The serious or fatal complications associated with c- holesteatoma prior to the antibiotic era have diminished remarkably, and intracranial complications now occur in less than 0.3 % of all cases (1). This incidence is not decreasing further, however; indeed, an increase is now apparent. Cholesteatoma of the temporal bone usually occurs in the attic (epitympanic cavity) and extends easi- ly into the mastoid antrum through the aditus. All com- plications of cholesteatoma are in fact related to bony erosion (2). The nature of the pathogenesis of bony change has provoked controversy, and various causes have been suggested. These include pressure phenome- na, the elaboration of collagenase by granulation tissue, invasive fibroblasts, and osteoclastic stimulation (3).
Common complications of cholesteatoma include ossic- ular erosion, labyrinthine fistula, facial nerve canal fistu-
la, and hearing loss (1), and the condition sometimes leads to serious and potentially fatal intracranial compli- cations including meningitis, dural sinus thrombosis, and parenchymal inflammation (2). High resolution computed tomography (HRCT) of the temporal bone has been quite useful for the diagnosis of cholesteatoma (4), but if bony erosion of the tegmen tympani or sinus plate occurs, or serious complications are suspected, M- RI is preferred (5).
The pages which follow provide a description of the diverse MR manifestations of the complications arising from atticoantral cholesteatoma.
MR Imaging
The typical MR characteristics of cholesteatoma are its isointensity to cerebral parenchyma, as seen on T1 weighted images, and its moderate hyperintensity on T2 weighted images (1, 2, 4-7), characteristics which are due to keratin materials (2, 4-6). When a contrast agent is administered, cholesteatoma other than those sur- rounded by granulation tissue do not show enhance- ment; when this tissue is present, there may be periph- eral rim enhancement (2) (Fig. 1). In order to distinguish non-enhancing cholesteatoma from enhancing granula-
Complications of At t i c o a n t ral Cholesteato ma:
MR Manifestations
1Jeong Hyun Lee, M.D., Ho Kyu Lee, M.D., Soo Mi Lim, M.D., Ji Hoon Shin, M.D., Choong Gon Choi, M.D., Dae Chul Suh, M.D., Kwang Sun Lee, M.D.2
Cholesteatoma of the temporal bone usually occurs in the attic (epitympanic cav i t y ) and extends easily into the mastoid antrum through the aditus ad antrum. Since atti- coantral cholesteatoma can lead to clinically serious complications, successful patient management requires an accurate knowledge of the extent of the condition. All com- plications of cholesteatoma are in fact related to bony erosion and may be classified as l a by r i n t h i t i s, extracranial complication, meningitis, dural sinus obstruction, or p a r e n c hymal inflammation. This paper describes the diverse MR manifestations of the complications arising from atticoantral cholesteatoma.
Index words :E a r, MR C h o l e s t e a t o m a
1Department of Diagnostic Radiology, University of Ulsan College of Medicine, Asan Medical Center
2Department of Otolaryngorhinology, University of Ulsan College of Medicine, Asan Medical Center
Received September 7, 1999 ; Accepted, November 25, 1999
Address reprint requests to : Ho Kyu Lee, M.D., Department of Diagnos- tic Radiology, Asan Medical Center
#388-1 Poongnap-dong, Songpa-gu, Seoul 138-736 Tel. 82-2-2224-4400/4371
Fax. 82-2-476-4719
E-mail: [email protected]
tion tissue, or to depict enhancement of the labyrinth or facial nerve which suggests inflammatory change in- duced by bony fistula, the use of contrast-enhanced M- RI is important.
C o m p l i c a t i o n s
L a b y r i n t h i t i s
Labyrinthine fistula is one of the common complica- tions of cholesteatoma and is associated with consider- able morbidity; most authors have reported an inci- dence of 5-10 % (4). Due to its proximity, the most com- mon site of bony fistula is the lateral semicircular canal, and this is, therefore, the site at which labyrinthitis com- monly occurs (5, 8, 9). The imaging finding of labyrinthi- tis is enhancement of the membranous labyrinth, as
seen on contrast-enhanced T1-weighted images (1, 7, 10). Such enhancement is normally faint and is typically detected during the subacute stage of the disorder (11) (Fig. 2). Progression to the chronic stage leads to fibrob- last proliferation. T2-weighted images disclose fibrous replacement of the fluid-filled spaces of the labyrinth.
