교신저자: 황선욱, 경기도 의정부시 금오동 65-1, 480-717, 가톨릭대학교 의정부성모병원 가정의학과 Tel: 031-820-3179, Fax: 031-847-3941, E-mail: [email protected]
남성 골다공증의 특징과 치료
황 선 욱
가톨릭대학교 의과대학 가정의학교실
Characteristics and Treatment of Osteoporosis in Men
Sun-Wook Hwang, M.D.
Department of Family Medicine, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea
서 론
골다공증으로 고통받는 남성의 수는 정확히 알려져 있지 않다. 그리고 골밀도 검사와 골절위험의 관계도 여성처럼 많은 연구가 되어있지 않다.
1)그러나 나이에 따라 남성도 여성과 마찬가지로 골절 위험이 증가하 는데 여성에 비하면 급격한 골절 위험이 10년정도 늦게 나타난다.
2)Schuitt 등
3)은 55세 이상의 남성에서 골밀도와 고관절 골절, 비척추 골절의 상관관계를 조사하였는데 여성과 비슷하다고 하였다. 척추골절률은 55∼59세 사이에는 여성과 비슷하지만 그 이후에는 여성보다는 상대적으로 골절률이 낮아져 75세에는 남 성의 13.6%, 여성의 29.3%가 척추골절을 가진다.
4)그리고 Chang 등
5)은 약 50%의 고관절 골절이 80세 이전에 발생하며 미국, 북유럽에서는 약 20∼25%의 고관절 골절이 남성에서 발생한다고 하였으며
6)50세 이상의 20∼25% 정도가 골다공증과 관련된 골절을 겪고 있다고 하였다.
7)중요한 사실은 고관절 골절에 의한 이환율과 사망률은 남성이 여성보다 높고 75세 이후 고관절 골절에 의한 치명률은 20.7%로 여성의 7.5%에 비하여 훨씬 높다는 사실이다. 그리고 1990년에는 남성 고관절 골절 발생자수가 50만명이었던 것이 2025년에는 116만명으로 증가할 것으로 예측되고 있다.
8)척추 골절도 과거 에는 남성에 비하여 여성이 10배 많았는데 최근에는 여성의 절반수준으로 높게 나타나고 있다.
9)그리고 예기치 못한 척추 골절은 특히 50∼60대의 남성에서 더 흔하며 반면 손목 골절은 남성에게 흔하지 않고 나이에 따라 증가하지 않는다.
10,11)본 론
1. 병태생리, 원인
남성은 성선기능저하증이나 전립선암 등 특별한 경우를 제외하고는 여성과 같이 성호르몬 손실이 적기
때문에 중년에는 골 소실이 천천히 진행된다. 남성은 폐경처럼 갑작스런 성선기능의 중지가 나타나지 않지
Table 1. Secondary cause of osteoporosis in men Secondary osteoporosis
• Alcoholism
• Hormonal disorders Hypogonadism Cushing's syndrome Hyperthyroism
Hyperparathyroism (1
oand 2
o)
• Gastrointestinal disorder Malabsorption syndromes
Inflammatory bowel disease, gluten entheropathy Primary biliary cirrhosis
Post gastrectomy
• Hypercalciuria
• Chronic obstructive pulmonary disease
• Transplantation osteoporosis
• Neuromuscular disorder
• Systemic illnesses Rheumatoid arthritis Multiple myeloma Other malignancies Mastocytosis
• Medication/drug-related Gllucocorticoids Anticonvulsants Thyroid hormone
Chemotherapeutics
만 서서히 연령과 관련된 골 소실이 나타난다. 이는 남성 호르몬의 감소에 따른 Sex Hormone Binding Globulin (SHBG)의 증가와 관련이 있다. 역학적 연구에서 SHBG의 증가가 골 소실에 영향을 미치며 골절 위험을 증가시키는 것으로 나타났다.
12)그 외에도 aromatase 효소활동의 감소를 통해서 testosterone으로부터 estradiol 의 생성의 감소도 남성 골다공증의 병태생리에 부가적인 역할을 담당한다.
13)Salmenda 등
14)은 혈청 estradiol 농도가 낮은 남성은 높은 남성에 비해 매년 1% 이상씩 골밀도 소실이 일어난다고 보고하였다. 따라서 estrogen 감소는 남녀 골다공증 모두에 있어서 중요한 역할을 한다. 이 시기 남성의 골 소실은 해면골 얇아짐 (trabecular thining)
15,16)으로 특징 지울수 있는데 이는 해면골 천공(trabecular perforation)보다 적은 척추 골소실 을 유발한다. 해면골 천공(trabecular perforation)은 폐경 여성에서 골 교체 상태(bone turnover state)가 높게 나타 나는 것을 의미한다. 그리고 남성에게 골밀도 보호기능을 나타내는 다른 요인은 남성이 여성보다 최대 골량(peak bone mass)이 10∼12% 높게 도달하며 해면골(trabecular bone)의 두께와 양은 비슷하지만 피질골 (cortical bone)이 더 두껍고 골(bone)이 더 크다.
