- 118 -
J Rhinol 17(1), 2010 www.ksrhino.or.kr
Fronto-Ethmoidal Osteoid Osteoma with Orbital Extension
Sung-Moon Hong, MD, Il-Ho Park, MD and Heung-Man Lee, MD, PhD
Department of Otolaryngology-Head and Neck Surgery, Korea University College of Medicine, Seoul, Korea ABSTRACT
An osteoid osteoma is a benign tumor that is usually located in the cortex of long bones and vertebrae and rarely involves parana- sal sinuses. We report a case of a 58-year-old woman with right epiphora, orbital pain, and exophthalmos. The mass was removed via an external frontoethmoidectomy approach. After surgery, the patient reported prompt relief of the orbital pain and epiphora, and opthalmologic examination showed improvement of exophthalmos. The post-operative CT scan of the paranasal sinus obtained 1 year later showed no evidence of tumor recurrence or complication. Although osteoid osteoma is rare in paranasal sinuses, it should be considered if there is a bone density mass and complete excision should be performed with care.
KEY WORDS:OsteomaㆍOsteoidㆍExophthalmos.
Address correspondences and reprint requests to Heung-Man Lee, M.D., Ph.D., Department of Otorhinolaryngology-Head and Neck Surgery, Korea University Collage of Medicine, 80 Guro- dong, Guro-gu, Seoul 152-703, Korea
Tel:82-2-2626-3185, Fax:82-2-868-0475 E-mail:[email protected]
Received for publication on November 30, 2009 Accepted for publication on February 2, 2010
INTRODUCTION
An osteoid osteoma is a solitary, benign lesion of bone, usually occurring in a long bone cortex and causing sig- nificant nocturnal pain that usually responds to non-ste- roidal anti-inflammatory medications. Osteoid osteomas occur most commonly in the femur, tibia, and spine.1) Os- teoid osteomas rarely involve the paranasal sinuses, the surgical approach to which is not easy because of the ac- cess and surrounding vital structures.2) Herein we report a very rare case of a fronto-ethmoidal osteoid osteoma with orbital extension.
CASE REPORT
A 58-year-old woman was referred to our department by an ophthalmologist of the same hospital. She had right epiphora, easily controllable orbital pain, and eye protrusion for 1 year. The physical examination revealed a 2×3 cm, firm mass palpated in the area of the right medial canthus.
There were no abnormal findings on the nasal endoscopic examination. The ophthalmologic examination showed slight limitation in medial movement of the right eye.
A computed tomograpic (CT) scan of the paranasal si-
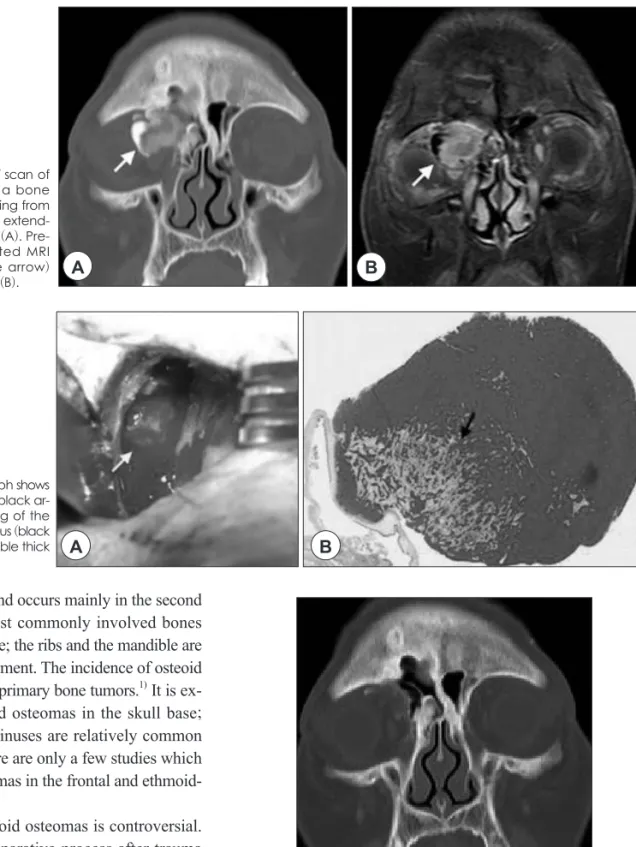
nuses was performed, and there was a 2×3 cm, high den- sity mass in the right frontoethmoid sinus which destructed the lamina papylacea and invaded the right orbit. The mass displaced the superior and medial rectus muscles, and the right eyeball was shifted inferolaterally due to the mass effect (Fig. 1A). Magnetic resonance imaging (MRI) of the paranasal sinuses showed the same mass with peripheral enhancement (Fig. 1B).
Under general anesthesia, an external frontoethmoidal incision was used around the right medial canthus in order to provide access to the mass. The lamina papyracea was in continuity with the mass. The orbit was gently shifted laterally, and the mass was carefully detached from orbital periosteum. The periosteum of the medial wall of the orbit was intact without any defects (Fig. 2A). The remaining part of the mass was separated from the frontoethmoid sinus. There were no severe complications, such as hem- orrhage, ocular disturbance, or loss of vision. The histopath- ologic examination revealed two histologically different bony compartments, a central core of vascular osteoid tis- sue (the nidus), and surrounding bone trabeculae (Fig. 2B).
The patient reported prompt relief of the orbital pain and epiphora, and the ophthalmologic examination showed improvement of the exophthalmos. The post-operative CT scan performed 1year later showed no evidence of tumor recurrence (Fig. 3).
