의 크기는 감소하였지만 관 절순의 표면이 편평한 경우는 O군으로, 암각형의 모양을 유지 하면서 관절순 내에 증가된 신호가 관찰되고 이것이 관절순의 표면까지 닿아 있으면 -군, 닿아 있지 않거나 균질한 저 신호 강도의 관절순이 관찰될 때는 군으로 분류하였다.
상 관절순 파열은 총 세 개의 군으로 나누었고 관절순이 관절 와로부터 분리되어 있거나 이두끈 관절순 복합체 (biceps
labral
complex) 의 위 또는 아래 변에서 불규칙한 신호 강도의 증가가 관찰되면 ++군, 관절순의 모서리가 둔탁하고 주위의 신호 강도가 증가된 경우는 +군, 그리고 삼각형의 모양을 유지 하면서 정상 저 신호 강도의 이두근건 (biceps tendon) 과 함쳐 지는 경우는 -군으로 나누었다.Hill응achs 병 변은 총 네 개의 군으로 나누었고 요구돌기
(coracoid
process) 가 관찰되는 높이 이상의 횡단 영상에서 상 완골두후외측부위에 뚜렷한손상이 보이면 +++군,불규칙 하게 편평한변을보이면서 주위의 골수신호강도의 변화가있 으면 ++군, 골수 변화가 없으면 +군으로 나누었고 원형 또는 타원형으로관찰되면 -군으로나누였다.정 해진 각 질환의 등급별로 근 골격 방사선 전문의 2명이 판
724
독하였다. 판독은 환자의 임상 병력을 모르는 상태에서 진행하 였고, 정해놓은 등급별 소견 이외의 진단에 도움이 될 수 있는 이차척인 소견들은 무시하였다.
판독 후 각 등급별로 진양성률(true
positive fraction=
true posi ti ve / true posi ti ve + false negati
ve) 과 가양성률(false positive fraction=false positive/true negative + false
positive) 을 구하여 두 관찰자의 평균값을 얻은 후ROC
curve를 구하였다.
ROC
curve는nonparametric smoothing
technique을 사용하여
curve
fitting하였고, 방법으로는Gaussian
함수를 사용한Kernel
method를 응용하였다. 검 사 의 정확도를 간접적으로 반영해 주는 curve아래의 면적 (Az) 은 curve를 얻은 후 적분하여 구하였다.회전근개의 전층 파열(++군)과 부분 파열(+군)의 각각의 예민도 (true
positive/true positive + false negative) ,
특이 도 (truenegative/true negative + false positive)
, 정확도(true positive + true negative /
all) 를 구하였다.vers
Table
1.Data of shoulder MRI interpreted by Two Obser-
Observer A Observer
BMR+
(Arthroscopy
+ /- )
MR+
(Arthroscopy
+/- )
Rotator Cu ff( n = 34) + +
+
0
Anterior Labrum(n=36) + + + + +
+
0
쩌
n뼈
배m
L빡 +
+
F3
+
Hi
ll-Sachs lesion(n=38) + + +
++
+
9(9/1이
18(14/4) 9(6/3) 3(1/2) 2( 1/1) 2(0/2) 6(0/6) 7(1/6) 8(1 /7) 4(1/3)
9(9/이 1
8(7/1 ) 6(5/1) 4( 2/2) 1(0/1)
0(0/1이1(0/1)
2(2/1이5(1/4)
2(2/1이l 여 2/1 2)
20(4 /1 6)
3(2/1) 3(2 /1) 11(3/8)
5(2β)2 4( 5/19) 30(6/24)
8(8/1이
8(7/1)
0(0/1이
2(1 /1) 5(3/2) 2(1 /1) 25(2/23) 26(4/22) MR + : number of patients showing positive finding in MRI
Arthroscopy + / - : nurnber of patients showing positive/
negative finding in arthroscopy
대한밤시선의학회지
'998 ; 38 : 723 - 729
결 과
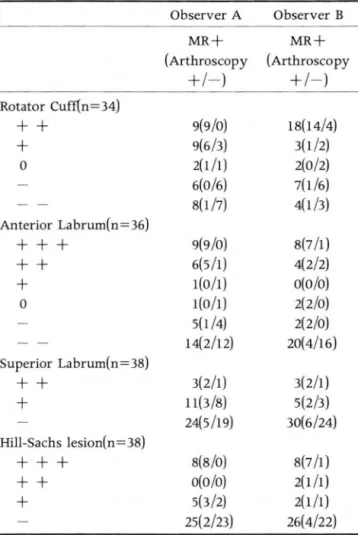
두명의 판독의에 의하여 회전근개 파열,전 관절순파열,상 관절순 파열 및 Hill-Sachs 병 변에서 각 등급별로 판독된 환자 의 수와 실제 관절경의 결과는 Table 1과 같다.