17)이차성 골다공증의 3가지 주요 요인은 알콜 남용, 스테로이드 과용(쿠싱증후군, 만성 스테로이드 치료
등), 성선기능 저하증(hypogonadism)이다. 이런 원인들이 약 40∼50%를 차지한다.
18-20)다른 원인으로 갑상선
기능 항진증, 위장관 질환, 만성폐쇄성 폐질환, 파킨슨병 같은 신경근육질환, 당뇨, 다발성 골수종 또는 다른
악성 질환들, 약물(항경련제, 고용량 항암요법, 고혈압 약물, SSRI) 등이 있다(Table 1).
21-23)그밖에 여성과
마찬가지로 흡연, 운동부족, 마른 체격, 낮은 칼슘 섭취, 비타민 D 부족, 단백질 부족, 골절 가족력, 골절
병력, 저체중, 악력(grip strength)의 감소 등과 같은 위험 요인이 존재할 때 골절을 촉진시킨다.
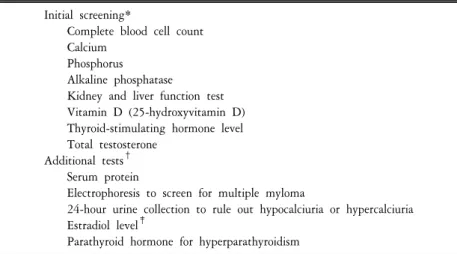
24,25)Table 2. Laboratory evaluation for osteoporosis in men Initial screening*
Complete blood cell count Calcium
Phosphorus Alkaline phosphatase
Kidney and liver function test Vitamin D (25-hydroxyvitamin D) Thyroid-stimulating hormone level Total testosterone
Additional tests
†Serum protein
Electrophoresis to screen for multiple myloma
24-hour urine collection to rule out hypocalciuria or hypercalciuria Estradiol level
‡Parathyroid hormone for hyperparathyroidism
*Recommended to determine cause in men diagnosed with osteoporosis.
†Consider further testing when initial screening dose not yield a definitive cause.
‡If level is low,it is likely to be contributing to osteoposis,but no treatment is available.
유전학적인 요인도 중요한 역할을 한다.
26)일란성 이란성 쌍둥이의 비교에서 보면 80%의 골밀도 변화가 유전과 연관이 있다.
27)그리고 역학적 연구에서는 부모의 골절 병력이 중요한 골다공증 위험 요인이라고 나타났다. 그러나 정확한 관련 유전자는 아직 밝혀지지 않았다.
28-30)2. 진단
일반적으로 남성에서는 골밀도(BMD)를 잘 측정하지 않지만 키가 작아지거나 척추 후만증, 골절, 증상이 있는 요통이 남성 골다공증의 처음 나타나는 특징이므로 검사가 필요하다.
31,32)골다공증은 보통 DXA 기계 로 측정하는데 주로 L1-L4, 고관절(hip), 특히 대퇴 경부, 전체 대퇴골(total femur)을 측정한다. Z score는 환자 의 골밀도를 비슷한 연령대와 비교한 것이며 T score는 정상 젊은이의 이상적인 최대 골량(peak bone mass)과 비교한 것이다. 측정한 부위중 가장 낮은 T 점수가 개인의 골밀도를 나타낸다.
33)International society for clinical densitometry에서는 골밀도가 −2.5 이하인 경우 남성 골다공증으로 진단한다.
34)International society for clinical densitometry에서 발표한 DXA의 적응증은 70세 이상의 남성, 골절 경향을 가진 사람, 골감소증이 나 골다공증으로 약물 치료를 받는 사람, 골다공증 약물 치료를 고려중인 사람, 치료 효과를 보기위해 낮은 골밀도 치료를 받고 있는 사람, 골밀도가 낮으나 현재 치료를 받고 있지 않은 사람 등이다.
