대한소화기학회지 2005;46:485-488
서 론
췌장루(pancreatic fistula)는 주로 외상이나 수술에 따른 췌 장 손상 때문에 생기며, 드물게는 급성 또는 만성췌장염의 합병증으로도 발생할 수 있다.1 췌장루는 크게 피부와 연결 되는 외부 췌장루와 내부 장기와 교통되는 내부 췌장루로 나눌 수 있는데, 외부 췌장루가 내부 췌장루보다 발생 빈도 가 훨씬 더 높다.1 내부 췌장루는 주로 인접 장기로 교통되 며 복막, 위, 소장, 대장, 담낭 등 복강 내 장기 외에도 흉막 강, 기관지, 중격동 등으로 교통된다.2 췌장염의 합병증으로 발생한 췌장루 중 췌관과 문맥 사이의 누공은 매우 드물 며,3,4 합병증이 동반될 경우 사망률이 높아 적극적인 수술
치료를 요한다.5 췌관-문맥 누공은 국내에는 아직 보고가 없 다. 저자들은 중증 급성췌장염의 합병증으로 발생한 췌관- 문맥 누공 1예를 경험하여서 문헌고찰과 함께 보고한다.
증 례
32세 남자가 일주일간 지속된 심와부 동통으로 내원하였 다. 환자는 내원 일주일 전 술을 많이 마신 후 누우면 심해 지고, 앉으면 호전되는 심와부 동통이 계속돼 외부 병원을 방문하였다. 당시 혈중 아밀라아제/리파아제 312/1,270 U/L 이었으며, 복부 전산화단층촬영에서 급성췌장염과 췌장 주 변의 액체 저류가 나타나 본원으로 옮겨졌다.
중증 급성췌장염에 합병된 췌관-문맥 누공 1예
울산대학교 의과대학 서울아산병원 내과학교실, 방사선과학교실*
여영선․김명환․유미현․정영주․김순주․변재호*
A Case of Pancreaticoportal Fistula Associated with Acute Severe Pancreatitis
Young Sun Yeo, M.D., Myung Hwan Kim, M.D., Mi Hyun Yu, M.D., Young Ju Jung, M.D., Soon Joo Kim, M.D., and Jae Ho Byun, M.D.
*
Departments of Internal Medicine and Diagnostic Radiology*, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
Pancreatic fistulas are usually caused by the disruption of pancreatic duct. The majority of pancreatic fistulas are external fistulas and common causes of external and internal pancreatic fistulas are trauma and surgery. Internal pancreatic fistulas due to pancreatitis are rare. Internal pancreatic fistulas may communicate with peritoneal cavity, colon, small bowel, biliary system or pleural cavity. Among them, fistula between pancreatic duct and portal vein due to acute pancreatitis is rare. We report a case of 32-year-old male with fistula between pancreatic duct and portal vein as a complication of acute pancreatitis. Pancreaticoportal fistula was diagnosed by endoscopic retrograde cholangiopancreatography. He recovered after distal pancreatectomy with splenectomy and supportive care. (Korean J Gastroenterol 2005;46:485-488)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Key Words: Pancreatic fistula; Acute pancreatitis
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
접수: 2005년 6월 22일, 승인: 2005년 9월 20일 연락처: 김명환, 138-736, 서울시 송파구 풍납동 388-1
서울아산병원 소화기내과
Tel: (02) 3010-3180, Fax: (02) 476-0824 E-mail: mhkim@amc.seoul.kr
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Correspondence to: Myung-Hwan Kim, M.D.
Department of Internal Medicine, Asan Medical Center 388-1 Pungnap-dong, Songpa-gu, Seoul 138-736, Korea Tel: +82-2-3010-3180, Fax: +82-2-476-0824
E-mail: mhkim@amc.seoul.kr
486 대한소화기학회지: 제46권 제6호, 2005
과거력에서 특이사항은 없었고, 10년간 주 2-3회 소주 2-3 병의 음주력이 있었으며, 가족력에서는 특이사항이 없었다.
신체검사에서 혈압 130/80 mmHg, 맥박 96회/분, 호흡수 20 회/분, 체온 36.4oC였으며, 급성 병색을 보였다. 결막 빈혈이 나 공막 황달은 관찰되지 않았으며, 흉부 청진에서 양측 폐 하부로 호흡음이 감소되었으며, 심음은 규칙적이고 잡음은 없었다. 복부는 부어 있었고, 장음은 감소되었으며, 복부에 전반적인 압통이 있었다.