Further degeneration results in labyrinthine ossification over a period varying between several months and years. Cochlear fistula is less common and is usually lo- cated at the level of the promontory between the round and oval windows occurring secondary to pars tensa c- holesteatoma. Facial nerve paresis occurs preoperative- ly in approximately one percent of cholesteatoma pa- tients and is usually caused by bony erosion of the facial nerve canal (1).
Fig. 1. MR findings of atticoantral cholesteatoma
A . On axial T1-weighted image, cholesteatoma is hypointense (asterisk) to the cerebral white matter.
B . On T2-weighted image, it is a moderately hyperintense lesion, mixed with a hypointense portion (asterisk) within the atti- coantral cavity.
C .Contrast-enhanced T1-weighted image shows a non-enhanced mass (asterisk) within the atticoantral cavity. Note peripheral thin rim enhancement (arrows) which means inflammatory change of the atticoantral cavity.
A B C
Fig. 2. Labyrinthitis
A . Axial precontrast T1-weighted image shows focal hyperintensity at the vestibule and lateral semicircular canal (long arrows).
B . Contrast-enhanced T1-weighted image shows strong enahancement of the membranous labyrinth of the vestibule and lateral semicircular canal (long arrows). It was caused by a bony fistula of the lateral semicircular canal.
Fig. 3. Subperiosteal abscess
Subperiosteal abscess is associated with soft tissue enhancement in preauricular area (open arrows) on contrast-enhanced axial T1- weighted image.
A B 3
Extracranial inflammation
Cholesteatoma may spread via a bony defect in the ex- ternal mastoid cortex to form a subperiosteal abscess. In general, because of the thin trabecular bone found there, this is found in the postauricular region (1, 7). If the infection spreads preferentially along the zygomatic arch, preauricular extension is, however, also possible (7) (Fig. 3). A Bezold abscess presenting as a tender mass beneath the sternocleidomastoid muscle may be the re- sult of diffusion through the large, thin-walled cells in- ternal to the digastric groove of the mastoid tip. Now that antibiotics are common, this complications, howev- er, rarely encountered.
M e n i n g i t i s
Meningitis is a serious complication, and may be local- ized or diffuse. A bony defect of the tegmen tympani permits access to the adjacent dura, and acute pyogenic meningitis may develop via direct extension of the in- flammatory process through the defect (Fig. 4). If pa- tients with cholesteatomas are not treated promptly, lo-
calized meningitis can spread over a wider area and leads to more serious complications such as choroid plexitis, ventriculitis or extracerebral empyema (Fig. 5, 6). The last-mentioned occurs in the subdural or epidur- al space, in which cresentic or lentiform extra-axial fluid collections mildly hyperintense to CSF are seen on T2- weighted images. Contrast-enhanced T1-weighted im- ages show strong enhancement and thickening of the meninges, a phenomenon which occurs on cerebral convexities or in the interhemispheric fissure.
Subarachnoid space compromised by extensive fibropu- rulent exudate may cause extraventricular obstructive hydrocephalus, whereas ventriculitis with cerebral aqueductal ependymitis leads to intraventricular hydro- cephalus (12).