35)DXA 검사에서 이상이 발견되거나 비외상성 골절(fragility fracture)이 있는 사람은 조혈기관 계통
(hematopoietic system)(다발성 골수종 등), 내분비 질환(갑상선 기능 항진증, 부갑상선기능 항진증등), 영양
결핍 소견(vitamin D 감소 등), 신장기능 등을 검사해야 한다. 처음 검사로는 CBC, 혈청 소변, 칼슘, ALP,
신기능, 간기능, 25-hydroxyvitamin D, I-PTH, TSH 등을 측정한다. 추가적으로 총 testosterone과 estradiol level
도 남성에게 측정하는 것이 좋다. 낮은 estradiol이 골다공증을 일으킬수 있으나 아직 특별히 받아들여지는
치료법은 없다(Table 2).
36,37)Testosterone level은 나이에 따라 감소하지만 병적인 범위로까지는 잘 떨어지지
않는다. 따라서 testosterone 보충 요법은 전립선암과 심장병 위험을 증가시킬수 있으므로 성선기능 저하증,
우울증, 기력저하, 근육량 감소 등 호르몬 감소에 의한 증상이 뚜렷할 때를 제외하고는 잘 사용하지 않는다.
골형성률(bone formation rate)은 bone specific ALP, osteocalcin 등으로 측정한다. 골흡수(bone resorption) 증가의 표지자(marker)는 콜라겐 분해 물질(collagen breakdown products)로 측정하며 소변에서의 pyridinoline, deoxypyri- dinoline, N-telopeptide crosslinked collagen type1과 혈청 C-telopeptide crosslinked collagen type1으로 측정할 수 있 다. 현재 치료제로 골흡수 억제제가 많이 사용됨으로 N-telopeptide crosslinked collagen type1과 C-telopeptide crosslinked collagen type1이 가장 흔히 사용하는 표지자이다. 높은 골 교체에 의한 골다공증(high turnover osteoporosis)에서는 파골세포(osteoclast)에 의한 골흡수가 증가되어 골모세포(osteoblast)가 이를 따라오지 못하 게 된다. 이것은 콜라겐 분해 물질(collagen breakdown products) 증가로 알 수 있다. 역으로 말하면 골모세포에 의한 골형성(osteoblastic bone formation)의 실패로 인해 발생하는 낮은 골 교체에 의한 골다공증(low turnover osteoporosis)에서는 N-telopeptide crosslinked collagen type1이 정상이거나 낮을 수 있다. 그리고 골 형성 표지자 는 특히 억제되어 있다.
38)3. 치료
최근의 후향성 코호트 연구에 따르면 65세 이상의 남성 골다공증 환자중에 7.1% 그리고 척추, 고관절 골절 환자의 16%가 골다공증 약물치료를 받고 있는 것으로 나타났다.
39)남성에게도 골다공증의 예방법은 여성과 유사하다. National Institute of Health and Food and Nutrition Board에서 권장하는 음식 칼슘 섭취는 1,200∼1,500 mg이며
40)비타민 D 섭취량은 400∼600 IU/day은 되어야하며 70이상의 남성은 600∼800 IU 섭취가 권장된다. 적절한 운동도 반드시 필요하다.
그러나 남성 골다공증 환자에게 약물치료는 주로 고위험도의 골절을 가진 경우에 추천된다. 남성 골다공 증에도 bisphosphonate를 주된 치료로 사용하는데
41)bisphosphonate는 pyrophosphonate의 유사체로 화학적으로 분해되지 않으며 뼈에 강력하게 결합하며 뼈의 파골세포에 의한 골흡수(osteoclastic resorption)를 막는 역할을 한다. Alendronate, risedronate, ibandronate 등은 지금까지 광범위한 연구가 시행되었으며 골밀도 증가와 골절 률을 50%정도 향상시키는 것으로 나타났다.
42)이런 약들은 매우 높은 산성이어서 소화불량을 야기할 수 있다. Alendronate와 risedronate는 매일복용 또는 일주에 한번 복용할 수 있으며 ibandronate는 1개월에 1회 복용, 또는 3개월마다 주사가 가능하다. 처음에는 주로 여성을 주 대상으로 치료 효과를 평가해왔으나 최근 에는 남성에게도 효과가 있다고 입증되고 있으며
43)특정부위의 골절 예방에 대한 입증은 어렵지만 특히 척추 골절에 대해서는 남성에게도 똑같은 효과가 있다고 보고되고 있다. 그러나 시간이 지남에 따라 bisphosphonate는 골 교체(bone turnover)를 감소시키며 동물실험에서 높은 농도에서 골의 강도(bone strength)와 탄성(resilience)이 감소하였다. 일부 연구에서는 장기간 사용하면 횡력에 의한 골절(transverse stress fracture)을 가져올 수 있다고 하였으며 이런 사람들은 조직검사를 하면 매우 낮은 골 교체(turnover)를 보였다. 따라서 bisphosphonate는 효과는 뛰어나지만 골 교체 표지자(bone turnover marker)를 반드시 추적하여 매우 억제되어 있다면 bisphosphonate를 끊고 N-telopeptide crosslinked collagen type 1 등이 치료수준(therapeutic level)으로 돌아 올때까지 기다려야 한다.
