110
<Received:June 6, 2014, Revised:June 23, 2014, Accepted:June 23, 2014>
Corresponding to:Seunghun Lee, Department of Radiology, Hanyang University College of Medicine, 17, Haengdang-dong, Seongdong-gu, Seoul 133-792, Korea. E-mail:[email protected]
pISSN: 2093-940X, eISSN: 2233-4718
Copyright ⓒ 2014 by The Korean College of Rheumatology
This is a Free Access article, which permits unrestricted non-commerical use, distribution, and reproduction in any medium, provided the original work is properly cited.
한양대학교 의과대학 영상의학교실
MRI Features of Axial Spondyloarthritis and Differential Diagnosis:
Focusing on the Spine and Sacroiliac Joint
Seunghun Lee
Department of Radiology, Hanyang University College of Medicine, Seoul, Korea
The spine and sacroiliac joint are involved in most cases of axial spondyloarthritis. Several pathologic findings from a ra- diography involving the spine and sacroiliac joint are the di- agnostic hallmarks of axial spondyloarthritis. However, these radiographic changes reflect structural damage rather than active inflammation, which may delay diagnosis by several years. Nowadays, the Assessment of SpondyloArthritis inter- national Society (ASAS) has focused on the reassessment of existing classification criteria and the development and vali-
dation of diagnostic tools to facilitate early diagnosis and as- sessment of treatment response. Magnetic resonance (MR) findings are the most remarkable changes with respect to the previously established classification criteria. Familiarity with typical MRI findings of axial spondyloarthritis and differ- ential diseases is important in order to correctly interpret the findings and avoid misdiagnosis.
Key Words. Spondyloarthritis, Spine, Sacroiliac joint, Magnetic Resonance Imaging
서 론
혈청음성 척추관절염(spondyloarthritis, SpA, 이하 척추관 절염)은 혈액에서 류마티스 인자는 발견되지 않으며 HLA-B27 항원의 발현율이 높은 만성 염증성 관절염의 한 종류이다 (1-6). 척추관절염은 특징적으로 천장관절염(sac- roiliitis)을 일으키며 부착부염(enthesopathy)을 일으키는 속 성과 함께 포도막염(uveitis) 등의 관절외 이상을 동반하는 질환군이다. 척추관절염은 임상적 특징에 따라 강직성 척 추염(ankylosing spondylitis, AS), 건선관절염(psoriatic ar- thritis, PsA), 반응관절염/라이터증후군(reactive arthritis/
Reiter’s arthritis, ReA/RD), 염증 장질환 관련 관절염(inflam-
matory bowel disease related arthritis, IBD-A), 미분화 척추관 절염(undifferentiated spondyloarthritis, uSpA) 등 5가지 질환 으로 나뉘어지며, 임상적 침범부위에 따라 천장관절과 척추 를 주로 침범하는 축성 척추관절염(axial spondyloarthritis)의 형태로 나타나거나 말초관절을 주로 침범하는 말초 척추관 절염(peripheral spondyloarthritis)의 형태로 나타난다.
단순촬영에서 천장관절염이 뚜렷하게 보여야 하는 이전의 기준과 달리 2009년 발표된 ASAS (Assessment of Spondylo- Arthritis international Society) 분류기준은 단순촬영에서는 뚜렷하게 보이지 않는 활동성 염증소견을 보여주는 천장관 절염의 자기공명 영상소견이 추가되었다(Figure 1) (7). 따라
Figure 1. ASAS classification cri- teria for axial spondyloarthritis (2009) in patients with back pain
≥3 months and age at onset >45 years. ASAS: Assessment of Spon- dyloarthritis International Society.
Figure 2. MRI changes in axial spondyloarthritis - ASAS/OMERACT consensual approach. ASAS: Asse- ssment of Spondyloarthritis Inter- national Society, OMERACT: Out- come Measures in Rheumatology.
Figure 3. Non-radiographic axial spondyloarthritis. (A) There is no evidence of sacroiliitis on plain radiography. (B) Hyperintense signal intensity on STIR image and (C) focal enhancement on fat-suppressed Gd-enhanced T1-weighted image in the left sacroiliac joint (arrows) reflect active inflammation. STIR: Short tau inversion recovery.