말초혈액검사에서 백혈구 14,800/mm3, 혈색소 12.5 g/dL, 헤마토크리트 35.7%, 혈소판 382,000/mm3이었고, CRP 29.4
mg/dL였다. 생화학검사에서 칼슘 7.4 mg/dL, 인 1.4 mg/dL, 혈당 176 mg/dL, BUN/크레아티닌 12/0.8 mg/dL, 총 단백 6.0 g/dL, 알부민 2.5 g/dL, AST/ALT 58/43 IU/L, 알칼리 포스파 타제 85 IU/L, 총 빌리루빈 1.5 mg/dL, 아밀라아제/리파아제 107/ 58 U/L, LDH 1,338 U/L, 중성지방 112 mg/dL이었으며 PT 75.2% (1.27 INR), aPTT 49.1초였다.
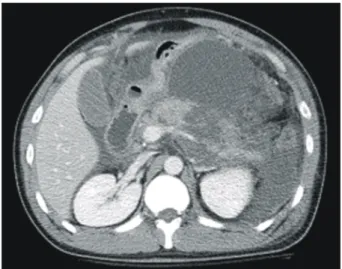
단순 흉부 촬영에서 양측 늑골 횡격막각의 둔화 소견이 보였으며, 단순 복부 촬영에서 전반적인 음영 증가가 보였 다. 입원 당시 시행한 복부 전산화단층촬영에서 췌장이 전 반적으로 부어 있었으며 췌장 주변과 늑막 주변, 양측 신장 주변에 다량의 액체 저류가 관찰되어 중증 췌장염으로 분류 하였다. 일부 췌실질은 조영 증강이 관찰되지 않아 췌실질 괴사의 동반이 강력히 의심되었다(Fig. 1).
내원 1일째 환자는 복통과 함께 호흡곤란을 호소하였으 며, 동맥혈 가스분석에서 산소분압 58.8 mmHg 소견을 보여 췌장 주변의 다량의 액체 저류에 대해 배액 목적의 배액관 을 삽입하였다. 액체 내 아밀라아제/리파아제는 4,011/13,564 U/L로 측정되었고 배양검사에서 균은 자라지 않았다.
금식, 항생제, octreotide를 사용하면서 보존 치료를 시행 하였다. 내원 14일째 시행한 복부 전산화단층촬영에서 췌장 주변의 액체 저류량은 배액관 삽입에 의해 다소 감소했으나 여전히 광범위한 액체 저류가 나타났다. 내원 30일째 주췌 관으로부터 췌액 유출 유무와 그 정도를 파악하고, 필요하 다면 주췌관 내로의 배액관 삽입을 고려하기 위해서 내시경 역행췌담관조영술을 시행하였다(Fig. 2). 당시 총담관에서 다량의 담즙 찌꺼기가 배출되었고 총담관은 경도로 확장되 어 있었으며, 주췌관 내로 카테터를 삽관한 후에 조영제를 Fig. 1. Abdominal CT. It shows extensive fluid collection around
the pancreas. Body portion of pancreatic parenchyma does not show enhancement, suggesting pancreatic necrosis.
Fig. 2. ERCP. (A) When the contrast is injected via a catheter inserted into the main pancreatic duct, pancreatic head portion (black arrowheads) is visualized, only. With further injection of contrast, faint visualization of portal vein (white arrowheads) is noted. (B) When the contrast is injected via endoscopic nasopancreatic drainage tube, portal vein (white arrowheads) running parallel to extrahepatic bile duct is visualized along with the branches of downstream pancreatic duct (black arrowhead). Drainage tube for peripancreatic fluid collection is also noted.
A B
여영선 외 5인. 중증 급성췌장염에 합병된 췌관-문맥 누공 1예 487
주입했을 때 췌두부 주췌관만 조영되었고, 췌장 체부에서 조영제가 누출되면서 간 문맥이 같이 조영되어 췌관-문맥 누공으로 판단하였다. 급성췌장염과 이에 합병된 주췌관 손 상에 의한 췌액 누출에 대해 수술 치료를 하기로 결정하고, 내원 32일째 원위부 췌-비장절제술을 시행하였고 췌관-문맥 누공부위는 수술하지 않고 보존 치료하기로 하였다. 수술 후 임상양상이 호전되어 퇴원하였다. 추적 검사로 시행한 복부 전산화단층촬영에서 췌장 부종은 감소되었고 경계는 뚜렷해졌고, 췌장 주변의 액체 저류는 더 이상 관찰되지 않 았으며, 문맥 내 음영 등의 이상소견은 관찰되지 않았다 (Fig. 3).