44)메타 분석에서 남성에서 alendronate 치료는 낮은 골밀도나 골절이 있는 경우 척추 골절위험을 효과적으로 감소시켰으나 비척추 골절에 대한 효과는 불충분하였으며
45)일주 한번 투여한(70 mg) 경우와 매일 투여한 경우(10 mg)에서 효과는 비슷하였다.
46)Risedronate 역시 골밀도를 증가시키고 척추 골절률을 감소 시킨다.
47)그리고 최근에 미국뿐 아니라 국내에
서도 남성 골다공증 치료제로 승인되었다. Alendronate와 risedronate는 또한 남성에서 스테로이드 과용, 성선
기능저하증, 이식등과 같이 이차성 골다공증이 원인인 경우에도 효과가 있었다.
48-52)그리고 여러나라에서
스테로이드로 인한 남성 골다공증 치료에 승인되었다.
53)Etidronate 2주씩 3개월간격으로 치료하는 방법도
Table 3. Treatment of osteoporosis, with grades of evidence, in men
Drug Dosage Grade* Contraindications and side effects
Nutrients, total daily intake (diet+supplements)
Calcium 1,500 mg C Contraindications: hypercalciuria
hypercalcemia Vitamin D
3(cholecalciferol) ≧800 IU A
Bisphosphonate therapy
Alendronate
†70 mg/week A Contraindications: renal failure
or Risedronate
†35 mg/week (glomerular filtration rate<30 ml/min), history of allergy to bisphosphonate exposure.
400 mg/d for Side effects: usually limited to GI intolerance.
or Cyclic etidronate
‡14d per 90-d cycle
Anabolic therapy: teriparatide 20 ug/d D
§Contraindications: skeletal malignancy, subcutaneously history of radio therapy of for 18 month the skeleton, Paget’s disease,
hypercalcemia
Side effects: nausea, headaches, muscle cramps
*Grades of evidence, from the 2002 osteoporosis canada guidelines.
†For treatment of idiopathic osteoporosis,or for treatment and prevention of glucocorticoid osteoporosis.
‡For prevention (not treatment) of glucocorticoid osteoporosis.
§Although the randomized controlled trials (RCTs) that involved men were not powered to detect reductions in fracture incidence, the pivotal RCT (evidence grade A),which involved postmenopausal women with severe osteoporosis,resulted in significant reductions in both vertebral and nonvertebral fracture.
또한 스테로이드에 의한 남성 골다공증을 예방하는데에 효과적이었다(Table 3).
54)최근에 human recombinant PTH (1-34)-teriparatide가 높은 골절위험을 가진 남성환자에게 효과적인 것으로 나타났다(일차성 또는 이차성 골다공증, 성선기능저하에 의한 골다공증). 그러나 약물비용, 복잡한 투약 일정, 잠재적인 위험성 등이 사용하는데 있어서 제한요인이다.
55-59)Teriparatide를 매일 20 μg 피하로 사용하 면 골(bone)에 동화 효과(anabolic effect)를 나타내며 요추 골밀도와 골 형성 표지자(bone formation marker)를 빠르게 증가 시킨다. 여러 연구에 의하면 2년간 척추 골밀도가 13% 증가하였으며 고관절 골밀도도 유사하 게 증가하였다.
60-63)지금까지 연구 대상자수가 작고 소규모 연구라서 PTH의 남성 골절률 감소에 대해서는 확실한 자료는 없지만 관찰 연구에서 teriparatide가 중등도에서 중증의 척추 골절의 위험을 감소시키는 것으로 나타났다.
64)Teriparatide와 bisphosphonate를 함께 사용한 경우 남성에서도 여성과 마찬가지로 단독 사용한 경우보다 이득 을 보지 못하였다.
65-68)PTH 적응증으로는 bisphosphonate를 사용하는데도 골밀도가 감소되고 골절이 발생되 고 골교체상태가 낮게 유지될때 사용할수 있다.
69)성선기능저하증인 남성에서 testosterone 보충요법이 골밀도를 증가시키는 것으로 나타났으나 골절률을 낮추는지는 알려져 있지 않다.