각 질환별 ROC curve아래의 면적 (Az) 은 회전근개 파열의 경우
82
.4%, 전 관절순 파열88.5%
, 상 관절순 파열62
.4%,Hill-Sachs 병변 91.3% 로 측정되어 회전근개 파열, 전 관절순
파열, Hill-Sachs 병변의 자기 공명 영상의 정확도는 비교적 높
게 측정되었으나, 상 관절순 파열 시에는 낮은 정확도를 보였다 (Fig. 1).
회전근개 파열에 있어서 전층파열로생각했던 ++군과부 분 파열로 생각 했던 +군을 따로 분류하여 각 질환의 예민도,
특이도, 정확도를 구하였고 전층 파열의 경우는 각각
93.7%
,75.0%
,85
.4 %였고, 부분 파열의 경우는 각각33.8%
,88.0%
, 60.7%였으며, 회전근개 파열 전체의 경우는 각각88.2%
,74
.4%, 81.3%였다.
고 찰
들이 소개되고 있고, 새로운 방법이 기존의 것에 비하여 어느 정도 유용한가를 결정하기 위하여 진단 방법의 정확도를 객관 적으로 평가하려는 노력이 늘고 있다. ROC curve는 뚜렷한 비 정상 소견이 관찰되는 경우, 비정상 소견이 의심되는 경우, 정 상과 비정상 간의 판단이 모호한 경우, 뚜렷하지는 않으나 정상 일 가능성이 높은 경우, 확실히 정상인 경우 등으로 진단 기준 을 세분화 시킨 후 각 경우 마다 예민도와 특이도를 측정하여 Y축에 진양성률(예빈도), X축에 가양성률(1-특이도)로 구성 된 도표를 작성함으로써 이루어 진다. curve 아래의 면적은 정 확도를 간접적으로 반영한다고 알려져 있으며, 관찰자의 판단 결과를 연속화 시킴으로써 소견을 단순히 정상 혹은 비정상으 로 판정했을 경우 생기는 관찰자 간의 주관적인 판단 오~~를 줄 여 주고객관화시킬수있다.
견관절의 가장효과적인 영상진단방법의 결정에 있어 논란 이 있어 왔으나 (6, 23-28) , 자기 공명영상은 많은 비용이 든다 는 단점에도 불구하고 비침습적이며 연 조직간의 대조도가 좋 아 견관절 질환시 가장 유용한 영상 진단 방법으로 알려져 있다
(6
,9
,11
,1 8
,29).
견관절 질환중에는 회전근개 파열을 포함}는 감입 증후군 (impingement syndrome) 과 습관성 탈구에 의한 관절순 질환 이 많다. 현재 회전근개 질환에 있어서 Neer가 발표한 이론이 기술적인 발전에 힘입어 많은 종류의 영상 진단 기기나 방법 널리 받아들여지고 있고(3이, 그는 극상근건 (supraspinatus
R otator Cuff
‘," ’
‘’
1/ι· •
/
82.4%
‘,0
1/
‘-
- 1.1 0.2
...
u 1.1’
l찌")
A
Supe끼 or Labrum
‘ '-f ___ -
0.2 OA 0.1 0.1
’
a어Rη
C
Anterior Labrum
‘φl / / - - -
‘ =-1 I .: .. •
아1 /
88.5%훌앤펀
B
D
‘~ A_
t-- ...
