당뇨병환자의 수술 전 심혈관계 위험도 평가
Preoperative Assessment of Cardiac Risk in the Patient with Diabetes
동국대학교 의과대학 내과학교실
김경아
Kyoung Ah Kim
Department of Medicine, Dongguk University IIsan Hospital, Dongguk University School of Medicine, Goyang, Korea
교신저자: 김경아, 경기도 고양시 일산구 식사동 814번지 동국대학교병원 내분비대사내과, E-mail: kyoung-ah.kim@dumc.or.kr
서 론
수 술 과 전 신 마 취 에 따 른 심 혈 관 계 사 망 률 은 0.3%이고, 비치명적 심근경색이 1%에서 발생한다.
수술기주위(perioperative) 사망의 40%는 심장사 (cardiac death)에 의한다. 당뇨병은 관상동맥질환과 무증상허혈증을 동반하는 경우가 많으므로[1] 수술기 주위 심혈관질환의 이환율과 사망률은 일반인에 비해 2~3배 증가한다[2,3]. 특히 인슐린치료를 받는 당뇨병환자는 비심장수술을 시행받는 환자에서의 심장위 험도를 예측하기 위한 revised cardiac risk index (RCRI) 위험인자 중 하나이다[4]. 따라서 당뇨병환자는 수술 전 심혈관질환에 대한 충분한 평가가 필요하다.
그러나 주요한 수술을 받는 모든 환자에게 수술 전 비침습적 심장검사를 시행할 근거는 없다. 따라서 수술기주위 위험도 평가를 하여 심장검사를 시행할지 여부를 결정하고 예방적 약물 치료를 시작하는 것이 중요하다[4]. 본 리뷰에서는 당뇨병환자에서 비심장질환 수술시 수술기주위 심혈관질환 위험도 평가를 고찰 하겠다.
임상적 평가: 병력청취/이학적 검진
각 개인의 수술 전 위험도는 환자의 병력, 동반질환, 받고자 하는 수술 유형, functional capacity, 이학적 검진, 심전도 검사로 유추할 수 있다. 주의 깊은 병력
Abstract
Focused Issue - 당뇨병과 수술
Approximately 50% of people with diabetes will at some point undergo surgery related to their disease. Since patients with diabetes mellitus are four times more likely to have silent ischemia and coronary artery disease compared to the risk of non-diabetic patients, they are at a higher risk for perioperative complications.
Preoperative evaluation can identify many patients at increased risk of an adverse cardiac event, and appropriate perioperative management can reduce that risk. Although there is great potential to reduce perioperative cardiovascular risk, it is also impractical to perform cardiovascular testing prior to non-cardiac surgery in all patients. Therefore, it is important to determine perioperative risk and the appropriateness of cardiac testing and to provide prophylactic treatment to reduce risk. Perioperative cardiac risk stratification is determined by comorbidity, other cardiovascular risk factors, functional status, and type of surgery. By categorizing the cardiac risk, physicians can perform surgery in low risk patients without the need for cardiac testing. When preoperative risk assessment identifies intermediate- and high-risk patients, further cardiac testing might be warranted. This article reviews the perioperative evaluation of patients with diabetes with a clinical focus on cardiovascular risk. (J Korean Diabetes 2011;12:142-146)
Keywords: Diabetes mellitus, Surgery, Perioperative care, Risk management, Coronary artery disease 142The Journal of Korean Diabetes
143The Journal of Korean Diabetes
청취는 수술 위험도가 높은 심혈관질환이나 동반질환을 발견하는데 있어 중요하다. 특히 당뇨병에서는 관상동맥 질환 위험이 높고 무증상허헐증을 동반하는 가능성이 많다. 환자의 병력상 active cardiac conditions을 가지는 경우는 수술을 연기하고 평가를 해야 된다(Table 1)[4]. 이는 다음과 같다.