70,71)일부 연구에 따르면 남성호르몬이 감소된 남성에서 낮은 용량의 testo- sterone 치료는 요추에 이득을 나타냈으나 대퇴 경부에는 큰 이득을 보이지 않았다.
72)치료방법으로는 일반 적으로 피하요법이 근주요법 보다는 골밀도에 좋은 효과를 보였다.
SERM (selective estrogen receptor modulator)제제인 raloxifene은 전립선암에 대해서 억제 효과가 있으며
73), 척
추 골밀도를 증가시키고 척추 골절률을 감소시키는 것으로 나타났으며 적은 여성화 효과를 가져서 최근에
남성에도 적용되고 있다.
74)50명의 노인에서 6개월간 raloxifene (60 mg/day)으로 치료한 연구에서 raloxifen을 혈청 estradiol level이 96 pmol/L 이하인 남성에 투여했을경우 골 흡수 표지자인 소변의 cross-linked N-telopeptide of type I collagen (NTX) 가 감소하였으며 반면 이 estrogen level 이상인 경우 골 흡수가 증가하였다. 이것은 raloxifen을 높은 용량으로 120 mg/day 6주간 중년 성선기능 정상인 남성에 적용했을때 estradiol level이 101.8 pmol/L 이하인 경우 골 전환 표지자가 상당히 감소한 결과와 비슷한 것이다.
따라서 남성에서 raloxifene 치료는 혈청 estradiol level이 낮은 경우에 골 대사에 좋은 효과를 나타낸다.
75)결 론
남성 골다공증은 현재 증가 추세에 있으며 노인인구에서 특히 많이 발생하고 골절이 동반될 경우 심각한 고통을 수반하게 된다. 따라서 적절한 진단을 통해 조기에 발견하고 치료한다면 골다공증에 의한 합병증을 예방할수 있다. 최근에 새로운 약제들이 개발되고 있으며 남성 골다공증에도 많이 적용되고 있기 때문에 앞으로 더 좋은 치료 방법과 결과가 나올것으로 기대되고 있어 적극적인 관심을 가지고 진단과 치료를 해야할 것이다.
참고문헌
1. Melton LJ III, Khosla S, Achenbach SJ, O'Connor MK, O'Fallon WM, Riggs BL. Effects of body size and skeletal site on the estimated prevalence of osteoporosis in women and men. Osteoporos Int 2000;11:977-83.
2. Melton LJ. Epidemiology of fractures. In: Riggs BL, Melton LJ, editors. Osteoporosis: etiology, diagnosis and management. 2nd ed. Philadelphia: Lippincott-Raven Publishers; 1995. p225-47.
3. Schuitt SC, van der Klift M, Weel AE, de Laet CE, Burger H, Seeman E, et al. Fracture incidence and association with bone mineral density in elderly men and women: the Rotterdam Study. Bone 2004;34:195-202.
4. Cummings SR, Karpf DB, Harris F, Genant HK, Ensrud K, LaCroix AZ, et al. Improvement in spine bone density and reduction in risk of vertebral factures during treatment with antiresorptive drugs. Am J Med 2002;112:281-9.
5. Chang KP, Center JR, Nguyen TV, Eisman JA. Incidence of hip and other osteoporotic fractures in elderly men and women:
Dubbo Osteoporosis Epidemiology Study. J Bone Miner Res 2004;19:532-6.
6. Cooper C, Campion G, Melton LJ 3rd. Hip fractures in the elderly: A world-wide projection. Osteoporos Int 1992;2:285-9.
7. Melton LJ 3rd, Atkinson EJ, O'Connor MK, O'Fallon WM, Riggs BL. Bone density and fracture risk in men. J Bone Miner Res 1998;13:1915-23.
8. Seeman E. Osteoporosis in men. Am J Med 1993;30:S22-8.
9. Cooper C, Atkinson EJ, O'FalIon WM, Melton LJ 3rd. Incidence of clinically diagnosed vertebral fractures: A population-based study in Rochester, Minnesota 1985–89. J Bone Miner Res 1992;7:221-7.
10. Kanis JA, Pitt FA. Epidemiology of osteoporosis. Bone 1992;13:S7-S15.
11. Alffram PA, Bauer CGH. Epidemiology of fractures of the forearm. J Bone Joint Surg Am 1962;44:105-14.
12. Goderie-Plomp HW, Van der Klift M, De Ronde W, Hofman A, de Jong FH, Pols HA. Endogenous sex hormones, sex hormone-binding globulin, and the risk of incident vertebral fractures in elderly men and women: The Rotterdam study. J Clin Endocrinol Metab 2004;89:3261-9.