0.2 O.A OA o.aP(FP)
Hill-Sach ’ s lesion
g3환 ‘
1.2
... ...
1.1에FI'’
725 -
1.0
’
lFig. 1. ROC curves presenting diag- nostic accuracies of rotator cuff tear(A), anterior labral tear(B), su- perior labral tear (C) and Hill-Sachs lesion(O).
p(TP) : true positive fraction p(FP) : false positive fraction
횡윤준 오I
: Receiver Operating Characteristic
Curve를 이용한 견관칠 자기공밍영삼 소견의 분석tendon) 이 상완골두의 대결절과 견봉 (acromion arch) 사이에 서 마찰을 일으킴으로써 대부분의 극상근 질환이 발생한다고 설명하고 있으며, 회전근개의 손상을 부종과 출혈이 오는 시기,
섬유화와 건염이 오는 시기, 그리고 골편 형성과 근개의 파열이 오는 시기로 나누었으나, 각 시기는 연속적이며 중복되어 나타 나게 펀다. 여기에 갈고리 (hook) 모양의 견봉 (31, 32) 과 해부학 적으로 저 혈류 분포 지역의 존재 (33,34) 등이 회전 근개의 파 열을 띨으키는데 관여하는 것으로 알려져 있다.
회진근개 파열에 있어 본 연구는 다른 보고자들과 비슷한
(10 -14, 35)
전층 파열 시85.4
%, 부분 파열 시60.7
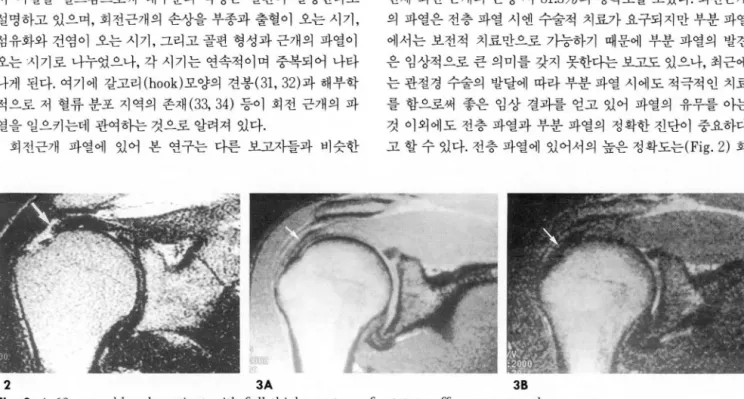
%, 그리고 전체 회전 근개의 손상 시 81.3%의 정확도를 보였다. 회전근개 의 파열은 전층 파열 시엔 수술적 치료가 요구되지만 부분 파열 에서는 보전적 치료만으로 가능하기 때문에 부분 파열의 발견 은 임상적으로 큰 의미를 갖지 못한다는 보고도 있으나, 최근에 는 관절경 수술의 발달에 따라 부분 파열 시에도 적극적인 치료 를 함으로써 좋은 임상 결과를 얻고 있어 파열의 유무를 아는 것 이외에도 전층 파열과 부분 파열의 정확한 진단이 중요하다 고 할 수 있다. 전층 파열에 있어서의 높은 정확도는(Fig.2) 회2
3A 38
Fig. 2. A
60-year-이dmale patient with full thickness tear of rotator cuff proven at arthroscopy
T2- weighted image shows complete interruption and retraction of rotator cuff, and two observers interpreted this film as grade + +.
Fig. 3. A 30-year-old male patient with a partial thickness tear of rotator cuff proven at arthroscoy. Proton density weighted image (A) shows mild increased signal intensity (arrow) on rotator cuff but does not show in T2-weighted im- age(arrow)(8). This was interpreted as Grade
- -by one observer, while it was considered as grade - by anothe
r.4
s
A
B
π ω
Fig.
4.A 27-year-old male patient with normal labrum at arthroscopy
Tl-weighted axial image shows cleft (arrow) at anterior labrum
.Two observers read this film Grade 0 and + +, respectively.
Fig.
