Original Article
pISSN 2233-9019 · eISSN 2233-9116
Korean J Fam Pract. 2015;5(3, suppl. 2):732-737
KJFP
Korean Journal of Family Practice서 론
2012
년 국가암등록통계 자료에 의하면 전체 평균수명81
세, 남 자77
세, 여자84
세이며 평균수명까지 생존할 경우 암 발생 확률은 전체37
.3
%로 남자는5
명중2
명, 여자는3
명중1
명으로 집계되었 고1999
년부터2012
년까지 연간 약3
.5
%씩 증가되었다.5
년 생존 율은68
.1
%로 증가하는 추세이나2013
년 암으로 사망한 사람은 총75
,334
명으로 전체 사망자의28
.3
%에 이른다.1)통증은 말기 암환자에서 가장 흔하고 괴로운 증상중의 하나이다.
암성 통증의
80
~90
%는 약물요법으로 조절 가능하다.2)69
%의 암환 자들은 통증으로 인해 능력의 저하를 초래한다고 하였다.3) 대부분의 말기 암 환자들은 마약성 진통제로 통증을 조절하고 있다. 하지만
56
% 에서82
.3
% 의 환자들은 불충분한 통증 치료를 받고 있는 것으 로 알려지고 있다.4-5) 불충분한 통증조절의 여러 원인으로 환자가 마 약에 대한 편견으로 처방을 원하지 않는 점과 의료진의 통증관리에 대한 불충분한 지식과 부적절한 통증 평가, 마약 처방에 부정적인 태 도가 포함되겠다. 한 국내 연구의 의하면 의사들이 중간용량의 마약 성 진통제 처방을 꺼려하는 이유로 중독에 대한 염려, 호흡곤란의 위 험인식 등이 다른 나라에 비해 더 높은 것으로 보고 되었다.6) 그러나 외국의 연구 결과에서는 중간용량의 마약성 진통제가 저용량 마약성 진통제 사용에 비해 말기 암 환자의 생존기간을 감소시키지 않는 것 으로 보고하였다.7) 세계보건기구에서도 중등도 이상의 암성 통증에일개 종합병원 호스피스 병동에서 사용된 임종 일주일 전 마약성 진통제 용량
송은
1, 송미연
2, 정승필
2, 변정길
1, 박경택
1, 오택근
1, 김현우
1, 이석환
1,*1대구의료원, 2영남대학교 의과대학 영남대학교 의료원 가정의학과
The narcotic analgesics in terminal cancer patients during the last 1 week to death
En Sung
1, Mi-Yoen Song
2, Seung-Pil Jung
2, Jung-Kil Byun
1, Kyung-Taek Park
1, Taek-Geun Oh
1, Hyun-Woo Kim
1, Seock-Hwan Lee
1,*1
Department of Family Medicine, Daegu Medical Center, Dae-gu;
2Department of Family medicine, Yeung-Nam University Medical Center, Yeung-Nam University School, College of Medicine, Dae-gu, Korea
Background: Physicians’ prejudices against narcotic analgesics have sometimes contributed to poor pain management of terminal cancer patients. In this study, we investigated how clinical differences in morphine administration affect patients’ quality of life by surveying morphine administration during patients’ last week of life at a hospice center.
Methods: This study was performed on 84 terminal cancer patients who had been admitted to hospice for more than one week and expired in the hospital between 1 January and 31 December in 2014. The morphine dose was calculated by using OME (oral morphine equivalent). We classified doses as either moderate (199mg OME), high (200mg OME), or very high (399mg OME and over). General characteristics, clinical characteristics, and the difference in narcotic analgesic type were tested for corellation by chi-square and one-way ANOVA. Age and duration of hospitalization were tested for correlation with morphine dose using the Pearson correlation coefficient.
Results: Age and OME had a negative correlation. The high dose group was associated with prescription of morphine injections and transdermal fentanyl patch. There were no differences in gender, type of cancer, metastasis, metastasis site, pain site, or pain intensity.
Conclusion: Pain was controlled in older patients by low dose morphine. To provide higher quality hospice care, doctors should pay more attention to quality of life of patients with an active narcotic analgesic regimen.
Keywords: Morphine dose, narcotic analgesics, hospice, cancer pain management, family medicine.