고 찰
췌장루는 췌장손상이나 염증에 의한 췌관 손상으로 발생 한다. 원인으로 복부 둔상이나 췌장 수술에 의한 췌장 손상 이 60%로 가장 흔하며, 췌장염에 의한 경우 가성낭종이 합 병된 경우는 27%이고, 가성낭종이 동반되지 않은 경우는 5% 정도이다.1,2 췌장 가성낭종이 존재할 때 췌장루가 발생 하는 기전은 정확히 알려져 있지 않으나, 압박괴사로 인한 가성낭종의 파열, 가성낭종 내 췌장 효소의 활성화로 인한 주변 조직의 미란 등을 가능한 기전으로 추정한다.5 췌장루 에서 누공이 형성되는 인접 장기로는 복막강, 위장관, 담도 계, 비장 등 복강 내 장기나 흉막강, 종격동, 기관지 등이 있 다. 이번 증례와 같은 문맥으로의 누공 형성은 매우 드물 며,3-18 국내에서는 보고된 바 없다.
보고된 예 중에 급성췌장염에 의한 가성낭종에서 누공이 발생한 경우가 2예13,14 있었고, 나머지는 만성췌장염에서 발 생한 경우였다. 이 중 가성낭종을 동반하지 않은 예는 2예
였다.7,15 이번 증례는 췌장염의 발생 시기와 복부 전산화단 층촬영 소견을 종합하여 고려할 때 아직 가성낭종 형성에는 이르지 못한 급성 액체 저류상태로 본다. 문맥으로의 누공 형성 기전은 가성낭종이나 유출된 췌액 내 췌장 효소의 활 성화로 인해 혈관 벽의 미란이 발생하기 때문이며,5 이로 인 해 문맥 내 혈전이 형성되고, 그 직후 췌장과의 누공이 발생 한다.11
췌관-문맥 누공 발생의 증상으로는 무증상 또는 경미한 복통을 호소한 경우가 많았고, 위장관 출혈 2예,11,12 패혈증 1예,14 폐혈전색전증 1예,18 피하 결절이나 봉와직염, 골수염, 광범위 피하지방 괴사가 5예13,15-17에서 있었다. 이 중 봉와직 염, 골수염, 광범위 피하지방 괴사는 췌장 효소가 문맥 내 혈전을 녹이면서 순환계로 유입되어 전신의 지방, 단백 분 해가 일어나는 것으로,11,13 이 경우 사망률이 50% 정도로 높 아서 진단이 되면 수술 치료를 적극 고려해야 한다.5 이번 증례에서는 심한 복통 호소는 있었으나, 출혈이나 패혈증, 광범위 피하지방 괴사와 같은 췌관-문맥 누공에 의한 합병 증은 발생하지 않았다.
췌관-문맥 누공의 진단 방법 중 복부 전산화단층촬영은 누공의 위치는 확인할 수 없지만, 동반된 췌관 확장이나 석 회화, 췌장 가성낭종의 유무를 알 수 있고, 일부에서 문맥 내에 혈전보다 낮은 농도의 액체 소견이나 혈관 벽의 비후 소견 등을 관찰할 수 있다.11 내시경역행췌담관조영술은 췌 장루의 확진과 분지 정도, 해부학 구조, 기시부와 췌관의 상 태를 알 수 있어 치료 계획 설정에 도움을 줄 수 있다. 문헌 에서 6예는 이번 증례와 같이 내시경역행췌담관조영술로 췌관-문맥 누공을 진단하였고,3,7,8,10,12,13
3예는 경피경간 문맥 조영술로 누공의 존재를 확인하고, 문맥 흡인검사에서 아밀 라아제, 리파아제가 상승되어 있는 흑갈색의 액체를 확인하 여 확진하였다.3,4,11 사망 후 부검으로 진단된 경우도 5예 있 었다.9,12,16-18
치료는 증상이 없거나 임상 양상이 가볍고, 자연 폐쇄가 예측되면 보존 치료를 시도해 볼 수 있다. 보존 치료에 실패 하거나, 내시경역행췌담관조영술에서 주췌관 손상과 연관 된 췌액 유출이 관찰될 경우 경유두로 췌관 내 배액관을 삽 입하여 췌액 유출을 차단시킴으로써 문맥 누공이 저절로 막 히는 것을 기대할 수 있다.19 보존 치료로는 금식과 수분, 전 해질과 영양 공급이 중요하며, 최근 somatostatin analogue인 octreotide의 치료 효과가 보고되었다.20 이번 증례에서는 주 췌관 손상으로 인한 췌액 누출에 의한 췌장 주변 괴사와 유 착이 심해서 수술 치료를 시행하였다.
예후는 보고된 16예 중 보존 치료로 호전된 경우가 3
예,7,8,10 수술 치료 후 호전된 경우는 6예,3,4,11,14,15
합병증에 의해 사망한 경우가 6예였다. 사망 원인으로는 광범위 피하 지방 괴사,16,17 신부전,3 위장관 출혈,12 패혈증,9 폐혈전색전 Fig. 3. Follow-up Abdominal CT. After distal pancreatectomy with
splenectomy, peripancreatic infiltration and fluid collection dis- appeares with improvement in pancreatic swelling.