S.A 25-year-old male patient with minimal Hill-Sachs lesion seen at arthroscopy
Two observers read this film nor- mal as Grade
Fig. 6. A 53-year-old female patient
with grade 3 SLAP injury found at
arthroscopy. Proton density weig
hted (A) and T2-weighted images
(8) show triangular shaped superior
labrum (arrow) without definite vis-
ible defect which was considered as
a grade
-대한밤시선의학호IXI 1998; 38: 723-729
전근개 질환시의 자기 공명 영상적용에 있어 의미 있다할수 있겠으나 부분 파열 시에는 높지 않은 결과를 보였고(Fig. 3), 이는 자기 공명 영상의 공간 분해능상 인식할 수 없었던 작은 면적의 파열 부위 또는표면에 국한되어 있는병변에 의한것일 것으로생각된다.
견관절은 인체에서 가장 운동성이 큰 관절이지만 상완골두에 비하여 관절와는 접촉면이 얄기 때문에 불안정한 구조를 이루 게 된다(1). 따라서 견관절 안정성의 유지에는 상완골두와 관 절와같은 구조 이외에 주위의 연조직들이 관여하게 되고 이중 관절순, 관절와상완골 인대 (glenohumeral ligament), 회전근 개 등이 중요한 역할을 하게 되며 이들은 서로 복합적으로 견관 절의 안정성 유지에 기여하게 된다 (36).
전방 탈구 시의 자기 공명 영상 소견은 관절순의 파열 이외에 하부 관절와상완골 인대 (inferior glenohumeralligament) 및 견갑하근과건의 손상에 의하여 신호강도의 변화및 퇴축,근 육의 위축 등이 관찰되고, Bankart 병변이나 Hill-Sachs 병변 과 같은 골격 구조의 손상이 관찰되게 된다. 전 관절순의 정상 자기공명영상 소견은 모든 조건의 영상에서 삼각형 모양의 균 질한 저 신호 강도를 보이게 되며, 파열 시에는 관절순이 관절 와로부터 분리되거나 모서리가 뭉룩해지고 관절순 내부의 신호 강도의 변화가 오게 되는 것으로 알려져 있으나 지금까지의 보 고에 의하면 증상이 없거나 수술로 정상임이 확인된 대상 군에 서도 다%댁} 모양의 정상 변이가 관찰되고, 퇴행성 변화를 동반 하게 되면 관절순 내의 신호 강도에 변화가 요게 되어 진단에 오류를 벙할 수 있다 (Fig. 4) (37, 38). 본 연구에서는 전 관절순 의 파열 시 88.5%의 정 확도를 보였다.
Hill응achs 병변은 그 자체로써 치료 방침의 결정에 중요한 영향을 미치지는 않으나 견관절 탈구의 다른 소견이 명확치 않 을 때 주위 조직 손상 유무를 예측하는데 도움을 주게 된다. 진 단은 상완골두 상부 후 외측 부위의 원형 모양이 소실되는 것을 관찰함으로써 이루어지며, 본 연구에서는 91.5%의 정확도를 보였다 (Fig. 5). 전 관절순 파열과 Hill-Sachs 병변에서의 결과 는 환자의 병력이나 주위 조직의 변화를 무시하고 얻은 결과이 기 때문에 실제로 임상 적용 시에는 더 높은 정확도를 얻을 수 있을것으로생각된다.
최근 견관절 질환에 관절경의 적용이 늘어 나면서 이두근건 과 이두근관절순 복합체를 포함하는 상 관절순의 손상이 보고 되고 있으며 젊은 운동 선수 등에서 발생송F는 빈도가 높아 중요 성을 띠고 있다 (4이. SLAP(superior labrum
,
anterior and posterior) lesion이라 불리우는 이러한 상 관절순의 손상은 손 상 정도와 부위에 따라 4가지 군으로 나뷔어 지고, 각군별CT
및 자기 공명 영상 소견이 보고되어지고 있으나 (7, 18), 상 관 절순은 전 관절순에 비하여 관절와에 대하여 정상적으로 좀 더 느슨하게 부착이 되어 있어 증상이 없는사람에서도어느정도 의 분리가 관찰될 수 있고 더욱이 상 관절순을 제일 잘 관찰할 수 있는 사관상 영상에서 일반적인
3mm
내외의 두께 절편으 로 촬영 시 상 관절순의 해부학적 구조를 명확히 관찰할 수 있 는 영상이 제한되어 주위의 여러 구조들이 서로 결합을 이루며 만들어낸 공간들이 관절순 파열의 유사한 양상을 보여 실제 판낀
독 시에 병변의 정확한 진단이 쉽지 않고 (Fig. 6), 본 연구에서 도 정 확도는 상당히 낮았다.