Received August 24, 2015 Revised August 24, 2015 Accepted September 11, 2015 Corresponding Author Seock-Hwan Lee
Tel: +82-53-560-7390, Fax: +82-53-560-7499 E-mail: [email protected]
Copyright © 2015 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
송은 외. 일개 종합병원 호스피스 병동에서 사용된 임종 일주일 전 마약성 진통제 용량 Korean Journal of Family Practice
KJFP
Original Article
Korean Journal of Family Practice
서는 마약성 진통제를 사용하도록 권고하였으나8) 최근에는 마약성 진통제를 모든 단계의 암성 통증에 적극적으로 사용하도록 권고하 고 있다.9)
이에 저자 등은 마약성 진통제 용량에 따른 말기 암환자의 인구 학적 특성과 임상적 특성, 약물종류, 마약성 진통제의 따른 심각한 부작용 발생 등의 차이가 있는지 조사하고자 하였다.
방 법
1. 연구대상
본 연구는
2014
년1
월부터2014
년12
월까지 대도시 일개 종합병 원 호스피스병동 입원환자를 대상으로 하였다.1
주일 이상 입원하 였다가 임종한 말기 암환자84
명을 대상으로 하였다.2. 연구방법
호스피스 병동 입원 시 담당의사가 보호자 혹은 본인과 면담하
여 호스피스 완화의료 기록지를 작성한 정보와 간호기록지 및 의무 기록지를 후향적 방법으로 분석하였다. 인구학적 자료에 성별, 나 이, 암 종류, 전이여부, 전이 암 부위, 재원기간, 일상수행능력을
ECOG
(Eastern Cooperative Oncology Group
)Performance Status
로 조사하였다. 임상적 자료에는 입원 시 통증위치, 입원 시 통증강 도, 입원 시 주 증상, 임종 전1
주일 동안 마약성 진통제 종류와 양,naloxone
양을 조사하였다. 통증강도는VAS
(Visual analog scales
) 로 측정하여 기록하였다.앞선 연구의 가이드라인10-11)에 따라 마약성 진통제 사용량을
OME
(Oral morphine equivalent
)로 환산하여 일일 평균200mg
미 만이면 중간용량군,200mg
이상400mg
미만이면 고용량군,400mg
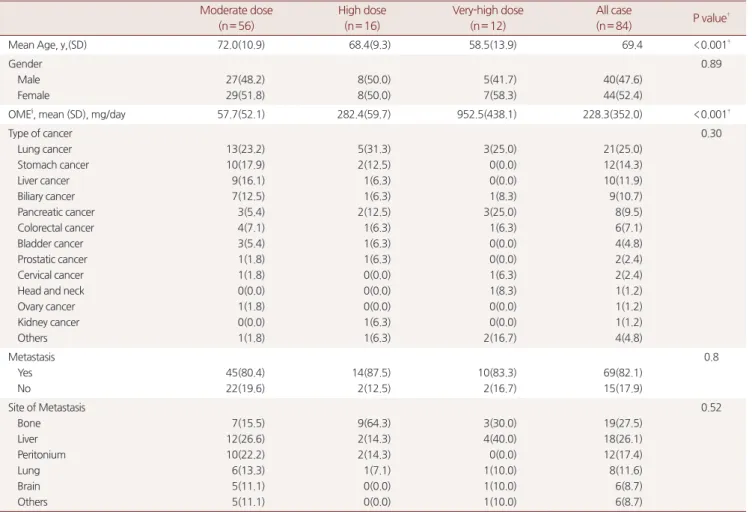
이상이면 초고용량군으로 나누어 비교하였다. 정규 처방 및 돌발성 통증시 처방된 마약성 진통제 모두를 포함하였다.Table 1. General characteristics of patients*
Moderate dose (n= 56)
High dose (n= 16)
Very-high dose (n= 12)
All case
(n= 84) P value†
Mean Age, y,(SD) 72.0(10.9) 68.4(9.3) 58.5(13.9) 69.4 <0.001‡
Gender Male Female
27(48.2) 29(51.8)
8(50.0) 8(50.0)
5(41.7) 7(58.3)
40(47.6) 44(52.4)
0.89
OME§, mean (SD), mg/day 57.7(52.1) 282.4(59.7) 952.5(438.1) 228.3(352.0) <0.001‡
Type of cancer Lung cancer Stomach cancer Liver cancer Biliary cancer Pancreatic cancer Colorectal cancer Bladder cancer Prostatic cancer Cervical cancer Head and neck Ovary cancer Kidney cancer Others