Dural sinus obstruction
Bony defects in the internal mastoid cortex permit ac- cess to the sigmoid sinus and adjacent dura (5). Simple obstruction of the dural sinus may occur through extrin- sic compression by a large atticoantral cholesteatoma,
A B
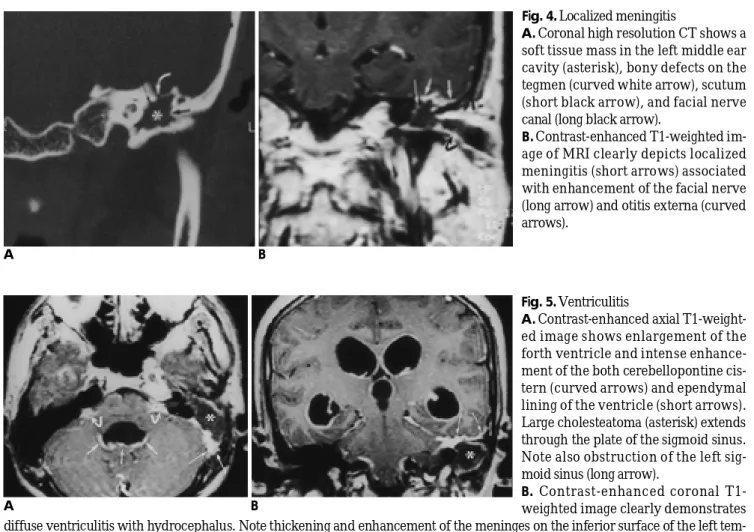
Fig. 4. Localized meningitis
A. Coronal high resolution CT shows a soft tissue mass in the left middle ear cavity (asterisk), bony defects on the tegmen (curved white arrow), scutum (short black arrow), and facial nerve canal (long black arrow).
B. Contrast-enhanced T1-weighted im- age of MRI clearly depicts localized meningitis (short arrows) associated with enhancement of the facial nerve (long arrow) and otitis externa (curved a r r o w s ) .
Fig. 5. V e n t r i c u l i t i s
A . Contrast-enhanced axial T1-weight- ed image shows enlargement of the forth ventricle and intense enhance- ment of the both cerebellopontine cis- tern (curved arrows) and ependymal lining of the ventricle (short arrows).
Large cholesteatoma (asterisk) extends through the plate of the sigmoid sinus.
Note also obstruction of the left sig- moid sinus (long arrow).
B. Contrast-enhanced coronal T1- weighted image clearly demonstrates diffuse ventriculitis with hydrocephalus. Note thickening and enhancement of the meninges on the inferior surface of the left tem- poral lobe (long arrows) adjacent to the cholesteatoma (asterisk), which suggests localized meningitis.
A B
but dural sinus thrombophlebitis may occur through bony defects in the sigmoid sinus plate via direct exten- sion (Fig. 7). The latter gives rise to hematogenous dis- semination and extensive thrombophlebitis (7). On occa- sion, MRI reveals the thrombosis either directly, within the lumen of the dural sinus or indirectly, as the absence of flow void on spin-echo images and of flow-related en- hancement on gradient-echo images (1, 7). After injec- tion of the contrast agent, an occluded sinus and intralu- minal thrombus appear as filling defect surrounded by enhanced engorged dural cavernous spaces, meningeal tributaries, or collateral venous channels producing the so-called empty delta sign (12). Due to increased venous pressure, enhancement and thickening of the meninges
and tentorium occur on the ipsilateral side, and a ve- nous ischemic lesion may sometimes be associated. For evaluation of this dangerous clinical condition, MR venography is useful (7).
Parenchymal inflammation
Brain abscess is one of the most serious complications.
Initially, infectious agents can cause focal cerebritis, which leads to a brain abscess via direct extension thr- ough bony defects (Fig. 8). The cause may, however, al- so be either retrograde thrombophlebitis or adjacent empyema or meningitis. The temporal lobe is the most vulnerable site of the brain (1, 7, 12). On MR, the central necrotic area is typically hyperintense to cerebral white
A B
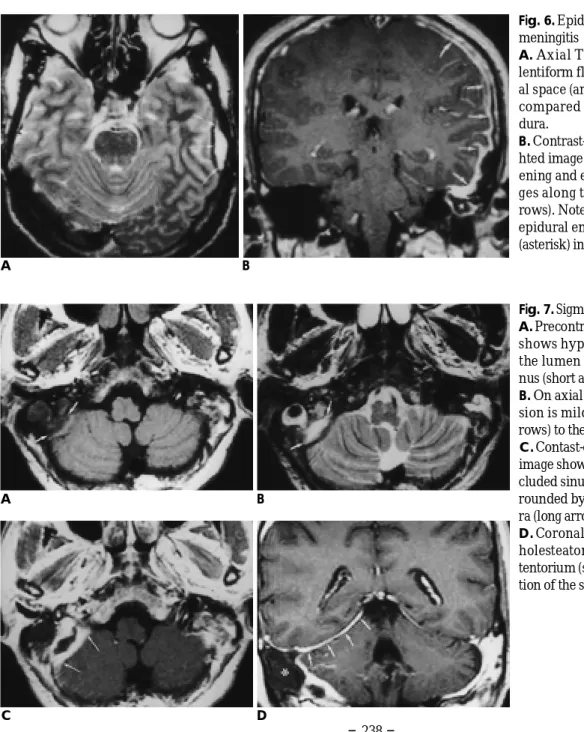
Fig. 6. Epidural empyema with diffuse m e n i n g i t i s
A. Axial T2-weighted image shows lentiform fluid collection in the epidur- al space (arrows) mildly hyperintense compared to CSF with the thickened d u r a .