결론적으로 견관절 질환의 자기 공명 영상 시 회전근개 파열,
전 관절순 파열, Hill-Sachs 병변에서는 높은 정확도를 보여 임 상적으로 유용할 것으로 생각되나 상 관절순의 파열 시에는 진 단에 어려움이 있었다.이러한결과는환자의 병력 및 이차적인 소견들을 염두에 두고 판독한다면 더 좋은 결과를 얻을 수 있을 것으로 생각되며 다양한 자기 공명 영상 기법의 발달에 따라 진 단의 정확도는 높아질 것으로 생각된다.
참 고 문 헌
1. Rothman RH, Marvel JP Jr, Heppenstall RB. Anatomic considerations in the glenohumeral joint. Orthop C/in North Am 1975; 6: 341-352
2. Bonafede RP, Bennet RM. Shoulder pain: guidelines to diag- nosis and management. Postgrad Med 1987; 82 ‘ 185-193 3. Gachter A, Seelig W. Arthroscopy of the shoulder‘ Arthroscopy
1982; 8 : 89-97
4. Mok DW, Fogg AJB, Hokan R, et al. The diagnostic value of arthroscopy in glenohumeral instability. J Bone Joint SurgfBrJ 1990 ; 72 : 698-700
5. Rockwood CA. Shoulder arthroscopy. J Bone Joint SurgfAmJ 1988; 70 : 639-640
6. Stiles RG, Otte MT. Imaging of the shoulder. Radi%gy 1993;
188: 603-613
7. Jahnke AH Jr, Petersen SA, Neumann C, et 허‘ A prospective comparison of computerized arthrotomography with MR imaging of the glenohumeral joint. Am J Sports Med 1992; 20:
695-701
8. Habibian A, Stauffer A, Resnick D, et al. Comparison of con- ventional and computed arthrotomography with MR imaging in the evaluation of the shoulder. J Comput Assist Tomogr 1989; 13: 968-975
9. Holt RG, Helms CA, Steinbach L, et al. Magnetic resonance imaging of the shoulder: rationale and current application. Ske/- eta/ Radio/ 1990; 19: 5-14
10. Hodler J, Kursunoglu-Brahme S, Snyder S, et al. Rotator cuff disease: assessment with MR arthrography versus standard MR imaging in 36 patients with arthroscopic confirmation. Radi-
0/0양 1992; 182: 431-436
11. Burl
‘
DL, Karasick D, Kurtz AB, et al. Rotator cuff tears: pro- spective comparison of MR imaging with arthrography, sonography, and surgery. AJR 1989; 153: 87-9212. Evancho AM, Stieles RG, Fajman W A,et al. MR imaging diag nosis of rota tor cuff tears. AJ R 1988; 151 : 751-754
13. Iannoti JP, Zlatkin MB, Esterhai JL, et al. Magnetic resonance imaging of shoulder. J Bone Joint Surgf AmJ 1991 ; 73 : 17-29 14. Zlatkin MB, Iannoti JP, Roberts MC, et al. Rotator cuff tears:
Diagnostic performance of MR imaging. Radi%gy 1989; 1 7 2 : 223-229
15. Legan JM, Burkhard TK, Goff II WB, et al. Rotator cuff lesion: Signal pattern at MR imaging Radi%gy 1990; 1 77: 817-823 16. Gusmer PB, Potter HG, Schatz JA, et al. Labral injuries: Accu
racy of detection with unenhanced MR imaging of the shoulder. Radi%gy 1996; 200: 519-524
17. Monu JUV, Pope TL, Chabon SJ, Vanarthos W J. MR diagnosis of superior labral anterior posterior injuries of the glenoid labrum: Value of routine imaging without intraarticular injec-
횡윤준 오I
:
Receiver Operating Characteristic Curve톨 이용한 견관절 자기공명영상 소견의 분석tion of contrast material. AJR 1994; 163: 1425-1429
18. Workman TL, Burkhard TK, Resnick D, et al. Hill-Sachs lesion:
Comparison of detection with MR imaging, radiography, and arthroscopy. Radiology 1992; 185: 847-852