13(23.2) 10(17.9) 9(16.1) 7(12.5) 3(5.4) 4(7.1) 3(5.4) 1(1.8) 1(1.8) 0(0.0) 1(1.8) 0(0.0) 1(1.8)
5(31.3) 2(12.5) 1(6.3) 1(6.3) 2(12.5) 1(6.3) 1(6.3) 1(6.3) 0(0.0) 0(0.0) 0(0.0) 1(6.3) 1(6.3)
3(25.0) 0(0.0) 0(0.0) 1(8.3) 3(25.0) 1(6.3) 0(0.0) 0(0.0) 1(6.3) 1(8.3) 0(0.0) 0(0.0) 2(16.7)
21(25.0) 12(14.3) 10(11.9) 9(10.7) 8(9.5) 6(7.1) 4(4.8) 2(2.4) 2(2.4) 1(1.2) 1(1.2) 1(1.2) 4(4.8)
0.30
Metastasis Yes No
45(80.4) 22(19.6)
14(87.5) 2(12.5)
10(83.3) 2(16.7)
69(82.1) 15(17.9)
0.8
Site of Metastasis Bone Liver Peritonium Lung Brain Others
7(15.5) 12(26.6) 10(22.2) 6(13.3) 5(11.1) 5(11.1)
9(64.3) 2(14.3) 2(14.3) 1(7.1) 0(0.0) 0(0.0)
3(30.0) 4(40.0) 0(0.0) 1(10.0) 1(10.0) 1(10.0)
19(27.5) 18(26.1) 12(17.4) 8(11.6) 6(8.7) 6(8.7)
0.52
* Data are presented as number(%) unless otherwise indicated.
† P value from χ2 test for comparing a difference between 3 of the study group unless otherwise indicated.
‡ P value from one-way ANOVA(analysis of variance) test for comparing a difference of mean value between any of the 3 study groups
§ OME: oral morphine equivalent, Data source: National Opioid Use Guideline Group, Canadian Guideline for Safe and Effective Use of Opioids for Chronic Non-Cancer Pain. The midpoint of the fentanyl ranges was used in our conversions.
En Sung, et al. The narcotic analgesics in terminal cancer patients during the last 1 week to death
Korean Journal of Family Practice
KJFP
통 계
통계분석은
R 3
.1
.2 for window
로 검정하였으며 주 증상,ECOG grade
, 통증위치, 성별, 입원횟수, 주진단명, 말기상태인 식, 전이여부, 전이위치 등의 세 그룹간 차이는 교차분석인chi
-square test
로 검정하였고 나이, 재원기간, 통증강도, 약물용량 등 은One
-way ANOVA
(analysis of variance
)를 이용하여 검정하 였다. 나이, 재원기간이 증가함에 따른 모르핀 용량과의 상관관계 를Pearson
상관계수를 구하여 검정하였으며 통계학적 유의수준은P
-value
<0
.05
로 하였다.결 과
1. 일반적 특성
84
명의 대상자중 중간용량군이56
명(66
.7
%), 고용량군이16
명(
19
.0
%), 초고용량군이12
명(14
.3
%)이었다. 대상자의 평균 연령은69
.4
세(±11
.9
)였으며 중간용량군이72
.0
세(±10
.9
), 고용량군이68
.7
세(±9
.3
), 초고용량군이59
