2008;22:8-12 □
종 설
□8
책임저자:양철우, 서울시 서초구 반포동 505
가톨릭대학교 의과대학 내과학교실, 137-040 Tel: 02-590-2527, Fax: 02-536-0323
E-mail: [email protected]
감작된 환자의 신장이식
가톨릭대학교 의과대학 강남성모병원 장기이식센터 윤 혜 은ㆍ양 철 우
Renal Transplantation in Highly Sensitized Re- cipients
Hye Eun Yoon and Chul Woo Yang
Transplantation Center, Kangnam St. Mary’s Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea
Sensitized patients have a reduced chance of receiving a crossmath-negative organ, because of the presence of anti- bodies against a variety of human leukocyte antigen (HLA).
There have been much attention and understanding on renal transplantation in sensitized patients, which led to attempts to remove alloantibodies and successful transplantation.
Therefore, a positive crossmatch test and the presence of donor-specific anti-HLA antibodies are no longer a contrain- dication to renal transplantation. These desensitization protocols include intravenous immunoglobulin (IVIG), plasmapheresis (PP), and rituximab. IVIG therapy is performed in two forms, high dose IVIG and low dose IVIG in combination with PP.
Rituximab is usually utilized in combination with IVIG the- rapy. Here we summarized the characterisitics of these strategies. (J Korean Soc Transplant 2008;22:8-12)
Key Words: Desenstization, Intravenous immunoglobulin, Plas-
mapheresis, Rituximab, Renal transplantation 중심 단어: 탈감작치료, 면역글로불린, 혈장반출법,
Rituximab, 신이식
서 론
면역학적으로 감작된 환자들(highly sensitized patients)은 신이식 전 교차반응검사를 통하여 양성으로 진단된 환자 또는 항HLA 항체가 고역가로 존재하는 환자(high panel reactive antibodies; high PRA)로 정의한다. 이러한 환자들은
이식 시 초급성 거부반응의 발생 위험이 높은 고위험군으 로 간주되어 일반적으로 이식이 금기 시 되어왔고, 광범위 한 HLA에 대한 감작으로 인해 교차반응 음성의 장기를 수 여 받을 기회가 감소하여 이식대기 시간이 장기화되었다.
그러나 최근 10년간 이 분야에 대한 관심이 증가되어 있는 데 그 이유는 항HLA 항체에 대한 측정방법의 향상, 항체매 개성 거부반응의 기전에 대한 이해 증가와 진단방법의 발 전, 강력하고 안전한 면역억제제의 도입 및 항체의존성거 부반응에 대한 효과적인 항 거부반응 치료법의 개발 등이 다. 감작된 환자에서는 이식을 가능하게 하기 위한 탈감작 치료(desensitization)가 시행되는데 실제로 이를 통해 면역 학적 한계를 극복한 성공적인 이식성적이 많이 보고되고 있다. 탈감작을 위한 접근은 항HLA IgG 항체의 제거 또는 중화, 신이식 전 새로운 항HLA IgG 항체의 형성 예방, 교차 반응이 음성일 때 신이식 시행, 이식 후 새로운 항HLA IgG 항체의 형성 예방 및 급성 항체매개성 거부반응의 발생에 대한 신속한 진단과 치료로 이루어진다. 탈감작치료로 크 게 두 가지의 방법, IVIG (intravenous immunoglobulin)과 혈 장반출법(plasmapheresis)이 사용된다. IVIG는 고용량으로 투여하는 프로토콜(1-6)과 혈장반출법과 병행하여 저용량 으로 투여하는 프로토콜(1,7-11)로 나뉘는데, 이 두 치료법 을 비교한 무작위 대조 연구는 현재까지 없다. 또한 일부에 서는 이식 전후로 단핵구성 항CD20 항체인 rituximab을 병 합 투여함으로써 이들 환자의 이식 기회를 증대시키고 있 다.(1,10,12)