서, 이번 종설에서는 척추관절염의 조기 발견을 위해서 중 요성이 강조되고 있는 자기공명 영상소견을 천장관절과 척 추를 중심으로 급성 활동성 염증병변과 만성 염증병변으로 나누어 설명하도록 하고(Figure 2), 각 부위에서 알고 있어 야 할 감별질환에 대해 알아보고자 한다.
본 론
급성활동성 천장관절염과 만성 천장관절염의 영상소견 천장관절염을 평가하기 위한 자기공명영상기법은 우선 천골의 종축에 평행하게 얻은 경사관상영상(oblique coro- nal scan)을 기본평면으로 사용하며, 추가로 경사축상영상
Figure 5. (A) Oblique coronal T1-weighted, (B) fat-suppressed T2-weighted, and (C) fat-suppressed Gd-enhanced T1-weighted MR images of sacroiliac joints show focal capsulitis in the anterior aspect of left sacroiliac joint (arrows) and active inflammation in the sacrum near left sacroiliac joint.
Figure 4. (A) Oblique coronal T1-weighted, (B) STIR, and (C) fat-suppressed Gd-enhanced T1-weighted MR images of sacroiliac joints show focal bony erosion, subchondral sclerosis and synovitis (arrows).
Figure 6. (A) Axial STIR and (B) fat-suppressed Gd-enhanced T1-weighted MR images of sacroiliac joints show enthesitis in the left posterosuperior sacroiliac joint (arrows). STIR: Short tau inversion recovery.
Figure 8. (A) Oblique coronal T1-weighted, (B) fat-suppressed T2-weighted, and (C) fat-suppressed Gd-enhanced T1-weighted MR images of sacroiliac joints show subchondral bone erosions (arrow) and fat deposition (star) around both sacroiliac joints.
Figure 7. Staging of axial spondyloarthritis.
(oblique axial scan)이나 축상영상(axial scan)을 얻기도 한 다. 얻어야 할 경사관상 자기공명영상은 병원에 따라 차이 가 있으나주로 단시간반전회복(STIR) 영상 혹은 지방억제 T2강조영상을 통해 병변의 활동성 여부를 판정하고 T1강 조영상을 통해 관절주위 골수의 지방침착, 지방억제 T1강 조영상 또는 T2강조영상을 통해 골미란 여부를 판정한다 (8-11). 경우에 따라 지방억제 조영증강 T1강조영상을 부 착부염이나 활액막염의 유무를 알기 위해 시행할 때도 있 다 (12).
다른 영상기법과 비교하여 자기공명영상은 천장관절의 연골하 골수부종, 골염, 부착부염, 관절낭염과 같은 급성 활동성 염증병변을 특징적으로 보여주기 때문에 단순촬영 이나 CT등에서 보이는 골미란이나 골경화 같은 형태학적 변화가 나타나기 전에 천장관절염을 조기에 진단할 수 있 으며, 골미란, 관절주위 지방침착, 연골하골경화, 관절강직 과 같은 만성 형태학적인 변화 소견도 진단할 수 있다 (8-11).
골수부종이나 골염은 관절주위 연골하 부위가 T1강조영 상에서 저신호강도, 지방억제 T2강조영상이나 단시간반 전회복영상에서 고신호강도로 나타나며, 지방억제 조영증 강 T1강조영상에서는 조영증강을 보이는데, 이는 천장관
절염의 활동성 여부를 판정하는 가장 중요한 기준이다 (Figure 3) (12). 골수부종은 대개 양측성, 대칭적으로 나타 나며 관절의 아래쪽과 뒤쪽 1/3 부위에 잘 나타난다 (12).
활액막염은 정상적인 연골신호강도의 소실과 함께 T1강 조영상에서 저신호 또는 중등도 신호강도로 보이고, 지방 억제 T2강조영상이나 단시간반전회복영상에서는 다양한 정도의 고신호강도로 나타나며 조영증강에서 선상 또는 점상의 조영증강(화살표)을 보인다(Figure 4). 활액막염과 관절액의 구별이 단시간반전회복영상에서는 어려울 수 있 으며 이 때는 지방억제 조영증강 T1강조영상을 이용함으 로써 활액막염을 구별할 수 있다 (12). 관절낭염은 활액막 염과 비슷한 신호강도를 보이고, 지방억제 조영증강 T1강 조영상에서 조영증강을 보인다(Figure 5). 천장관절의 후상 부 1/3에서 보이는 부착부염도 지방억제 T2강조영상과 단 시간반전회복영상에서 고신호강도를 보이고, 조영증강 T1강조영상에서 조영증강된다(Figure 6). 특히, 단순촬영 이나 CT등의 방사선 영상에서는 진단되지 않고 자기공명 영상소견에서 연골하 골수부종이 있거나 조영증강을 보이 는 골염이 있을 때 비방사선학적 축성 척추관절염으로 정 의한다(Figure 3 and 7).