.6
세(±13
.9
)였으며 세 군간의 통 계적 유의한 차이를 보였다. 성별은 남자40
명(47
.6
%), 여자44
명 (52
.4
%)였으며 세 군간의 통계적 유의한 차이는 없었다(Table 1
).2. 임상적 특성
암의 종류는 폐암(
25
.0
%), 위암, 간암 순이었으며69
명(82
.1
%)에 서 전이가 확인 되었다. 전이 위치로는 뼈(27
.5
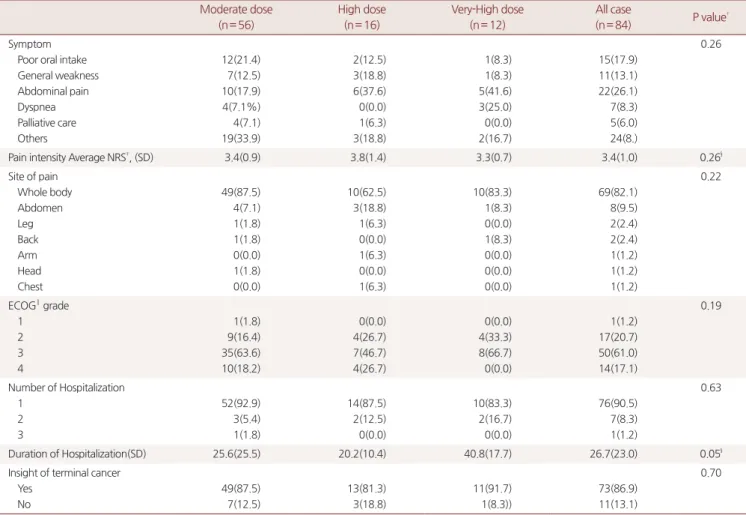
%), 간, 복막 순이었 다. 중간용량군에 비해 고용량군의 뼈 전이율이 높았지만 세 군간 의 통계적 유의한 차이는 없었다.입원 시 주로 호소한 증상은 통증(
26
.1
%), 식욕부진, 전신허약 순 이었다. 통증의 위치는 세 군 모두 전신통 호소가 많았으며 입원 시 통증의 강도는NRS
(Numeric rating scale
)로 중간용량군이3
.4
(±0
.9
), 고용량군이3
.8
(±1
.4
), 초고용량군이3
.3
(±0
.7
)이었으며 입Table 2. Clinical characteristics of patients*
Moderate dose (n= 56)
High dose (n= 16)
Very-High dose (n= 12)
All case
(n= 84) P value† Symptom
Poor oral intake General weakness Abdominal pain Dyspnea Palliative care Others
12(21.4) 7(12.5) 10(17.9) 4(7.1%) 4(7.1) 19(33.9)
2(12.5) 3(18.8) 6(37.6) 0(0.0) 1(6.3) 3(18.8)
1(8.3) 1(8.3) 5(41.6) 3(25.0) 0(0.0) 2(16.7)
15(17.9) 11(13.1) 22(26.1) 7(8.3) 5(6.0) 24(8.)
0.26
Pain intensity Average NRS‡, (SD) 3.4(0.9) 3.8(1.4) 3.3(0.7) 3.4(1.0) 0.26§
Site of pain Whole body Abdomen Leg Back Arm Head Chest
49(87.5) 4(7.1) 1(1.8) 1(1.8) 0(0.0) 1(1.8) 0(0.0)
10(62.5) 3(18.8) 1(6.3) 0(0.0) 1(6.3) 0(0.0) 1(6.3)
10(83.3) 1(8.3) 0(0.0) 1(8.3) 0(0.0) 0(0.0) 0(0.0)
69(82.1) 8(9.5) 2(2.4) 2(2.4) 1(1.2) 1(1.2) 1(1.2)
0.22
ECOG‖ grade 1 2 3 4
1(1.8) 9(16.4) 35(63.6) 10(18.2)
0(0.0) 4(26.7) 7(46.7) 4(26.7)
0(0.0) 4(33.3) 8(66.7) 0(0.0)
1(1.2) 17(20.7) 50(61.0) 14(17.1)
0.19
Number of Hospitalization 1
2 3
52(92.9) 3(5.4) 1(1.8)
14(87.5) 2(12.5) 0(0.0)
10(83.3) 2(16.7) 0(0.0)
76(90.5) 7(8.3) 1(1.2)
0.63
Duration of Hospitalization(SD) 25.6(25.5) 20.2(10.4) 40.8(17.7) 26.7(23.0) 0.05§
Insight of terminal cancer Yes
No
49(87.5) 7(12.5)
13(81.3) 3(18.8)
11(91.7) 1(8.3))
73(86.9) 11(13.1)
0.70
* Data are presented as number(%) unless otherwise indicated.
† P value from χ2 test for comparing a difference between 3 of the study group.