본 론
1) 고용량의 IVIG 투여를 통한 탈감작 포로토콜
고용량의 IVIG가 항체매개성 거부반응을 예방하는 기전
은 현재까지 확실히 알려져 있지 않으나 일반적으로, 단핵
구의 Fc수용체의 차단,(13,14) alloantibody에 대한 직접적인
중성화(anti-idiotypic effects),(15,16) 활성화된 B임파구의 CD19
에 대한 발현 억제(13) 및 보체와 alloreactive T임파구의 억
제(13,14,17)의 기전이 제시되고 있다. 고용량의 IVIG를 투
여하는 횟수는 프로토콜마다 다르지만, 대부분 2 g/kg의 용
량으로 주며 3∼7 차례 투여하고 있다.(1-6) 대표적인 프로
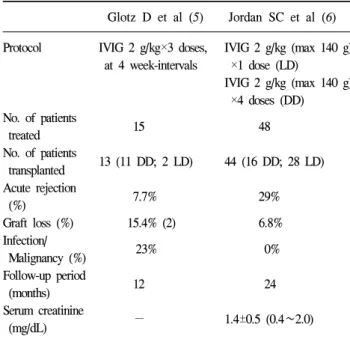
토콜을 소개하면 Table 1과 같다. 위의 두 보고에서의 결과
Table 1. Desensitization protocols based on high dose IVIG
Glotz D et al (5) Jordan SC et al (6) Protocol IVIG 2 g/kg×3 doses, IVIG 2 g/kg (max 140 g)
at 4 week-intervals ×1 dose (LD)
IVIG 2 g/kg (max 140 g) ×4 doses (DD) No. of patients
15 48 treated
No. of patients
13 (11 DD; 2 LD) 44 (16 DD; 28 LD) transplanted
Acute rejection
7.7% 29%
(%)
Graft loss (%) 15.4% (2) 6.8%
Infection/
23% 0%
Malignancy (%) Follow-up period
12 24 (months)
Serum creatinine
− 1.4±0.5 (0.4∼2.0) (mg/dL)
DD = deceased donor; LD = living donor.
Table 2. Desensitization protocols based on plasmapheresis Montgomery RA, Schweitzer EJ,
et al(7) et al(9)
Protocol PP/IVIG until MMF prior to PP, crossmatch (−)
MP 500 mg/day IVIG ×7 doses ×3 doses (total 500 mg/kg),
FK and corticosteroid started with first PP, PP (thrice/week) ×2 weeks before transplant No. of patients
4 15 treated
No. of patients
4 11 transplanted
Acute rejection
100% 36.4%
(%)
Graft loss (%) 0% 0%
Infection/
−/− 9.1%
Malignancy (%) Follow-up period
10 (4.3∼17) 13.3±2.4 (3∼26) (months)
Serum creatinine
1.0 (0.8∼1.2) 1.6±0.2 (1.1∼2.4) (mg/dL)
PP = plasmapheresis; MP = methylprednisolone; FK = tacrolimus.
에서 보듯이 고용량의 IVIG의 성적은 감작된 환자의 치료 에 비교적 효과적으로 여겨지나 아직까지 장기간의 이식신 성적에 대하여서는 확실치 않다. 고용량의 IVIG는 비교적 면역억제 기능이 적고 투여하기 용이하며 독성이 적은 장 점이 있지만, 그 효과를 예측하기가 어렵고, 부작용이 또한 문제이다. IVIG 투여와 관련된 부작용의 빈도는 12∼23%로 보고되고 있는데, 가장 흔한 부작용으로 고열, 오한, 심한 두통, 근육통, 흉통 등이 있으며 아나필락시스, 혈전증, 신 독성 등의 심각한 부작용도 보고되고 있다.(18,19)
2) 혈장반출을 이용한 탈감작 프로토콜
혈장반출에 기초한 프로토콜은 여러 연구자들이 발표하 였으며 기본적인 프로토콜은 비슷하다. 혈창반출법을 이용 하며 항HLA 항체를 제거한 직후 저용량의 IVIG를 투여한 다. IVIG의 용량과 횟수는 프로토콜마다 다르지만 대부분 100 mg/kg의 용량을 3∼8회로 투여한다.(1,7-11,20) 혈장반 출을 시작함과 동시에 tacrolimus, mycophenolate mofetil (MMF) 및 스테로이드 투여를 병행하는데, 이는 항HLA 항 체의 재형성을 제한하기 위함이다. 혈장반출은 주 3회 시행 하고 그 횟수는 T임파구 교차반응이 음전할 때까지 시행하 며 음전이 되면 24시간 이내에 이식을 시행한다. 혈장반출 후 항HLA 항체가 반동으로 생성될 수 있기 때문에 혈장반 출 직후 저용량의 IVIG를 투여함으로써 항체를 제거한다.