연골하 경화소견은 모든 자기공명영상에서 저신호강도 로 나타나고 주변 피질골보다 두껍게 보이면서 피질-골수 인접면이 명확하지 않게 보인다(Figure 4).
골미란은 장골에서 먼저 나타나고 피질골은 유지되어 있 지 않으면서 관절면의 연골하골이 불규칙적인 결손 모양 을 보이고 T1강조영상에서 저신호강도, 지방억제 T2강조 영상이나 단시간반전회복영상에서 고신호강도로 나타난 다(Figure 4). 관절주위의 지방침착은 골미란과 인접하여 나타나고 만성적 골미란과 관계가 있다(Figure 8).
천장관절염의 감별질환
1) 퇴행성 천장관절염(degenerative sacroiliitis): 천장관절의 퇴 행성 변화는 주로 관절간격이 좁아지고 불규칙해지며 관
Figure 9. 50-year-old women with degenerative sacroiliitis. (A) Axial and (B) oblique coronal CT scans show osteophytes (arrows) and subchondral sclerosis in the anterior aspect of both sacroiliac joints without definite bony erosion in the both sacroiliac joint.
Figure 10. (A) Plain radiography and (B) oblique coronal CT scans of sacroiliac joint show well-defined trangular sclerosis involving both sacroiliac joints without definite bony erosions. (C) Oblique coronal T1-weighted and (D) fat-suppressed T2-weighted MR images of sacroiliac joints show well-defined low signal intensity in the both ilium near both sacroiliac joints without definite bony erosions characterizing sclerosis.
Figure 11. 63-year-old women with right pyogenic sacroiliitis. (A, B) Fat-suppressed Gd-enhanced T1-weighted MR images show focal loculated fluid collection and soft tissue inflammation (arrows) in the anterior aspect of right sacroiliac joint with marrow enhancement in the right ilium characterizing osteomyelitis.
Figure 12. Pelvic abnormalities in DISH. (A) Note the irregular bony excrescences above the both anterior inferior iliac spines (arrow heads) and heterotopic ossification along the right sacrotuberous ligament (empyt arrow) in relation to DISH. (B) The osseous bridges (arrows) extend across the both sacroiliac joints without definite sacroiliitis. DISH: diffuse idiopathic skeletal hyperostosis.
절주위 연골하 부위에 경화 소견이 보이고 연골하 낭종도 보일 수 있으나, 염증성 관절염의 특징적인 소견인 골미란 은 보이지 않는다 (13). 퇴행성 변화는 주로 노인층에서 잘 발생하고 관절 하부 2/3에 국한된다(Figure 9) (14).
2) 장골치밀화골염(osteitis condensans ilii): 장골치밀화골염은 천장관절주위, 특히 편측 또는 양측 장골에 경계가 좋은 삼각형의 골경화 소견을 보이는 경우를 말한다 (14,15). 대 부분은 출산 경험이 있는 여성에서 흔하며 원인으로는 임 신과 출산동안 골반 인대가 느슨해지고, 천장관절에 압력 이 증가하게 되어 나타나는 소견으로 생각되고 있다 (16).
자기공명영상에서는 T1강조영상과 지방억제 T2강조영상 모두에서 저신호강도를 보이면서 경계가 좋은 병변이 주 로 장골에 보이게 된다(Figure 10).
3) 감염성천장관절염(infectious sacroiliitis): 감염성 천장관절 염은 주로 편측성으로 지방억제 조영증강 T1강조영상과 단시간반전회복영상에서 활액막염, 관절연골과 연골하골
의 파괴와 주위의 골수염, 주위 연조직의 부종, 농양등의 변화가 심하게 나타난다(Figure 11). 천장관절 주위에서 연 조직의 농양이 보인다면 감염성 천장관절염을 진단하는 데 도움이 된다 (14,15).