13. Van Pottelbergh I, Gomaere S, Kaufman JM. Bioavailable estradiol and an aromatase gene polymorphism are determinants of bone mineral density changes in men over 70 years of age. J Clin Endocrinol Metab 2003;88:3075-81.
14. Slemenda CW, Longcope C, Zhou L, Hui SL, Peacock M, Johnston CC. Sex steroids and bone mass in older men: Positive associations with serum estrogens and negative associations with androgens. J Clin Invest 1997;100:1755-9.
15. Wang XF, Duan Y, Beck T, Seeman E. Varying contributions of growth and ageing to racial and sex differences in femoral neck structure and strength in old age. Bone 2005;36:978-86.
16. Seeman E, Bianchi G, Khosla S. Bone fragility in men-where are we? Osteoporos Int 2006;17:1577-83.
17. Delaney MF. Strategies for the prevention and treatment of osteoporosis during early postmenopause. Am J Obstet Gyneco 2006;19:S12-23.
18. Bilezikian JP. Osteoporosis in men. J Clin Endocrinol Metab 1999;84:3431-4.
19. Orwoll ES. Osteoporosis in men. Endocr Rev 1995;16:87-116.
20. Seeman E. Osteoporosis in men: Epidemiology, pathophysiology, and treatment possibilities. Am J Med 1993;95:22-8.
21. Cauley JA, Fullman RL, Stone KL, Zmuda JM, Bauer DC, Connor EB, et al. Factors associated with the lumbar spine and proximal femur bone mineral density in older men. Osteoporos Int 2005;16:1525-37.
22. Lau EM, Leung PC, Kwok T, Woo J, Lynn H, Orwoll E, et al. The determinants of bone mineral density in Chinese men-results from Mr. Os (Hong Kong), the first cohort study on osteoporosis in Asian men. Osteoporos Int 2006;17:297-303.
23. Gennari L, Bilezikian JP. Osteoporosis in men. Endocrinol Metab Clin North Am 2007;36:399-419.
24. Seeman E, Melton LJ 3rd, O`Fallon WM, Riggs BL. Risk factors for spinal osteoporosis in men. Am J Med 1983;75:977-82.
25. Cummings SR, Browner W, Black DM, Nevitt MC, Genant HK, Cauley J, et al. Bone density at various sites for prediction of hip fractures: The Study of Osteoporotic Fractures Research Group. Lancet 1993;341:72-5.
26. Gennari L, Brandi ML. Genetics of male osteoporosis. Calcif Tissue Int 2001;69:200-4.
27. Eisman JA. Genetics of osteoporosis. Endocr Rev 1999;20:788-804.
28. Cohen-Solal ME, Baudoin C, Omouri M, KUNTZ D, Vernejoul DE. Bone mass in middle-aged osteoporotic men and their relatives: Familial effect. J Bone Miner Res 1998;13:1909-14.
29. Soroko SB, Barrett-Connor E, Edelstein SL, Kritz-Silverstein D. Family history of osteoporosis and bone mineral density at the axial skeleton: The Rancho-Bernardo Study. J Bone Miner Res 1994;9:761-9.
30. Diaz MN, O'Neill WO, Silman AJ. European Vertebral Osteoporosis Study Group. The influence of family history of hip fracture on the risk of vertebral deformity in men and women: The European Vertebral Osteoporosis Study. Bone 1997;20:145-9.
31. Orwoll E. Assessing bone density in men. J Bone Miner Res 2000;15:1867-70.
32. Lewiecki EM, Watts NB, McClung MR, Petak SM, Bachrach LK, Shepherd JA, et al. International Society for Clinical Densitometry. Official positions of the international society for clinical densitometry. J Clin Endocrinol Metab 2004;89:3651-5.
33. Baim S, Wilson CR, Lewiecki EM, Luckey MM, Downs RW Jr, Lentle BC. Precision assessment and radiation safety for dual-energy X-ray absorptiometry: Position paper of the International Society for Clinical Densitometry. J Clin Densitom 2005;8:371-8.
34. Cummings SR, Cawthon PM, Ensrud KE, Cauley JA, Fink HA, Orwoll ES, et al. BMD and risk of hip and nonvertebral fractures in older men: A prospective study and comparison with older women. J Bone Miner Res 2006;21:1550-6.
35. Writing Group for the ISCD Position Development Conference. Indications and reporting for dual-energy x-ray absorptiometry.
J Clin Densitom 2004;7:37-44.