교차반응 검사가 음성으로 전환되기 위해 필요한 혈장반출 횟수는 치료 전 혈청 내 존재하는 공여자 특이항체 (donor- specific antibody, DSA)의 역가에 따라 다르다. 이전 보고에
서는 이식 전 최소 3회에서 최대 6회까지 시행하였으며(1, 7,9,10,11) 이식 후에 추가로 PP를 시행하기도 하였다.(10) 대표적인 프로토콜은 Table 2와 같다. 이와 같이 혈장반출 법은 치료효과가 우수하고 비교적 환자들이 잘 적응하며 교차반응의 음전 시기를 어느 정도 예측할 수 있는 장점이 있지만, 비용이 고가이고 혈장반출 치료를 위한 인력이 필 요한 단점이 있다. 또한 혈장반출 시 알부민, 면역글로불린, 응고인자 등이 제거될 수 있기 때문에 저칼슘혈증, 출혈경 향이 발생 할 수 있고, 혈장반출 시 대치하는 수액으로 인한 고열 또는 오한이 발생할 수 있다.(21)
3) 탈감작된 환자들의 이식 후 면역억제요법 탈감작치료를 시행하고 신장이식을 시행할 때 대부분의 면 역억제요법은 항임파구 항체를 이용한 induction therapy와 MMF, tacrolimus 및 스테로이드의 병합치료를 선호한다.
Induction therapy는 과거에 OKT3를 많이 사용하였으나,
cytokine의 방출로 인한 부작용(발열, 두통, 복통, 저혈압, 폐부
종 등)으로 인하여 사용이 많이 감소하였다.(22) 이에 대신하여
다클론 항임파구 제제와 단클론 IL-2 수용체항체를 많이 사용
하고 있다.
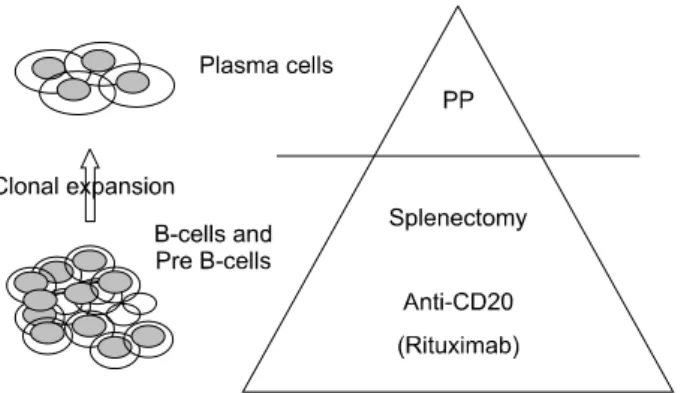
Fig. 1. B cell targeting therapy in renal transplantation.