4) 미만성 특발성 골격 과골화증(diffuse idiopathic skeletal hy- perostosis): 미만성 특발성 골격 과골화증(diffuse idiopathic skeletal hyperostosis, DISH)은 척추와 척추외 골격을 침범 하는 미만성 골형성 변화로 주로 인대나 건에 골형성이 나 타난다. 원인에 대해서는 알려진 바 없으나, 고령에서 주 로 호발하므로 퇴행 변화의 특별한 형태로 생각되고 있다.
흉추에 호발하며 그 외 경추나 요추도 침범할 수 있는 데, 천장관절을 침범하는 경우 관절주위에 골증식체(osteo- phyte)이 생겨서 골융합(osseous fusion)이 생길 수도 있지 만 관절내골미란이나 융합은 없다(Figure 12) (3,14).
5) 천골 부전골절(insufficiency fracture of the sacrum): 천골 부 전골절은 방사선 치료후에 혹은 골다골증과 관련해 생긴
Figure 14. (A, B) Sagittal and (C) axial CT scans of thoracic spine. Spondyloarthritis involving the spine show-vertebral body (triangles), discovertebral junction (semicircles), the interspinous spaces (arrows), facet joints (empty arrows), costovertebral joint (arrow heads), costotransverse joint (asterisks).
Figure 13. (A) There is no evidence of sacroiliitis on plain radiography of pelvis. Subtle sclerosis in the left sacral wing is suspected.
(B) Hypointense signal intensity on T1-weighted image and (C) diffuse edema on STIR in the left sacral wing (arrows) reflect insufficient fracture. STIR: Short tau inversion recovery.
Figure 15. (A) Sagittal fat-supp- ressed T2-weighted and (B) fat-su- ppressed Gd-enhanced T1-weighted MR images of lumbar spine show active inflammation in the corners of L4 vertebral bodies (arrows) in spondyloarthritis. (C) Sagittal T1- weighted and (D) fat- suppressed Gd-enhanced T1-weighted MR images of lumbar spine show fat deposition in the corners of L4 vertebral bodies (arrow heads) cha- racterizing inactive lesions.
Figure 16. (A) Sagittal fat-suppressed T2-weighted and (B) fat-suppressed Gd-enhanced T1-weighted MR images of thoracic spine show end-plate erosion with subchondral marrow edema and inflammation characterizing spondylodiskitis (arrows).
Figure 17. (A) Sagittal and (B) axial fat-suppressed Gd-enhanced T1-weighted MR images of thora- cic spine show enhancement in the facet joint (arrows), costovertebral joint (arrow head) and costotran- sverse joints (asterisks) characteri- zing active inflammation.
다고 알려져 있으며 진단이 어려운 경우가 종종 있다. 주 요한 방사선학적 소견은 골소주(trabecula)의 압박과 가골 형성에 의해 나타나는 골경화이다 (17). 또한 특징적인 소 견이 골절이 발생하는 위치인데, 주로 천골 날개(sacral ala) 에 수직으로 진행하는 양상이며 천장관절에 평행하게 발 생한다. 자기공명영상에서는 특징적인 골부종 소견이 골 절주변으로 뚜렷하게 보여 T1강조영상에서 저신호강도, 지방억제 T2강조영상과 단시간반전회복영상에서 고신호 강도를 보이게 된다(Figure 13).
급성 활동성 척추관절염과 만성 척추관절염의 영상소견 척추관절염을 평가하기 위한 자기공명영상기법은 시상 면(sagittal) T1강조영상과 지방억제 T2강조영상이고, 지방 억제 조영증강 T1강조영상은 급성염증을 발견 하는데 더 민감하고 감염성 질환과 감별하는 데 사용된다. 축상면 (axial) 영상은 후관절(facet joint), 늑골척추관절(costoverte- bral joint), 늑골횡돌기관절(costotransverse joint)등의 병변 을 보는데 유용하다.