B . Contrast-enhanced coronal T1-weig- hted image demonstrates diffuse thick- ening and enhancement of the menin- ges along the cerebral convexity (ar- rows). Note close relationship between epidural empyema and cholesteatoma (asterisk) in the left antral cavity.
Fig. 7. Sigmoid sinus thrombophlebitis A . Precontrast axial T1-weighted image shows hypointense thrombus within the lumen of the enlarged sigmoid si- nus (short arrows).
B. On axial T2-weighted image, the le- sion is mildly hyperintense (short ar- rows) to the CSF.
C .Contast-enhanced axial T1-weighted image shows relatively hypointense oc- cluded sinus and periosteal abscess sur- rounded by the enhanced engorged du- ra (long arrows).
D . Coronal MR image shows antral c- holesteatoma (asterisk) and engorged tentorium (short arrows) due to obstruc- tion of the sigmoid sinus.
A B
C D
matter, as seen on proton-density and T2-weighted im- ages. The thin-walled, well-demarcated rim appears iso- to mildly hyperintense on T1-weighted images, iso- to relatively hypointense on proton-density and T2-weight- ed images, and enhances intensely following contrast administration. Peripheral edema is usually present.
In conclusion, MRI can give useful information about various complications of atticoantral cholesteatoma, es- pecially when bony defects of the tegmen tympani or si- nus plate are revealed by HRCT of the temporal bone.
MRI, including the use of a contrast agent, plays an im- portant role in demonstrating the serious complications which can arise from a cholesteatoma. An understand- ing of the variety of these will facilitate the evaluation of MRI of the temporal bone in patients with atticoantral c- h o l e s t e a t o m a .
R e f e r e n c e s
1 . Swarts JD, Harnsberger HR. Imaging of the temporal bone. 3rd ed.
New York: Thieme, 1998:85-107, 272-280
2 . Swartz JD. Cholesteatomas of the middle ear: diagnosis, etiology, and complications. Radiol Clin North Am 1 9 8 4 ; 2 2 ( 1 ) : 1 5 - 3 4 3 . Robert Y, Dubrulle F, Careasset S, et al. Petrous bone extension of
middle ear acquired cholesteatoma. Acta Radiol 1 9 9 6 ; 3 7 : 1 6 6 - 1 7 0 4 . Ishii K, Takahashi S, Kobayashi T, Matsumoto K, Ishibashi T. MR
imaging of middle ear cholesteatomas. J Comput Assist Tomogr 1 9 9 1 ; 1 5 ( 6 ) : 9 3 4 - 9 3 7
5 . Som PM, Curtin HD. Head and neck imaging. 3rd ed. St. Louis:
Mosby, 1996:1391-1405
6 . Martin N, Sterkers O, Nahum H. Chronic inflammatory disease of the middle ear cavities: Gd-DTPA-enhanced MR imaging.