36. Orwoll ES. Osteoporosis in men. Endocrinol Metab Clin North Am 1998;27:349-67.
37. Campion JM, Maricic MJ. Osteoporosis in men. Am Fam Physician 2003;67:1521-6.
38. Miller PD, Baran DT, Bilezikian JP, Greenspan SL, Lindsay R, Riggs BL, et al. Practical clinical application of biochemical markers of bone turnover: Consensus of an expert panel. J Clin Densitom 1999;2:323-80.
39. Feldstein AC, Nichols G, Orwoll E, Elmer PJ, Smith DH, Herson M, et al. The near absence of osteoporosis treatment in older men with fractures. Osteoporos Int 2005;16:953-62.
40. Bilezikian JP, Panel Members. Optimal calcium intake: Statement of the consensus development panel on optimal calcium intake.
JAMA 1994;272:1942-8.
41. Orwoll ES. Treatment of osteoporosis in men. Calcif Tissue Int 2004;75:114-9.
42. Black DM, Greenspan SL, Ensrud KE, Palermo L, McGowan JA, Lang TF, et al. The effects of parathyroid hormone and alendronate alone or in combination in postmenopausal osteoporosis. N Engl J Med 2003;349:1207-15.
43. Ringe JD, Orwoll E, Daifotis A, Lombardi A. Treatment of male osteoporosis: recent advances with alendronate. Osteoporos Int 2002;13:195-9.
44. Odvina CV, Zerwekh JE, Rao DS, Maalouf N, Gottschalk FA, Pak CY. Severely suppressed bone turnover: A potential complication of alendronate therapy. J Clin Endocrinol Metab 2005;900:1897-9.
45. Sawka AM, Papaioannou A, Adachi JD, Gafni A, Hanley DA, Thabane L. Does alendronate reduce the risk of fracture in men?
A meta-analysis incorporating prior knowledge of anti-fracture efficacy in women. BMC Musculoskelet Disord 2005;6:39.
46. Greenspan S, Field–Munves E, Tonino R, Smith M, Petruschke R, Wang L, et al. Tolerability of once-weekly alendronate in patients with osteoporosis: A randomized,,double-blind, placebo controlled study. Mayo Clin Proc 2002;77:1044-52.
47. Ringe JD, Faber H, Farahmand P, Dorst A. Efficacy of risedronate in men with primary and secondary osteoporosis: Results of a 1-year study. Rheumatol INT 2006;26:427-31.
48. Minsola S, Scillitani A, Romagnoli E. Alendronate or alfacalcidol in glucocorticoid-induced osteoporosis. N Engl J Med 2006;355:675-84.
49. Shimon I, Eshed V, Doolman R, Sela BA, Karasik A, Vered I. Alendronate for osteoporosis in men with androgen-repleted hypogonadism. Osteoporos Int 2005;16:1591-6.
50. Millonig G, Graziadei IW, Eichler D, Pfeiffer KP, Finkenstedt G, Muehllechner, et al. Alendronate in combination with calcium and vitamin D prevents bone loss after orthotopic liver transplantation: A prospective single-center study. Liver Transpl 2005;11:960-6.
51. Shane E, Addesso V, Namerow PB, Mcmahon DJ, Lo SH, Staron RB, et al. Alendronate versus calcitriol for the prevention of bone loss after cardiac transplantation. N Engl J Med 2004;350:767-76.
52. Sato Y, Iwamoto J, Kanoko T, Satoh K. Risedronate sodium therapy for prevention of hip fracture in men 65 years or older after stroke. Arch Intern Med 2005;165:1743-8.
53. Thomson PDR, Montvale NJ. Physicians' desk reference: PDR. 57th ed. 2003. p3550.
54. Khan AA, Hodsman AB, Papaioannou A, Kendler D, Brown JP, Olszynski WP. Management of osteoporosis in men: An update and case example. CMAJ 2007;176:345-8.
55. Kurland ES, Cosman F, McMahon DJ, Rosen CJ, Lindsay R, Bilezikian JP, et al. Parathyroid hormone as a therapy for idiopathic osteoporosis in men: Effects on bone mineral density and bone markers. J Clin Endocrinol Metab 2000;85:3069-76.
56. Orwoll ES, Scheele WH, Paul S, Adami S, Syversen U, Diez-Perez A, et al. The effect of teriparatide [human parathyroid hormone (1-34) therapy on bone density in men with osteoporosis. J Bone Miner Res 2003;18:9-17.
57. Misof BM, Roschger P, Cosman F, Kurland ES, Tesch W, Messmer P, et al. Effects of intermittent parathyroid hormone administration on bone mineralization density in iliac crest biopsies from patients with osteoporosis: A paired study before and after treatment. J Clin Endocrinol Metab 2003;88:1150-6.