‡ NRS: numeric rating scale, ‡ECOG: eastern cooperative oncology group.
§ P value from one-way ANOVA(analysis of variance) test for comparing a difference of mean value between any of the 3 study groups.
‖ ECOG : Eastern Cooperative Oncology Group Performance Status.
송은 외. 일개 종합병원 호스피스 병동에서 사용된 임종 일주일 전 마약성 진통제 용량 Korean Journal of Family Practice
KJFP
원 시 증상, 입원 시 통증 위치, 입원 시 통증강도 모두 통계적 유의 한 차이는 없었다. 입원 시
ECOG Performance Status
는 모든 군 에서ECOG grade 3
이 가장 많았다. 초고용량군에서ECOG grade 2
(33
.3
%)의 비율이 높았지만 통계적 유의한 차이는 없었다.1
년 동 안의 입원횟수를 보면 대부분의 환자들이1
번(90
.5
%)입원하였으며 재원기간은 초고용량군이40
.8
일(±17
.7
)로 가장 길게 입원하였으 나 세 군간의 통계적 차이는 없었다(Table 2
).3. 1주일 동안 사용된 마약성 진통제 종류와 용량
대상자의 평균
OME
용량은228
.3mg
(±352
.0
)이었으며 중간용 량군은57
.7mg
(±52
.1
), 고용량군은282
.4mg
(±59
.7
), 초고용량 군이952
.5mg
(±438
.1
)였다.1
주일 동안 사용된 마약성 진통제 종류로morphine parenteral
,transdermal fentanyl patch
,oxycodone PO
(per oral
),Meperidine PO
,Oxycodone HCL controlled release PO
,codein PO
,hydromorphone PO
가 처방되었다.Morphine parenteral
은 대상자 중75
명,Transdermal fentanyl patch
는76
명으로 빈도가 가장 높았으며Oxycodone PO
(per oral
) 는 총7
명,Meperidine PO
는3
명,Oxycodone HCL controlled release PO
는 총4
명,codeine PO
는 총5
명,hydromorphone PO
는 총4
명에게 처방되었다.연령과
OME
용량은Pearson
상관계수가 -0
.36
으로 뚜렷한 음 의 상관관계를 보였으며 재원기간과 상관관계는 통계적으로 유의 하지 않았다(Table 4
).고 찰
마약성 진통제 투여는 말기 암 환자의 고식적 치료에서 중요한 부분을 차지한다. 하지만 환자 스스로 마약성 진통제 투여의 두려
움으로 인한 마약성 진통제 투여의 제한, 처방하는 의사들의 마약 성 진통제 투여에 대한 부정적인 태도에 의해 치료 용량에 미치지 못하며 통증조절을 실패하게 된다.
마약성 진통제는 천장용량이 없다고 알려져 있으며 충분히 효과 가 나타날 때까지 투여 용량의 증가가 가능하며, 지속적인 고용량 투여가 가능하다. 특히 말기 암환자에게서 통증 조절을 위한 고용 량의 투여로는 중독이 잘 발생하지 않는다고 알려져 있다.12) 지금까 지 알려진 마약성 진통제에 의한 부작용으로는 정신혼미, 오심, 구 토, 변비 호흡억제, 수면장애 등이 있으며 가장 심각한 부작용은 호 흡억제이다. 하지만 말기 암 환자는 통증이 중추신경계를 자극함으 로 호흡억제가 잘 발생하지 않는다.13) 본 연구의 대상자중 마약성 진통제의 부작용인 호흡감소로 인해
naloxone
을 사용한 경우는1
명이었다. 고용량을 사용한 환자에게서 발생한 것이 아니라 중간용 량 환자에게서 발생 한 것이었다. 본 연구에서는 통계적으로 유의 한 결과는 없었으나, 고용량 처방이 심각한 호흡저하와 관련이 없 었다.마약성 진통제 중에서 말기 암환자에게 임종 전 가장 많이 처방 된 약제는
morphine
과fentanyl
이라고 발표한 적 있으며 본 연구 에서도 결과는 같았다.14-15) 세계보건기구에서 중등도 이상의 통증 에 경구 마약성 진통 제제를 권하였으나 본 연구 결과에서는 경구 투여보다 주사제 투여가 많았다.Transdermal fentanyl