4) Anti CD20 antibody (rituximab)의 신이식에서의 역할
Rituximab은 chimeric 단클론 항 CD20 항체이다. 작용기 전을 간단히 요약하면 첫째 항체 의존성 세포매개성 세포 독성(antibody dependent cell mediated cytotoxicity: ADCC), 둘째, 보체 의존성 세포독성(complement dependent cyto- toxicity, CDC), 셋째, 세포자멸(apoptosis)에 의한 B 임파구 의 파괴이다.(23) 현재까지 악성임파종과 자가면역질환에 제한적으로 투여되었으나 ABO 혈액형의 불일치 장기이식 및 항체매개성 거부반응의 치료에까지 범위가 확대되고 있 다. (1,10,12,20,24,25)
항체매개성 거부반응의 예방에 rituximab를 투여하는 이 론적 근거는 다음과 같다. 이미 나열한 탈감작치료 방법들 (IVIG, 혈장반출)은 이미 형성된 항HLA 항체를 제거하는 방법이다. 따라서 신이식 후 B임파구 전구세포에 의하여 새로이 생성되는 항HLA 항체에 의한 항체매개성 거부반응 을 예방할 수 없다. CD20은 B임파구 전구세포의 표면에도 발현하고 있으므로, rituximab을 투여함으로써 이식 후 memory B임파구에 의한 항HLA 항체 생성을 억제시키기 위함이다.(23) Fig. 1은 감작된 환자의 신이식에 있어 B임파 구를 제거하는 치료의 이론적 근거를 나타낸 것이다. 비장 적출도 이 같은 목적으로 시행되긴 하였으나, 비장적출 후 발생하는 패혈증의 위험, 특히 면역억제제를 함께 복용하 는 신이식 환자의 특성을 고려할 때 rituximab이 보다 안전 하다고 하겠다.(26,27)
Rituximab의 투여시 그 용량과 시기에 있어서는 아직 정 립된 바가 없다. 말기 신질환의 환자에서 rituximab의 반감 기는 9∼14일이고,(28) 1회 투여로 항체 생성을 예방하기에 충분하다고 보고되고 있다.(29) 그러나 최근 교차반응 양성 인 환자의 신이식에서 rituximab을 투여함에도 불구하고 항 체매개성 급성거부반응으로 인한 이식신 소실을 경험한 예 가 보고되고 있다.(30) 이를 설명하는 근거로는 rituximab 1 회 투여가 림프장기에 존재하는 잔여 B임파구를 제거하기
에는 부족하고,(28,30,31) germinal center에 존재하는 B임파 구는 말초혈액에 있는 B임파구보다 항CD20 치료에 덜 반 응하며,(32) 형질세포에는 CD20의 발현이 적어 rituximab의 치료에 반응하지 않아 항체생성을 완전히 막을 수 없다는 (33) 점이다.
Rituximab의 투여에 있어서 고려해야 할 다른 점은 공여 자 특이 항HLA 항체(donor specific antibody, DSA)의 측정법 이다. Rituximab은 보체 활성화를 일으킴으로써 ADCC에 관여할 수 있기 때문에 전통적인 임파구 교차반응 검사인 보체 의존성 세포독성법(complement-dependent cytotoxicity, CDC)의 결과에 혼선을 줄 수 있다. 또한 rituximab의 human Fc 부분이 임파구 표면과 결합함으로써 유세포분석기를 이 용한 교차시험(flow cytometry, FCXM)가 위양성을 보일 수 있다.(34) Rituximab을 교차반응 검사 시 제거하기 위한 방 법들이 고안되었지만(8,35,36) 검사를 위한 추가적인 노력 이 필요하고 결과 해석에 다른 영향을 줄 수 있다. 따라서 이 경우 혈청 내의 항HLA 항체만 특이적으로 검출하는 solid phase ELISA 방법에 의한 교차반응 검사가 가장 적합하다.