척추에서 급성 활동성 염증은 척추체, 추간판척추체경계 (discovertebral junction), 후관절, 늑골척추관절, 늑골횡돌 기관절, 고리중쇠관절(atlantoaxial joint) 및 척추후부인대 부착부위등에서 관찰되는데, 초기에는 흉요추경계 및 요 천추경계부위에서 변화가 뚜렷하고 진행하면서 전체 척추 의 변화로 나타난다(Figure 14).
척추체의 염증은 섬유테(annulus fibrosus)의 외섬유(outer fiber)가 부착하는 척추체 테두리의 골염(osteitis)와 전종인 대(anterior longitudinal ligament), 후종인대(posterior longi- tudinal ligament)의 부착부염(enthesitis)으로 주로 상부와 하 부의 모퉁이와 전면(anterior border)에서 저명하다. 하부요 추보다는 흉요추 경계부위에 흔하게 나타나는 것으로 알 려져 있고, 급성기에는 골수부종으로 인해 T1강조영상에 서 저신호강도, 지방억제 T2강조영상이나 단시간반전회
복영상에서 고신호강도를 보인다. 골염이 오래 진행되고 치유과정에 이르면 골수부종이 소실되고 지방골수로 변환 되므로 T1강조영상에서 고신호강도를 보이고 지방억제 T2강조영상이나 단시간반전회복영상에서는 저신호강도 를 보이게 된다(Figure 15).
추간판척추체경계부염(spondylodiskitis)은 초기에는 척추 종판(endplate)의 골미란과 주변부 골수부종이 추간판을 중심으로 상하부에 반구형(hemispheric appearance)으로 관 찰되며 염증성 앤더슨병변(inflammatory Andersson lesion) 으로도 불린다(Figure 16). 후관절, 늑골척추관절, 늑골횡돌 기 관절등의 급성 활동성 염증은 관절내 삼출액, 주변부 골부종, 활액막염등의 소견으로 보일 수 있고(Figure 17),
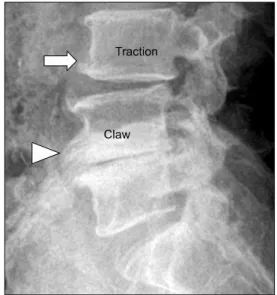
Figure 19. Segmental instability of lumbar spine. A traction osteophyte (arrow) in L3 body develops 2 to 3mm from the edge of the intervertebral disc and horizontal direction. A claw osteophyte (arrow head) in L4 body develops closer to the disc margin and has a sweeping configuration.
Figure 18. (A) Enthesitis in the L1-2 interspinous and supraspi- nous ligaments (arrow) on sagittal fat-suppressed Gd-enhanced T1- weighted MR image. (B) AP radiographs of the lumbar spine reveals ossification of the inters- pinous and supraspinous ligaments, which is producing a vertical central radiodense shadow, the dagger sign.
중요한 병변으로 척추관절염의 특징적 소견인 인대골증식 체(syndesmophytes)와 혼동되기 쉽다. 퇴행성 골증식체는 섬유테(annulus fibrosus) 부착부위의 뼈과다증(hyperosto- sis)으로 삼각형 모양의 성장(triangular outgrowth)을 보이 고 추간판 간격이 좁아져 있으며, 척추종말판을 따라서 골 경화 소견이 잘 동반된다(Figure 19) (13).
2) 미만성 특발성 골격 과골화증(diffuse idiopathic skeletal hy- perostosis, DISH): 미만성 특발성 골격 과골화증(DISH)은 주 로 흉추에 호발하며 그 외 경추나 요추도 침범할 수 있는 데, 과골화로 인한 척추체의 연결이 연속적으로 적어도 네 군데에 걸쳐서 보일 때 미만성 특발성 골격 과골화증으로 진단할 수 있다 (3). 미만성 특발성 골격 과골화증은 주로 흉추 7번에서 흉추 11번 사이에 호발하며, 주로는 척추체 의 전방이나 전외측에 특징적으로 불규칙하고 두꺼운 척 추주위 골화를 형성하며 이는 척추체와 분리되어 형성된 다. 또한 추간판 간격은 유지되어 있고 척추의 후관절과 천장관절의 침범은 보이지 않는다(Figure 20) (3,4,14). 반
Figure 20. (A) Plain radiography of lateral cervical spine, (B) sagittal CT scan and (C) sagittal T1-weighted MR image of cervial spine show extensive anterior bone formation (arrows) and anterior disc extension(empty arrows) without facet involvement (arrow head).