은 다른 약제 에 비해 변비의 발생이 줄었으며 연하장애가 있는 환자들에게도 사 용 가능하다는 장점이 있어 치료의 순응도를 높인다고 하였다.16) 임 종1
주일 전 의식 수준은 확인 하지 않았지만 본 연구의 대상자들 의 임상적 상태가 경구투여보다는 주사제 혹은 경피형 형태의 약물 이 순응도가 더 높았을 가능성이 있겠다. 이는 임종에 가까워지면 서 식욕이 급격히 떨어지고 경구투여가 힘들어지며 의식상태가 떨 어지는 것과 관련이 있어 보인다.17-18)병의 이환 기간 및 입원기간이 길수록 마약성 진통제 요구량은 증가되며, 이는 마약성 진통제 투여 시 발생하는 내성과 관련이 있 는 것으로 보이나 본 연구에서는 재원기간과
OME
용량과 상관성 이 없었다.19) 말기 암 환자들의 통증 치료 시 나이가 적을수록 더 적 극적인 마약성 진통제 투여가 필요하다.20-21) 본 연구에서도 나이와OME
용량과는 음의 상관관계를 가졌다. 이는 노인의 경우 동반된 다른 질환 및 나이 증가에 따른 콩팥, 간 기능이 저하된 상태로 약물 Table 3. Narcotic analgesics typeN OME*, median(SD), mg/week
Morphine parenteral 75 258.4(349.6)
Transdermal fentanyl patch 76 961.9725(1942.873)
Oxycodone PO‡ 7 240.0(491.0)
Oxycodone HCL controlled
release PO 4 390.0(333.2)
Meperidine PO 3 791.6(1220.2)
Codeine PO 5 292.0(173.1)
Hydromorphone PO 4 1110.0(1105.8)
* OME: Oral morphine equivalent, Data source: Notional Opioid Use Guideline Group, Canadian Guideline for Safe and Effective Use of Opioids for Chronic Non-Cancer Pain. The midpoint of the fentanyl ranges was used in our conversions.
‡ PO: Per oral.
Table 4. Correlation OME* and change of age and duration of hospitalization
OME P value†
Age - 0.360 0.001
Duration of Hospitalization 0.157 0.15
* OME: oral morphine equivalence
† P values were calculated by Pearson correlation coefficient analysis.
En Sung, et al. The narcotic analgesics in terminal cancer patients during the last 1 week to death
Korean Journal of Family Practice
KJFP
의 대사와 배설이 감소하여 마약성 진통제로 통증 조절이 가능하다 는 것으로 제시한 보고와 관련이 있다.22)
본 연구의 제한 점으로 대상자들의 입원 시 상급종합병원에서 전 원 되어 통증치료를 받고 있었던 경우가 많았기 때문에 통증이 과소 평가 되었을 가능성이 있다는 것이다. 통증은 신체적 요인 뿐만 아 니라 정서적 사회적 경제적 영적 요인들의 영향을 받고 개인마다 통 증을 느끼는 정도가 다를 수 있으며, 의식수준이 떨어지면서 입원 시 증상 호소가 줄었기 때문에 낮은 점수로 확인되었을 가능성이 있 다. 그리고 전체 대상자에서
NRS
가3
.49
(+-1
.05
)로 측정되었는데 이는 국내의 한 연구에서도 말기 암 환자 들의 평균NRS
는3
.6
점과 비슷한 결과를 나타냈다.23)부작용의 지표로서
naloxone
사용만을 조사하였기 때문에 경한 호흡억제가 일어난 경우와 그 밖에 부작용의 발생 및OME
용량과 의 관계에 대해서는 알 수 없었다.마지막으로 대도시 소재의 일개 종합병원을 대상으로 하였고, 다른 기관 및 다른 의사들의 약물 처방력을 고려하지 않아 결과를 일반화 할 수는 없을 것이다. 그리고 정규 처방과 돌발성 통증 시 처방을 따로 조사하지 못하여 치료가 적절하였는지 여부는 알 수 없었다.