(10,34,37)
5) 탈감작치료에 있어 고려해야 할 사항
탈감작치료를 시행하기 이전에 이식 후 급성 항체매개성 거부반응의 발생 위험도를 평가하는 것이 중요하다. 교차 반응 양성인 경우, 양성 결과를 보인 횟수 및 시기, 검사방 법의 종류(CDC 또는 FCXM)에 따라 항체매개성 거부반응 발생 위험이 다르기 때문이다. 예를 들어 현재 CDC에 의한 교차반응 양성인 경우의 거부반응 발생 위험이 매우 높은 반면에 과거에 FCXM에 의한 교차반응 양성인 경우의 위험 은 더 낮다.(38) 또한 이전에 감작된 과거력, 즉 수혈, 이식, 재이식에 대한 정보를 파악하여 탈감작치료 후 다시 DSA 가 생성될 가능성을 염두하여야 한다. 탈감작치료 이후로 혈중 내 DSA 여부를 정기적으로 감시하는 것 또한 중요하 다. 탈감작치료에 의해 항체가 효과적으로 제거되었는지를 확인 후 이식을 시행해야 하며, 특히 이식 후 초기에 DSA의 재형성 여부를 진단하여 적기에 추가적인 항체제거 치료를 하는 것이 항체매개성 거부반응에 의한 이식신 소실을 예 방할 수 있기 때문이다.
결 론
교차반응 양성 또는 혈중 항HLA 항체의 존재가 이제 더
이상 이식의 금기가 아님은 확실하며, 탈감작치료는 많은 환
자들에게 신이식의 기회를 증대시킬 것이다. 앞서 나열한 탈
감작치료에 의한 신이식 성적이 양호하긴 하나 탈감작치료에
대한 현재까지의 보고는 많은 제약을 가지고 있다. 이를 요약
하면 첫째, 대부분의 발표된 논문이 무작위 비교연구가 되어
있지 않아 그 치료 효과에 대한 객관성이 결여되어 있으며
둘째, 고비용이 들며 셋째, 강한 면역억제요법로 인한 BK virus nephropathy, 전신감염 및 종양의 발생빈도가 증가하며, 넷째, 현재까지 장기간의 추적 결과가 없어 이식 후 얼마나 오랜 기간 동안 효과적으로 항HLA 항체 생성을 억제할 수 있는가와 탈감작치료를 받은 환자들의 장기간의 생존율에 대 한 보고가 미비하다는 점 등이다. 따라서 이러한 점을 고려하 여 탈감작치료 여부를 결정해야 할 것이다.
REFERENCES
1) Stegall MD, Gloor J, Winters JL, Moore SB, DeGoey S. A comparison of plasmapheresis versus high-dose IVIG desensi- tization in renal allograft recipients with high levels of donor specific alloantibody. Am J Transplant 2006;6:346-51.
2) Jordan SC, Vo AA, Peng A, Toyoda M, Tyan D. Intravenous gammaglobulin (IVIG): a novel approach to improve transplant rates and outcomes in highly HLA-sensitized patients. Am J Transplant 2006;6:459-66.
3) Vo AA, Toyoda M, Peng A, Bunnapradist S, Lukovsky M, Jordan SC. Effect of induction therapy protocols on transplant outcomes in crossmatch positive renal allograft recipients desensitized with IVIG. Am J Transplant 2006;6:2384-90.
4) Jordan SC, Tyan D, Stablein D, Mcintosh M, Rose S, Vo A, Toyoda M, Davis C, Shapiro R, Adey D, Milliner D, Graff R, Steiner R, Ciancio G, Sahney S, Light J. Evaluation of intravenous immunoglobulin as an agent to lower allosensi- tization and improve transplantation in highly sensitized adult patients with end-stage renal disease: report of the NIH IG02 trial. J Am Soc Nephrol 2004;15:3256-62.
5) Glotz D, Antoine C, Julia P, Suberbielle-Boissel C, Boudjeltia S, Fraoui R, Hacen C, Duboust A, Bariety J. Desensitization and subsequent kidney transplantation of patients using intravenous immunoglobulins (IVIg). Am J Transplant 2002;2:
758-60.
6) Jordan SC, Vo AA, Bunnapradist S, Toyoda M, Peng A, Puliyanda D, Kamil E, Tyan D. Intravenous immune globuliln inhibitis crossmatch positivity and allows for successful trans- plantation of incompatible organs in living donor and cadaver transplant recipients. Transplantation 2003 76: 631-36.