19. Erickson SJ, Cox IH, Hde JS, Carrera GF, Strandt JA, Estkowski LD. Effect of tendon orientation on MR imaging sig- nal intensity: A manifestation of the ’magic angle' phenom- enon. Radiology 1991; 181: 389-392
20. Vining DJ, Gladish GW, Receiver operating characteristic curves: a basic understanding. RadioGraphics 1992; 12 ’ 1147 1154
21. Hanley JA. Receiver operating characteristic (ROC) method ology: the state of the art. Crit Rev Diagn Imaging 1989; 29 : 307-335
22. Hanley JA, Mcneil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982;
143: 29-36
23. Resnick D, Shoulder arthrography. Radiol Clin North Am 1981;
19: 243-253
24. Goldman AB, Ghelman B. The double contrast shoulder arthrogram. Radiology 1978; 127: 655-663
25. Haynor DR, Shuman WP. Double contrast CT arthrography of the glenoid labrum and shoulder girdle. RadioGraphics 1984; 4:
411-421
26. Shuman WP, Kilcoyne RF, Matsen FA, et al. Double contrast computed tomography of the glenoid labrum‘ AJR 1983; 141 : 581-584
27. Middleton WD. Sonographic detection and quantification of ro tator cufftears. AJR 1993;160:109-110
28. Mack LA. Matsen FA, Kilcoyne RF, et al. US evaluation of the rotator cuff‘ Radiology 1985; 157: 205-209
29. Kieft GJ, Bloem JL. Rozing PM, Obermann WR. MR imaging of recurrent anterior dislocation of the shoulder: Comparison with CT arthrography. AJR 1988; 150: 1083-1087
30. Neer CS. Impingement lesions. Clin 0π hop 1983; 173: 70-77 31. Epstein RE, Schweitzer ME, Frieman BG, Fenlin JM Jr, Mitchel
DG. Hooked acromion: prevalence on MR images of painful shoulder. Radiology 1993; 187: 479-481
32. Edelson JG. The 'hooked’ acromion revisited. J Bone Joint Surg [Br] 1995; 77: 284-287
33. Moseley HF, Colsiw 1. The arterial pattern of the rotator cuff of the shoulder. J Bone Joint Surg[Br] 1963; 45: 780-789
34. Rathbun JB, MacNab 1. The microvascular pattern of the ro tator cuff. J Bone Joint Surg[Br] 1970;52:540-553
35. Traughter PD, Goodwin TE. Shoulder MRI: Arthoscopic corre lation with emphasis on partial tears. J Comput Assist Tomogn 1992; 16: 129-133
36. Deutsch AL, Resnick D, Mink JH,et al. Computed and conven- tional arthrotomography of the glenohumeral joint: Normal anatomy and clinical experience. Radiology 1984; 153: 603-609 37. Loredo R, Longo C. Salonen D, et al. Glenoid labrum ‘ MR
imaging with histologic correlation. Radiology 1995; 196: 33-41 38. Longo C Loredo R, Yu J, et al. MRI of the glenoid labrum with
gross anatomic correlation. J Comput Assist Tomogn 1996; 20 487-498
39. Hodler J, Kursunoglu-Brahme S, Flannigan B, Snyder SJ, Karzel RP, Resnick D. Injuries of superior portion of glenoid labrum involving the insertion of the biceps tendon: MR imaging findings in nine case. AJR 1992; 159: 565-568
40. Hunter JC Baltz DJ, Escobedo EM. SLAP lesions of the glenoid labrum: CT arthrographic and arthrographic correlation. Radi- ology 1992; 184: 513-518
얘
@대한빙시선의학호IXI
1998; 38: 723- 729
J Korean
Radi이Soc 1998; 38 : 723- 729
Analysis of Shoulder MR Imaging Using Receiver Operating Characteristic Curve
1Yoon-Joon Hwang , M.D. , Jin-Suck Suh , M.D. , Jae-Hyun Cho , M.D.