호스피스의 치료를 효과적으로 받기 위해 적어도 임종
3
개월 전 에 등록하는 것이 중요하나, 대부분의 대상자들은 임종 직전에 입 원을 하며, 그 시점과 동시에 호스피스에 등록되었다.2004
년 국내 일개 병원에서의 ‘말기 암 환자의 임상적 고찰’ 과 유사한 결과이며10
년이 지났지만 여전히 호스피스에 대한 사회 전반적인 인식이 낮 음을 알 수 있다.24) 이는 앞으로 환자와 가족 뿐만 아니라 의료인도 호스피스의 인식변화를 위해 적극적인 교육이 필요할 것으로 사료 된다.본 연구에서 말기 암 환자들의 마약성 진통제 용량에 따른 임상 양상은 큰 차이가 없었다. 다만 나이가 많은 환자들은 주의가 필요 하다. 본 연구에서는 용량에 따른 임상양상뿐 만 아니라 마약성 진 통제 종류도 분석할 수 있었다. 이러한 연구가 향후 말기암 환자의 통증 조절에 대한 치료의 미미한 도움이 될 것으로 생각된다. 결론 적으로 의료진은 조금 더 적극적인 마약성 진통제 처방이 필요하 며, 마약성 진통제 오해에 대한 교육을 통해 환자 및 보호자들의 마 약성 진통제에 대한 심리적 장벽을 낮추도록 노력하여, 말기 암 환 자들의 삶의 질의 개선에 도움이 될 수 있도록 하여야 할 것이다.
요 약
연구배경: 의료진들의 마약성 진통제의 편견이 말기 암환자들의 불 충분한 통증관리에 영향을 미쳐왔다. 이에 본 저자들은 말기 암 환 자들의 임종
1
주일 전morphine
사용 실태 조사를 하여morphine
용량에 따른 차이가 있는지 알아보고자 하였다.
방법:
2014
년1
월1
일부터2014
년12
월31
일 까지 대도시 소재 일개 종합병원 호스피스 병동에1
주일 이상 입원하였다가 임종 한 말기 암 환자84
명을 대상으로morphine
용량을OME
(Oral morphine equivalent
)로 환산하여200mg
/day
미만이면 저용량군,200mg
/day
이상400mg
/day
미만이면 중간용량이군,400mg
/day
이상이면 고용량군으로 나누어 세 군간의 인구학적 특성, 임상학적 특성, 마약성 진통제 종류,naloxone
처방 등의 차이를chi
-square
및one way ANOVA
로 검정하였으며OME
용량에 따른 나이, 재원 기간의 상관관계를Pearson
상관계수를 이용하여 검정하였다.결과: 나이와
OME
용량과는 음의 상관관계를 가졌으며 고용량군이morphine parentral
과trans fentanyl patch
가 처방의 빈도가 높았 다. 세 군간의 성별, 암의 종류, 전이 부위, 통증 강도, 통증위치 등 은 차이가 없었다.결론: 나이가 많을수록 적은 용량의
morphine
으로 통증 조절이 가 능하였다. 의료진은 조금 더 적극적인 마약성 진통제 처방을 통해 환자의 삶의 질에 많은 관심을 가져야겠다.중심단어: 모르핀 용량, 마약성 진통제, 호스피스, 암성통증관리, 가정의
REFERENCES
1. National Cancer Registry statistics. [updated 2015 Jan 7]. Korea Central Cancer Registry; [cited 2015 Jan 15]; P. 3-42. Available from: http://www.cancer.go.kr/ebook/104/PC/104.html.
2. Park JM. Cancer pain. In: Korean Society of Anesthesiologists.
Anesthesiology & pain medicine. 2nd ed. Seoul: Ryo Moon Gak;
2010. p. 379-98.
3. Caraceni A, Cherny N, Fainsinger R, Kaasa S, Poulain P, Radbruch L, et al. Pain measurement tools and methods in clinical research in palliative care: recommendations of an Expert Working Group of the European Association of Palliative Care. J Pain Symptom Manage 2002; 23: 239-55.
4. Van den Beuken-van Everdingen MH, de Rijke JM, Kessels AG, Schouten HC, van Kleef M, Patijn J. Prevalence of pain in patients with cancer: a systematic review of the past 40 years. Ann Oncol 2007;18:1437-49.
5. Deandrea S, Montanari M, Moja L, Apolone G. Prevalence of undertreatment in cancer pain. A review of published literature.