488 The Korean Journal of Gastroenterology: Vol. 46, No. 6, 2005
증18으로 나타났다.
결론으로, 이번 증례는 중증 급성췌장염 환자에서 주췌관 손상에 의한 췌액 누출로 혈관 미란이 생겨 췌관-문맥 누공 이 발생했으며, 장기간 보존 치료에도 호전되지 않아 내시 경역행췌담관조영술로 진단하였다. 췌장 주변 조직 괴사와 유착에 대해 원위부 췌-비장절제술을 시행하였고, 누공부위 는 수술에 포함되지 않았으며, 이후 보존 치료로 환자는 호 전되었다. 췌장염에 의한 췌관-문맥 누공 형성은 매우 드문 합병증으로 국내에는 아직 보고가 없어서 증례를 문헌고찰 과 함께 보고한다.
참고문헌
1. Jordan GL Jr. Pancreatic fistula. Am J Surg 1970;119:200- 207.
2. Fielding GA, McLatchie GR, Wilson C, Imrie CW, Carter DC. Acute pancreatitis and pancreatic fistula formation. Br J Surg 1989;76:1126-1128.
3. Takayama T, Kato K, Katada N, et al. Radiological demons- tration of spontaneous rupture of a pancreatic pseudocyst into the portal system. Am J Gastroenterol 1982;77:55-58.
4. Takayama T, Kato K, Sano H, Katada N, Takeichi M.
Spontaneous rupture of a pancreatic pseudocyst into the portal venous system. AJR Am J Roentgenol 1986;147:935- 936.
5. Sorensen EV. Subcutaneous fat necrosis in pancreatic disease.
A review and two new case reports. J Clin Gastroenterol 1988;10:71-75.
6. McCormick PA, Chronos N, Burroughs AK, McIntyre N, McLaughlin JE. Pancreatic pseudocyst causing portal vein thrombosis and pancreatico-pleural fistula. Gut 1990;31:561- 563.
7. Willis SM, Brewer TG. Pancreatic duct-portal vein fistula.
Gastroenterology 1989;97:1025-1027.
8. Van Steenbergen W, Ponette E. Pancreaticoportal fistula: a rare complication of chronic pancreatitis. Gastrointest Radiol 1990;15:299-300.
9. Skarsgard ED, Ellison E, Quenville N. Spontaneous rupture of
a pancreatic pseudocyst into the portal vein. Can J Surg 1995;38:459-463.
10. Yamamoto S, Takeshige K, Aradawa T, et al. Case report of a pancreatic pseudocyst ruptured into the splenic vein causing extrahepatic portal hypertension. Jap J Surg 1982;12:387-390.
11. Procacci C, Mansueto GC, Graziani R, et al. Spontaneous rupture of a pancreatic pseudocyst into the portal vein.
Cardiovasc Intervent Radiol 1995;18:399-402.
12. Demetrick DJ, Kelly JK. Variceal hemorrhage as a conse- quence of spontaneous rupture of a pancreatic pseudocyst into the splenic vein. Am J Gastroenterol 1989;84:1103-1105.
13. Hammar AM, Sand J, Lumio J, et al. Pancreatic pseudocys- tportal vein fistula manifests as residivating oligoarthritis, subcutaneous, bursal and osseal necrosis: a case report and review of literature. Hepatogastroenterology 2002;49:273-278.
14. Ko HS, Anders M. Diehl S, Dominguez E, Lohr M, Duber C.
Portal vein erosion and acute abdominal hemorrhage as a complication of acute pancreatitis. Abdom Imaging 2003;28:
700-702.
15. Potts JR 3rd. Pancreatic-portal vein fistula with disseminated fat necrosis treated by pancreaticoduodenectomy. South Med J 1991;84:632-635.
16. Zeller M, Hetz HH. Rupture of a pancreatic cyst into the portal vein. Report of a case of subcutaneous nodular and generalized fat necrosis. JAMA 1966;195:869-871.
17. Lee SH, Bodensteiner D, Eisman S, Dixon AY, McGregor DH. Chronic relapsing pancreatitis with pseudocyst erosion into the portal vein and disseminated fat necrosis. Am J Gastroenterol 1985;80:452-458.
18. Packeisen J, Klingen D, Grezella F. Spontaneous rupture of a pancreatic pseudocyst into the portal vein. Z Gastroenterol 2001;39:961-964.
19. Kozarek RA, Ball TJ, Patterson DJ, Freeny PC, Ryan JA, Traverso LW. Endoscopic transpapillary therapy for disrupted pancreatic duct and peripancreatic fluid collections. Gastroen- terology 1991;100:1362-1370.
20. Torres AJ, Landa JI, Moreno-Azcoita M, et al. Somatostatin in the management of gastrointestinal fistula. A multicenter trial. Arch Surg 1992;127:97-100.