21 Department Of Diagnostic Radiology, Yonsei University College Of Medicine 2Department Of Diagnostic radiology , Ajou University College Of Medicine
Purpose: To assess the utility of shoulder MRI by using ROC (receiver operating characteristic) curve in the evaluation of rotator cuff tear , anterior labral tear , superior labral tear and Hill-Sachs lesion.
Materials and Methods: We evaluated 38 arthroscopically confirmed patients who had under- gone shoulder MR
I.According to the signal intensity of the rotator cuf f, as seen on T2 and proton density imaging , a five-stage grading system was devised. Labral tears were graded according to the separation of the labium; this was based on gleaned , morphologic and signal intensity changes of the labrum: six grades of anterior labral tear and three grades of superior labral tea
r.Hill-Sachs lesion was also classified into four grades according to morphologic and signal changes of the hu- meral head. These findings were reviewed by two musculoskeletal radiologists and ROC curves and areas under the curve (Az) was obtained
Results: The ratio of area under the curve of rotator cuff tear , anterior labral tear , superior labral tear and Hill-Sachs lesion were 82 .4%, 88.5% , 62 .4% and 9
1.3% , respectively.
Conclusion: The Accuracy of shoulder MRI using ROC curve was relatively high in rotator cuff tear , anterior labral tear and Hill-Sachs lesion , but low in superior labral tear.
Index words: Shoulder , abnormalities Shoulder ,
~‘RIReceiver operating characteristic curve (ROC)
Address reprint requests to: Jin Suck Suh , M.D. , Department of Diagnostic Radiology , Yonsei University Medical College
ij 134
, Shinchon-Dong , Seodaemun-Gu , SeouL
120-752Korea.
Tel. 82-2-361-5837 Fax. 82-2-393-3035
m
국제 학술대회 일정표[ 1 J
• 10th Int. Symposium on Radionuclides in Nephro-Urology (1998/05/14-16) venue: Copenhagen, Denmark.
contact: Henrik S. Thomsen M.D., Herlev Hosp., Radiology D., Herlev Ringvej 75, DK-2730 Herlev, Oenmark (tel :45 - 44-535300; fax: 45-42 -910480)
• 85th Congress & Annual Meeting of the Swiss Society for Medical Radiology (1998/05/14- 16) venue: Solothurn, Switzerland
contact: Prof. Or. med. P. Probst, Secr. Gen. SGMR/SSRM, IMR, Buergerspital, CH-4500 Solothurn, Switzerland.
(teI:41-32-6274Ioo; fax:41-32-6274125)
• Internal Derangements of Joints: MR Imaging (1998/05/15 -17)
venue: The Plaza Hotel New Y ork, NY, USA contact: Ryals & Ass., Inc., P.O. Box 1925,
Roswell, GA 30077 -1925, USA
(tel: 1-770-6419773; fax: 1-770-5529859)
• XVI Symposium Neuroradiologicum of the
WFNRS/36th Annual Meeting ASNR(1998/05/15- 21) venue: Pennsylvania Conv. Center Philadelphia, Penns., USA.
contact: Mr. James Gantenberg or, Mr. Timothy Moses, WFNRS, 2210 Midwest Road, Ste 207, Oak Brook, IL 60521, USA.