7) Montgomery RA, Zachary AA, Racusen LC, Leffell MS, King KE, Burdick J, Maley WR, Ratner LE. Plasmapheresis and intravenous immune globulin provides effective rescue therapy for refractory humoral rejection and allows kidneys to be successfully transplanted into cross-match-positive recipients.
Transplantation 2000;70:887-95.
8) Zachary AA, Montgomery RA, Ratner LE, Samaniego-Picota M, Haas M, Kopchaliiska D, Leffell MS. Specific and durable elimination of antibody to donor HLA antigens in renal- transplant patients. Transplantation 2003;76:1519-25.
9) Schweitzer EJ, Wilson JS, Fernandez-Vina M, Fox M, Gutierrez M, Wiland A, Hunter J, Farney A, Philosophe B,
Colonna J, Jarrell BE, Bartlett ST. A high panel-reactive antibody rescue protocol for cross-match-positive live donor kidney transplants. Transplantation 2000;70:1531-6.
10) Gloor JM, DeGoey SR, Pineda AA, Moore SB, Prieto M, Nyberg SL, Larson TS, Griffen MD, Textor SC, Velosa JA, Schwab TR, Fix LA, Stegall MD. Overcoming a positive crossmatch in living-donor kidney transplantation. Am J Transplant 2003;3:1017-23.
11) 주동진, 김명수, 안형준, 주만기, 전경옥, 김현정, 김순일, 김유선. 혈장사혈과 감마글로브린으로 림프구 교차반응 음성전환 후 시행한 신장이식의 1년 이상 추적결과. 대한 이식학회지 2006;20:207-12.
12) Magee CC, Mah H, Tinckam K, Wood I, Ji F, Powelson J.
Successful living donor kidney transplantation across HLA and ABO incompatibilities. Nephrol Dial Transplant 2007;22:
602-4.
13) Toyoda M, Pao A, Petrosian A, Jordan SC. Pooled human immune globulin modulates surface molecule expression and induces apoptosis in human B-cells. Am J Transplant 2003;
3:156-66.
14) Andersson U, Bjork L, Skansen-Saphir U, Andersson J. Pooled human IgG modulates cytokine production in lymphocytes and monocytes. Immunol Rev 1994;139:21-42.
15) Kazatchkine MD, Kaveri SV. Immunomodulation of autoi- mmune and inflammatory diseases with intravenous immune globulin. N Eng J Med 2001;345:747-55.
16) Jordan SC, Quartel AW, Czer LS, Admon D, Chen G, Fishbein MC, Schweiger J, Steiner RW, Davis C, Tyan DB.
Post transplant therapy using high-dose human immunoglo- bulin (intravenous gammaglobulin) to control acute humoral rejection in renal and cardiac allograft recipients and potential mechanism of action. Transplantation 1998;66:800-5.
17) Magee JC, Collins BH, Harland RC, Lindman BJ, Bollinger RR, Frank MM, Platt JL. Immunoglobulin prevents comple- ment-mediated hyperacute rejection in swine-to-primate xeno- transplantation. J Clin Invest 1995;96:2404-12.
18) Schiff RI, Williams LW, Nelson RP, Buckley RH, Burks W, Good RA. Multicenter crossover comparison of the safety and efficacy of Intraglobin-F with Gamimune-N, Sandoglobulin, and Gammagard in patients with primary immunodeficiency diseases. J Clin Immunol 1997;17:21-8.
19) Bagdasarian A, Tonetta S, Harel W, Mamidi R, Uemura Y.
IVIG adverse reactions: potential role of cytokines and vasoa- ctive substances. Vox Sang 1998;74:74-82.
20) Sonnenday CJ, Warren DS, Cooper M, Samaniego M, Haas M, King KE, Shirey RS, Simpkins CE, Montgomery RA.
Plasmapheresis, CMV hyperimmune globulin, and anti-CD20 allow ABO-incompatible renal transplantation without splenec- tomy. Am J Transplant 2004;4:1315-22.
21) Rahman T, Harper L. Plasmapheresis in nephrology: an update.