DISCUSSION
An osteoid osteoma is a benign tumor that is most usu- ally located in the cortex of long bones and vertebrae. It
online©MLComm
Hong et al:Osteoid Osteoma with Orbital Extension / 119
osteoid osteomas. Radiographically, osteoid osteomas appear as round-to-ovoid radiopaque lesions with a nidus which has a radiolucent center surrounded by dense scle- rosis.3) The MRI appearance depends on the amount of calcification within the nidus, the amount of edema in the bone, the size of the fibrovascular zone, and reactive scle- rosis. MRI is more sensitive than a CT in evaluating soft tissue and bone marrow changes adjacent to the nidus.
has a male preponderance and occurs mainly in the second and third decades. The most commonly involved bones are the femur, tibia, and spine; the ribs and the mandible are less frequent sites of involvement. The incidence of osteoid osteomas is about 3% of all primary bone tumors.1) It is ex- tremely rare to find osteoid osteomas in the skull base;
the frontal and ethmoidal sinuses are relatively common sites in the skull base.2) There are only a few studies which have reported osteoid osteomas in the frontal and ethmoid- al sinuses.
The pathogenesis of osteoid osteomas is controversial.
Abnormal healing and a reparative process after trauma is considered to be a contributing factor to the pathogene- sis of osteoid osteomas, but the correlation between inju- ry and the onset of osteoid osteoma remains inapparent.
Indeed, some authorities have suggested that osteoid os- teomas are neoplasms. However, osteoid osteomas have limited growth potential and are typically 1.5 cm in diam- eter when evaluated. Because of the age distribution of the patients and the limited growth potential characteristics, it is thought that osteoid osteomas may heal spontane- ously.1)
A CT is the most adequate imaging modality to detect
Fig. 3. Post-operative coronal CT scan of the paranasal sinuses performed 1year later shows no evidence of tumor recurrence.
Fig. 2. Intra-operative photograph shows the orbital portion of the mass (black ar- row)(A). Histopathologic finding of the mass shows a wedge-shaped nidus (black arrow) with a surrounding variable thick
layer of dense bone (H & E)(B). A B
Fig. 1. Pre-operative coronal CT scan of the paranasal sinuses shows a bone density mass (white arrow) arising from the right fronto-ethmoidal sinus, extend- ing to the ipsilateral right orbit (A). Pre- operative coronal T1-weighted MRI shows the same mass (white arrow)
with peripheral enhancement (B). A B
120 / J Rhinol 17(1), 2010
Thus, MRI should be interpreted with plain radiographs and a CT.4)
The clinical symptoms depend on the location of the lesion. The most remarkable early symptom is mild inter- mittent vague pain, gradually increasing in severity with nocturnal paroxysms. Characteristically, this pain responds to oral salicylates or non-steroidal anti-inflammatory drug treatment.5)
In most case, the treatment consists of en bloc resection or curettage of the tumor. If the lesion is asymptomatic and small, it can be left in situ and observed. The indication for surgery relies on the severity and duration of symptoms and the patient’s pain tolerance. Generally, complete sur- gical removal of the nidus is sufficient and essential for immediate, lasting pain relief. Accurate localization of the nidus by CT is critical for predictable success of surgi- cal intervention.6) Recurrence is likely due to incomplete excision of the nidus, and a recurrence rate is approxi- mately 10%.1)
In conclusion, osteoid osteomas of the paranasal sinus- es are very rare and only a few cases have been reported.
Excision is difficult and not without risk, especially if the osteoma invades adjacent vital structures. In the case re- ported herein, the tumor invaded the orbit and the patient could have had some opthalmologic complications. How- ever, there were no complications and the symptoms im- proved dramatically.
Acknowledgments
This study was supported by a grant of the Korea Healthcare technology R&D Projects, Ministry for Health, Welfare & Family Affairs, Republic of Korea (A090084).
저자역할(Author Contributions)
홍성문, 박일호, 이흥만은 본 연구에서 모든 자료에 접근할 수 있 으며 자료의 완전성과 자료 분석의 정확성에 책임을 지고 있습니 다. 연구 기획:홍성문. 자료 해석 및 분석:홍성문, 박일호. 논 문초안:홍성문. 논문수정:이흥만. 연구 총괄:이흥만.
REFERENCES
1) Lee EH, Shafi M, Hui JH. Osteoid osteoma; a current review. J Pe- diatr Orthop 2006;26:695-700.
2) Grayeli AB, Redondo A, Sterkers O. Anterior skull base osteoid osteoma: case report. Br J Neurosurg 1998;12:173-5.
3) Pai SB, Harish K, Venkatesh M, Udayshankar, Jermely D. Ethmoid osteoid osteoma with orbital and intracranial extension? a case re- port. BMC Ear, Nose and Throat Disord 2005 Mar 11;5:2.
4) Assoun J, Richardi G, Railhac JJ, Baunin C, Fajadet P, Giron J, et al. Osteoid osteoma: MR imaging versus CT. Radiology 1994;191:
217-23.
5) Greenspan A. Benign bone-forming lesions: osteoma, osteoid oste- oma, and osteoblastoma. Clinical, imaging, pathologic, and differ- ential considerations. Skeletal Radiol 1993;22:485-500.
6) Campanacci M, Ruggieri P, Gasbarrini A, Ferraro A, Campanacci L. Osteoid osteoma. Direct visual identification and intralesional excision of the nidus with minimal removal of bone. J Bone Joint Surg Br 1999;81:814-20.