Ann Oncol 2008; 19: 1985-91.
6. Young Ho Yun, Sang Min Park, Ki heon Lee, Ki Young Son, So Yeon Chung, Dae Seog Heo et al. Knowledge and Attitudes of Family Physician and Oncologist toward Cancer Pain Management in Korea. J Korean Acad Fam Med 2005; 26: 397-403.
송은 외. 일개 종합병원 호스피스 병동에서 사용된 임종 일주일 전 마약성 진통제 용량 Korean Journal of Family Practice
KJFP
7. Morita T, Tsunoda J, Inoue S, Chihara S. Effects of high dose opioids and sedatives on survival in terminally ill cancer patients. J Pain Symptom Manage 2001; 21: 282-9.
8. Ventafridda V, Saita L, Ripamonti C, De Conno F. WHO guidelines for the use of analgesics in cancer pain. Int J Tissue React 1985; 7:
93-6.
9. National Comprehensive Cancer Network. NCCN clinical practice guideline in oncology: adult cancer pain. Fort Washington:
National Comprehensive Cancer Network, 2012; volume 1.
10. Chou R, Fanciullo GJ, Fine PG, Adler JA, Ballantyne JC, Davies P, et al. Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J Pain 2009;10(2):113–130.
11. National Opioid Use Guideline Group. Canadian Guideline for Safe and Effective Use of Opioids for Chronic Non-Cancer Pain.
Hamilton (ON): McMaster University National Pain Centre; 2010.
12. Young Jin Yuh, MD. Opioid Use in Pain. Journal of Pain and Autonomic Disorders, Volume 2, No.2, 2013 Dec.
13. Borgbjerg FM, Nielsen K, Franks J. Experimental pain stimulates respiration and attenuates morphine-induced respiratory depression: a controlled study in human volunteers. Pain 1996; 64:
123-8.
14. Hye Ran Lee, Seong Yoon Yi, Do Yeun Kim. Evaluation of Prescribing medications for Terminal Cancer Patients near Death;
Cancer Research Treatment. 2013; 45(3): 220-225.
15. Ro You-Ja, Kim Nam-cho, Hong Young-sun, Yong Jin-Sun.
Factors Influencing Pain with Terminally Ill Cancer Patients in Hospice Units. Journal of Korean Academy of Nursing. 2001; 31:
206-20.
16. Slover R : Transdermal fentanyl ; Clinical trial at the University of
Colorado Health Science Center. J Pain Symptom Manage 1992; 7;
S45-7,
17. Lichter I, Hunt E. The last 48 hours of life. J Palliat Care.1990; 6:
7-15.
18. Sim YS, Kim DY, Nam EM, Lee SM. Symptom experience in terminal cancer patients during the last 48 hours of life. Korean J Hosp Palliat Care. 2007; 10: 190-4.
19. Coyle N, Adelgardt J, Foley KM. Disease progression and tolerance in the cancer pain patient. 2nd international Congress on Cancer Pain. J pain Symptom Manage 1988; 3(Suppl): 25.
20. Fainsinger R, Nekolaichuk C, Lawlor P, Neumann C, Hanson J, A multicenter study of the revised Edmonton Staging System for classifying cancer pain in advanced cancer patients. J Pain Symptom Manage. 2005; 29: 224-37.
21. Knudsen AK, Brunelli C, Klepstad P, Aass N, Apolone G, Corli O, et al. Which domains should be included in a cancer pain classification system? Pain. 2012; 153: 696-703.
22. Owen JA, Sitar DS, Berger L, Browell N, Duke PC, Mitenko PA.
Age-related morphine kinetics. Clin pharmacol Ther 1983; 34:
364-8.
23. Seok Hoon Kang, Ha Young Lee, Jun Su Kim, Jung Kwon Lee, Hwa Kyung Jung. Home-based Hospice-palliative Care Service Administered by University-based Family Practice. J Korean Acad Fam Med 2006; 27: 889-94.
24. Do Ho Moon, Wha Sook Choe, Myung Ah Lee, In Sook Woo, Jin Hyoung Kang, Young Seon Hong et al. Clinical considerations about terminally ill cancer patients who died in hospice unit. Korean Journal of Medicine 2004; 67: 341-8.