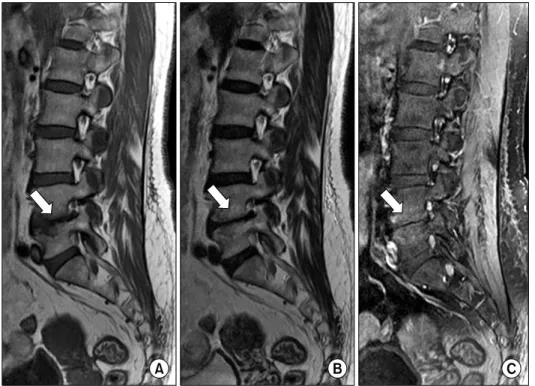
Figure 21. Abnormal intervertebral disc: Modic type I change. (A) Sagi- ttal T1-weighted, (B) T2-weighted and (C) fat-suppressed Gd-enhanced T1-weighted MR images show marrow edema and inflammation without erosion around L4-5 inter- vertebral disc (arrows) characteri- zing fibrovascular marrow.
이에 의해서 척수압박증상이 나타날 수 있다. 강직성 척추 염에서 보이는 인대골증식체(syndesmophytes)는 초기에 섬 유테의 바깥층을 따라서 골화가 생기기 시작하므로 척추체 의 외연에 붙어 진행하고 비교적 얇은 두께를 보인다.
3) 퇴행성 종판변화(intervertebral osteochondrosis, Modic dis-
ease): 퇴행성 종판변화는 수핵의 퇴행성 변화와 연관된 종
판(endplate)과 연골하 골수 변화를 보이는 질환이다. 추간 판의 높이 감소와 vacuum phenomenon등의 변화를 보이며 자기공명영상 소견상 세가지 유형(type)으로 나뉘어 진다 (18). 제1유형은 조직 소견상 섬유혈관 골수(fibrovascular marrow) 소견으로 T1강조영상에서 저신호강도, T2강조영 상에서 고신호강도를 보이고(Figure 21), 제2유형은 조직
fat-suppressed Gd-enhanced T1-weighted MR images reveal prominent marrow signal change with end plate erosions (arrows) and paraspinal soft tissue phlegmon (arrow heads) around L5-S1 disc.
소견상 지방 골수(fatty marrow)의 소견으로 T1강조영상에 서 고신호강도, T2강조영상에서 고신호강도를 보이며, 마 지막으로 제3유형은 조직 소견상 골경화 소견으로 T1강조 영상에서 저신호강도, T2강조영상에서 저신호강도를 보 인다. 퇴행성 종판변화는 보통 인접한 추간판의 퇴행성 변 화를 동반하는 반면에 척추 관절염에서의 추간판척추체경 계부염(Andersson lesion)에서는 드물다 (19).
4) 감염성 척추추간판염(infectious spondylodiskitis): 감염성 척 추추간판염과 추간판척추체경계부염(Andersson lesion)의 감별은 다소 복잡하며, 감염성 척추추간판염은 특징적으 로 척추체 주변의 연부조직과 경막외 공간의 염증성 변화 가 잘 동반되고, 척추종판의 변화가 뚜렷하다(Figure 22).
결 론
축성 척추관절염은 천장관절과 척추를 침범하는 염증성 병변으로 특징적인 영상의학적 소견을 보이며 감별해야 하는 다양한 질환의 영상 소견을 정확히 숙지해야 임상 진 료시 도움을 받을 수 있다. 그 중에서 자기공명영상은 축 성 척추관절염의 조기 진단, 추적검사뿐 아니라 치료결과 의 판정에 있어서 질병의 유무와 활성도를 측정할 수 있는 좋은 검사이다. 또한 자기공명영상은 점차 천장관절염의 표준 참고 검사로 각광받고 있으며 비방사선학적 축성 척 추관절염의 진단에는 필수적인 영상 수단이 되었다. 최근 에는 자기공명영상이 염증성 활동을 정량화하는 수단으로 쓰이고 있을 뿐 아니라 임상치료의 효과 추적 검사 수단으 로도 사용되고 있다. 여기에 최근 새로운 영상기법들의 발 달로 전신 자기공명영상까지 촬영이 가능해 지고 있어 앞 으로는 검사도중에 환자의 위치변화나 코일의 교체없이 현재보다 빠른 시간내에 척추관절염을 폭넓게 평가할 수 있을 것으로 기대한다.