(tel: 1 - 630 - 5740220; fax: 1 -630 - 5740661)
• 380 Congresso Nazionale Dell' Associazione Italiana di Radiologia Medica (1998/05/16 - 20)
venue: Fiera di Milano Milan, Italy contact: SIRκι
Via della Signora 2, 1-20122 Milano, Italy (tel: 39 - 2 - 76006124; fax: 39 -2 -76006108)
• 36th Annual Meeting of the American Society of Neuroradiology (1998/05/17 -21)
venue ‘ Pennsylvania Conv. Ctr. Philade\phia, PA, USA. contact: Tim Moses or, Lora Tannehill, ASNR,
2210 Midwest Road, Ste 207, Oak Brook, IL 60521, USA.
(tel: 1-630-5740220; fax: 1-630-5740661)
• Practical Training in Interventional Radiology Using the Pig as a Model (1998/05/18-22)
venue ‘ Liège, Belgium
contact: Dr. A. Lunderquist, M.O.,
Svenska vagen 48, S-226 39 Lund, Sweden (tel:46 -46 - 2115656; fax: 46 -46 -2115656)
• 35th Annual Congress European Society of Paediat- ric Radiology (1998/05/18- 23)
venue: Rodos Palace Hotel Rodos Island, Greece contact: Dr. V. Theodoropoulos, c/o Amphitrion,
2, Karageorgi Servias Str, 105 62 A thens, Greece (tel : 30 -1 - 3228884 -7; fax: 30 -1 - 3230370)
• The Conference on Head and Neck Radiology and Neuroradiology (1998/05/20 -21)
venue: Odessa Medical University Odessa, Ukraine contact: Dr. V.T. Ojomin,
Lomonosova str. 33/43, Kiev, Ukraine 252022 (tel: 380-44-2637610; fax: 380-44 -2660108)
• 79th Deutscher Roentgenkongress (1998/05/20-23) venue ‘ Rhein-Main-Hallen Wiesbaden, Germany‘
contact: Beate v. Waldthausen, Deutsche Roentgenges. e. V., Postfach 1336
,
D-61283 Bad Homburg,
Germany (tel:49 - 6172 -488585; fax:49 -6172 -488587)• VII International & Interdisciplinary Symposium Stents & Grafts (1998/05/20-23)
venue ‘ Nara, Japan
contact: Or. D. Liermann, M.D., Hosp. J.W. Goethe Univ‘’
Hs23A, Thedor-Stern-Kai 7, 0-60590 Frankfurt am Main, Germany
(tel:49 -69 -63017277; fax‘49 -69 -630\7259)
• European Course in Neuroradiology-Spine and Spinal Cord (1998/05/22 - 27)
venue: Convento San Domenico Bologna, Italy contact: Dr. P.F. Bistoletti, c/o MGR Congressi, Via Servio Tullio 4, 1-20123 Milano, Italy.
(tel: 39 - 2 -43007247; fax: 39 -2 -43007247)
• National Congress of the Italian Society of Radiology (SIRM) (1998/05/23-27) venue: Fiera di κ1ilano κ1ilano, Italy
contact: Luciana Venturini, Univ. Napoli Federico II, Via Sergio Pansini 5., Pad. 16-180131 Napoli, Italy.
(teI:39-81-5467826; fax:39-81-5461703)
• Conference of the European Soc. of Gastro-Intesti-
nal & Abdominal Radiology (1998/05/24-28)
venue: Hotel don Carlos Marbella, Spain
contact: Prof. C. Pedrosa, Hosp. Univ. of San Carlos, C 7 Martin Lagos S/N, 28040 Madrid, Spain.
(tel : 34 - 1 -3303589; fax: 34 -1 - 3303257)
• CNR ’98-Congresso Nacional De Radiologia (1998/05/27 -30)
venue: Lisbon, Portugal
contact: Portuguese Society of, Radiology & Nuclear Med., Av. Elias Garcia 123-7dto, P-1050 Lisboa, Portugal (tel:351-1-7970530; fax:351-1-7969830)
• NICER China Series: Pediatric Radiology and Neuroradiology (1998/05/29 -01)
venue: Beijing, China.
contact: The NICER Institute, att. Kristin Sandvik, Postboks 4462 Torshov, N-0401 Oslo, Norway (tel :47 -22 -891867; fax: 47 -22 -891210)
n v
η
제공:대한방사선의학회 국제협력위원회