Curr Opin Nephrol Hypertens 2006;15:603-9.
22) Kirk AD. Induction immunosuppression. Transplantation 2006;
82:593-602.
23) Salama AD, Pusey CD. Drug insight: rituximab in renal disease and transplantation. Nat Clin Practice 2006;2:221-30.
24) Sawada T, Fuchinoue S, Teraoka S. Successful A1-to-O ABO- incompatible kidney transplantation after a preconditioning regimen consisting of anti-CD20 monoclonal antibody infusions, splenectomy, and double-filtration plasmapheresis Transplan- tation 2002;74:1207-10.
25) Tydén G, Kumlien G, Genberg H, Sandberg J, Lundgren T, Fehrman I. ABO incompatible kidney transplantations without splenectomy, using antigen-specific immunoadsorption and rituximab. Am J Transplant 2005;5:145-8.
26) Malangoni MA, Dillon LD, Klamer TW, Condon RE. Factors influencing the risk of early and late serious infection in adults after splenectomy for trauma. Surgery 1984;96:775-83.
27) Alexander JW, First MR, Majeski JA, Munda R, Fidler JP, Morris MJ, Suttman MP. The late adverse effect of sple- nectomy on patient survival following cadaveric renal trans- plantation. Transplantation 1984;37:467-70.
28) Vieira CA, Agarwal A, Book BK, Sidner RA, Bearden CM, Gebel HM, Roggero AL, Fineberg NS, Taber T, Kraus MA, Pescovitz MD. Rituximab for reduction of anti-HLA antibodies in patients awaiting renal transplantation: 1. safety, pharmaco- dynamics, and pharmacokinetics. Transplantation 2004;77:
542-8.
29) Genberg H, Hansson A, Wernerson A, Wennberg L, Tydén G. Pharmacodynamics of rituximab in kidney transplantation.
Transplantation 2007;84:S33-S36.
30) Matignon M, Tagnaouti M, Audard V, Dahan K, Lang P, Grimbert P. Failure of anti-CD20 monoclonal antibody therapy to prevent antibody-mediated rejection in three crossmatch-
positive renal transplant recipients. Transplant Proc 2007;39:
2565-7.
31) Beimler JHM, Susal C, Zeier M. Desensitization strategies enabling successful renal transplantation in highly sensitized patients. Clin Transplant 2006;20:7-12.
32) Schröder C, Azimzadeh AM, Wu G, Price JO, Atkinson JB, Pierson RN. Anti-CD20 treatment depletes B-cells in blood and lymphatic tissue of cynomolgus monkeys. Transpl Immunol 2003;12:19-28.
33) Slifka MK, Ahmed R. Long-lived plasma cells: a mechanism for maintain persistent antibody production. Curr Opin Immunol 1998;10:252-8.
34) Book BK, Agarwal A, Milgrom AB, Bearden CM, Sidner RA, Higgins NG, Pescovitz MD. New crossmatch technique eliminates interference by humanized and chimeric monoclonal antibodies. Transplant Proc 2005;37:640-2.
35) Bearden CM, Agarwal A, Book BK, Sidner RA, Gebel HM, Bray RA, Pescovitz MD. Pronase treatment facilitates alloan- tibody flow cytometric and cytotoxic crossmatching in the presence of rituximab. Human Immunol 2994;65:803-9.
36) Bearden CM, Book BK, Sidner RA, Pescovitz MD. Removal of therapeutic anti-lymphocyte antibodies from human sera prior to anti-human leukocytes antibody testing. J Immunol Methods 2005;300:192-9.
37) Yang CW, Oh EJ, Lee SB, Moon IS, Kim DG, Choi BS, Park SC, Choi YJ, Park YJ, Han K. Detection of donor-specific anti-HLA class I and II antibodies using antibody monitoring system. Trans Proc 2006;38:2803-6.
38) Fuggle SV, Martin S. Toward performing transplantation in highly sensitized patients. Transplantation 2004;78:186-9.