Radiology 1 9 9 0 ; 1 7 6 : 3 9 9 - 4 0 5
7 . Phelps PD, Wright A. Imaging cholesteatoma. Clin Radiol 1 9 9 0 ; 4 : 1 5 6 - 1 6 2
8 . Silver AJ, Janecka I, Wazen J, Hilal SK, Rutledge JN. Complicated cholesteatomas: CT findings in inner ear complications of middle ear cholesteatomas. Radiology 1 9 8 7 ; 1 6 4 : 4 7 - 5 1
A B
C D
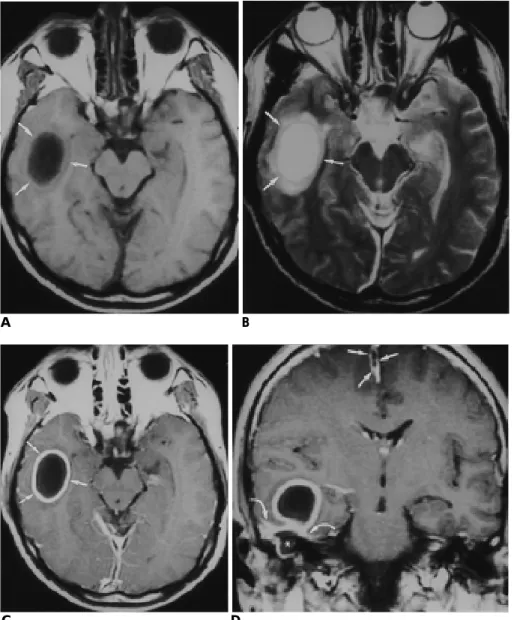
Fig. 8. Brain abscess and subdural em- p y e m a
A . Precontrast axial T1-weighted image shows hypointense lesion with isoin- tense thin, well-demarcated rim (ar- rows) in the right temporal lobe.
B . On axial T2-weighted image, the central hypointense lesion and the rim becomes hyperintense to the brain parenchyma (arrows). Note peripheral hyperintensity due to edema around the abscess.
C .Contrast-enhanced T1-weighted im- age shows strong enhancement of the rim of the abscess cavity (arrows).
D . Contrast-enhanced coronal T1- weighted image shows cholesteatoma (asterisk) in the right attic adjacent to thick enhancing meninges (curved ar- rows) and abscess cavity. Note subdur- al empyema (short arrows) in the inter- hemispheric space.
9 . Cummings CW, Fredrickson JM, Harker LA. Otolaryngology - Head and Neck Surgery. St Louis: Mosby, 1993:2833-2855
1 0 . Seltzer B, Mark AS. Contrast enhancement of the labyrinth on MR scans in patients with sudden hearing loss and vertigo: evidence of labyrinthine disease. AJNR 1 9 9 1 ; 1 2 : 1 2 - 1 9
1 1 . Swartz JD. Sensorineural hearing deficit: a systematic approach based on imaging findings. Radiographics 1 9 9 6 ; 1 6 : 5 6 1 - 5 7 4 1 2 . Osborn AG. Diagnostic neuroradiology. St. Louis: Mosby, 1994:680-
6 9 4
대한방사선의학회지 2 0 00;42: 2 35- 2 4 0
상고실동 진주종 합병증의 자기공명영상 소견
11울산대학교 의과대학 서울중앙병원 진단방사선과
2울산대학교 의과대학 서울중앙병원 이비인후과
이정현・이호규・임수미・신지훈・최충곤・서대철・이광선2
측두골에 위치한 진주종은 대개 상고실에 발생하고 유돌동구(aditus ad antrum) 를 통해 유양동 ( m a s t o i d antrum) 으로 쉽게 파급된다. 진주종의 합병증은 임상적으로 매우 심각한 결과를 초래할 수 있기 때문에 질병의 정확한 범위를 아는 것이 적절한 치료를 시행하는데 있어 매우 중요하다. 모든 진주종의 합병증은 골 미란에 의 한 것으로 때때로 심각하고도 치명적인 두개내 합병증을 초래할 수 있다. 본 화보에서는 이들 합병증을 미로염, 두개외 합병증, 수막염, 경막동 폐쇄, 그리고 뇌실질 염증으로 나누어 진주종의 MR 상의 특징과 다양한 합병증 을 보여 주고자 한다.