References
1. van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis. A pro- posal for modification of the New York criteria. Arthritis
Rheum 1984;27:361-8.
2. Dougados M, van der Linden S, Juhlin R, Huitfeldt B, Amor B, Calin A, et al. The European Spondylarthropa- thy Study Group preliminary criteria for the classification of spondylarthropathy. Arthritis Rheum 1991;34:1218-27.
3. Resnick D, Kransdorf MJ. Bone and joint imaging. 3rd ed. p. 267, Philadelphia, Elsevier Saunders, 2005.
4. Yochum TR, Rowe LJ. Essentials of skeletal radiology.
2nd ed. p. 877, Baltimore, Williams and Wilkins, 1996.
5. Braun J, Bollow M, Sieper J. Radiologic diagnosis and pathology of the spondyloarthropathies. Rheum Dis Clin North Am 1998;24:697-735.
6. Jacobson JA, Girish G, Jiang Y, Resnick D. Radiographic evaluation of arthritis: inflammatory conditions.
Radiology 2008;248:378-89.
7. Rudwaleit M, van der Heijde D, Landewé R, Listing J, Akkoc N, Brandt J, et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): validation and final selection. Ann Rheum Dis 2009;68:777-83.
8. Jee WH, McCauley TR, Lee SH, Kim SH, Im SA, Ha KY. Sacroiliitis in patients with ankylosing spondylitis:
association of MR findings with disease activity. Magn Reson Imaging 2004;22:245-50.
9. Rudwaleit M, Jurik AG, Hermann KG, Landewé R, van der Heijde D, Baraliakos X, et al. Defining active sacroi- liitis on magnetic resonance imaging (MRI) for classi- fication of axial spondyloarthritis: a consensual approach by the ASAS/OMERACT MRI group. Ann Rheum Dis 2009;68:1520-7.
10. Bredella MA, Steinbach LS, Morgan S, Ward M, Davis JC. MRI of the sacroiliac joints in patients with moderate to severe ankylosing spondylitis. AJR Am J Roentgenol 2006;187:1420-6.
11. Lacout A, Rousselin B, Pelage JP. CT and MRI of spine and sacroiliac involvement in spondyloarthropathy. AJR Am J Roentgenol 2008;191:1016-23.
12. Sieper J, Rudwaleit M, Baraliakos X, Brandt J, Braun J, Burgos-Vargas R, et al. The Assessment of SpondyloAr- thritis international Society (ASAS) handbook: a guide to assess spondyloarthritis. Ann Rheum Dis 2009;68 Suppl 2:ii1-44.
13. Jacobson JA, Girish G, Jiang Y, Sabb BJ. Radiographic evaluation of arthritis: degenerative joint disease and variations. Radiology 2008;248:737-47.
14. Kang HS, Hong SH, Chang HK. Musculoskeletal Radiology. 1st ed. p. 121, Seoul, Korea, Medicalplus, 2013.
15. Canella C, Schau B, Ribeiro E, Sbaffi B, Marchiori E.
MRI in seronegative spondyloarthritis: imaging features and differential diagnosis in the spine and sacroiliac joints. AJR Am J Roentgenol 2013;200:149-57.
16. Olivieri I, Ferri S, Barozzi L. Osteitis condensans ilii. Br J Rheumatol 1996;35:295-7.
17. Resnick D, Niwayama G. Osteoporosis. In: Resnick D, Niwayama G, eds. Diagnosis of bone and joint disorders.
3rd ed. p. 1839, Philadelphia, WB Saunders, 1995.
18. Modic MT, Steinberg PM, Ross JS, Masaryk TJ, Carter JR. Degenerative disk disease: assessment of changes in vertebral body marrow with MR imaging. Radiology 1988;166:193-9.
19. Resnick D, Niwayama G. Ankylosing spondylitis. In:
Resnick D, ed. Diagnosis of bone and joint disorders. 3rd ed. p. 1008. Philadelphia, WB Saunders, 1995.