58. Kaufman JM, Orwoll E, Goemaere S, San Martin J, Hossain A, Dalsky GP, et al. Teriparatide effects on vertebral fractures and bone mineral density in men with osteoporosis: Treatment and discontinuation of therapy. Osteoporos Int 2005;16:510-6.
59. Bilezikian JP, Kurland ES. Therapy of male osteoporosis with parathyroid hormone. Calcif Tissue Int 2001:69;248-51.
60. Hodsman AC, Bauer DC, Dempster DW, Dian L, Henley DA, Harris ST, et al. Parathyroid hormone and teriparatide for the treatment of osteoporosis: A review of the evidence and suggested guidelines for its use. Endocr Rev 2005;26:688-703 61. Dempster DW, Cosman F, Kurland ES, Zhou H, Nieves J, Woelfert L, et al. Effects of daily treatment with parathyroid hormone
on bone microarchitecture and turnover in patients with osteoporosis: A paired biopsy study. J Bone Miner Res 2001;16:1846-53.
62. Neer RM, Arnaud CD, Zanchetta JR, Prince R, Gaich GA, Reginster JY, et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med 2001;344:1434-41.
63. Body JJ, Gaich GA, Scheele WH, Kulkarni PM, Miller PD, Peretz A, et al. A andomized double-blind trial to compare the efficacy of teriparatide [recombinant human parathyroid hormone (1-34)] with alendronate in postmenopausal women with osteoporosis. J Clin Endocrinol Metab 2002;87:4528-35.
64. Kaufman JM, Orwoll E, Goemaere S, San Martin J, Hossain A, Dalsky GP, et al. Teriparatide effects on vertebral fractures and bone mineral density in men with osteoporosis: Treatment and discontinuation of therapy. Osteoporos Int 2005;16:510-6.
65. Finkelstein JS, Hayes A, Hunzelman JL, Wyland JJ, Lee H, Neer RM. The effects of parathyroid hormone, alendronate, or both in men with osteoporosis. N Engl J Med 2003;349:1216-26.
66. Kurland ES, Heller SL, Diamond B, McMahon DJ, Cosman F, Bilezikian JP. The importance of bisphosphonate therapy in maintaining bone mass in men after therapy with teriparatide [human parathyroid hormone (1-34). Osteoporos Int 2004;15:992-7.
67. Bilezikian JP, Rubin MR. Combination/sequential therapies for anabolic and antiresorptive skeletal agents for osteoporosis. Curr Osteoporos Rep 2006:4:5-13
68. Finkelstein JS, Hayes A, Hunjelman JL, Wyland JJ, Lee H, Neer RM. The effects of parathyroid hormone, alendronate, or both in men with osteoporosis. N Engl J Med 2003;349:1216-26.
69. Alkhiary YM, Gerstenfeld LC, Krall E, Westmore M, Sato M, Mitlak BH, et al. Enhancement of experimental fracture-healing by systemic administration of recombinant human parathyroid hormone. J Bone Joint Surg Am 2005;87:731-41.
70. Behre HM, Kliesch S, Leifke E, Link TM, Nieschlag E. Long-term effect of testosterone therapy on bone mineral density in hypogonadal men. J Clin Endocrinol Metab 1997;82:2386-90.
71. Snyder PJ, Peachey H, Berlin JA, Hannoush P, Haddad G, Dlewati A, et al. Effects of testosterone replacement in hypogonadal men. J Clin Endocrinol Metab 2000;85:2670-7.
72. Smith MR, McGovern FJ, Zietman AL, Fallon MA, Hayden DL, Schoenfeld DA, et al. Pamidronate to prevent bone loss during androgen deprivation therapy for prostate cancer. N Engl J Med 2001;345:948-55.
73. Anderson FH, Francis RM, Peaston RT, Wastell HJ. Androgen supplementation in eugonadal men with osteoporosis: Effects of six months' treatment on markers of bone formation and resorption. J Bone Miner Res 1997;12:472-8.
74. Maricic M, Adachi JD, Sarkar S, Wu W, Wong M, Harper KD. Early effects of raloxifene on clinical vertebral fractures at 12 months in postmenopausal women with osteoporosis. Arch Intern Med 2002;162:1140-3.
75. Doran PM, Riggs BL, Atkinson EJ, Khosla S. Effects of raloxifene, a selective estrogen receptor modultor, on bone turnover markers and serum sex steroid and lipid levels in elderly men. J Bone Miner Res 2001;16:2118-25.