① 불안정 관상동맥 증후군 • 불안정 또는 심한 협심증 •최근의 심근경색
② 비대상성 심부전
③ 주요한 부정맥
④ 심한 판막질환
또한 환자의 functional capacity를 평가하여 수술의 위험도를 예측해야 한다.
수술-특이적인 위험
수술 방법에 따른 수술 위험도가 달라지므로 수술 전 심혈관질환 평가를 하는데 중요한 요소가 된다. 그 이유로는 첫째, 일부 질환들은 심혈관질환의 위험인자를 같이 공유하는 경우가 많다. 예를 들어 vascular surgery를 받는 환자는 관상동맥질환을 동반할 가능성이 높다. 둘째, 수술 자체로 급격한 심장스트레스를 유발할 수 있다. 예를 들어 응급 수술은 수술기주위 심장위험이 2~5배로 증가한다. 수술방법에 따른 위험도는 Table 1과 같이 분류한다.
수술기주위 심혈관계사건 위험도의 임상적 예측인자
긴급하지 않은 주된 비심장수술을 받게 되는 안정된 환자에 있어서 수술기주위 심혈관계사건의 위험도를 예측하기 위한 여러 가지 risk index가 소개되고 있다.
이중 1999년 Lee 등이 제시한 revised cardiac risk index가 많이 쓰이고 있다[5]. 이는 다음과 같은 6개의 위험인자로 구성되 있다.
①2 고위험 수술(intraperitoneal, intrathoracic, suprainguinal vascular)
②2 허혈성심질환(심근경색 병력 또는 활동성 협심증, 설하 니트로글리세린 사용자, 최근 스트레스 테스트상 이상소견, 심전도상 Q waves, 관상동맥 재개통술의 병력과 진행 중인 흉통)
③2 울혈성 심부전
④2 뇌혈관질환(뇌졸증, 일과성 허혈발작)
⑤2 수술 전 인슐린 치료를 하는 당뇨병
⑥2 수술 전 크레아티닌 > 2mg/dL
위험인자가 많을수록 수술의 위험도는 높아지며 RCRI가 0, 1, 2 또는 3개 이상 시 주요 심장사건이 발생할 확률은 각각 0.4%, 0.9%, 7%, 11%이다. 나이를 보정하고 고혈압을 포함한 modified Lee index도 소개되고 있다[6,7].
비심장수술에서 심혈관계 평가 알고리즘
American College of Cardiology (ACC)/American
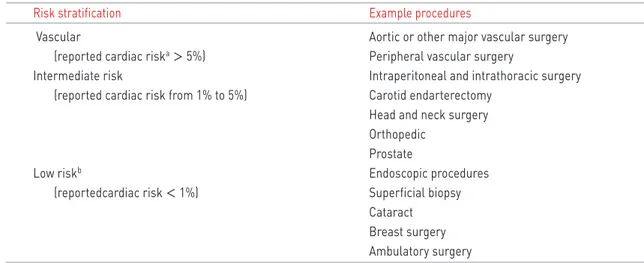
Table 1. Cardiac risk stratification for noncardiac surgical procedures
Risk stratification Example procedures
Vascular Aortic or other major vascular surgery (reported cardiac riska > 5%) Peripheral vascular surgery
Intermediate risk Intraperitoneal and intrathoracic surgery (reported cardiac risk from 1% to 5%) Carotid endarterectomy
Head and neck surgery
Orthopedic
Prostate
Low riskb Endoscopic procedures
(reportedcardiac risk < 1%) Superficial biopsy
Cataract
Breast surgery
Ambulatory surgery
Adapted from Fleisher et al. Circulation 2009;120:e169-276 [4].
a
Combined incidence of cardiac death and non-fatal myocardial infarction.
b
These procedures do not generally require further preoperative cardiac testing.
Heart Association (AHA)에서 수술기주위 심혈관계 위험도에 관한 평가 및 조치에 관해 다음과 같은 가이드라인을 제시했다. 당뇨병환자에서도 이 가이드 라인에 따른 검사 진행여부를 결정한다(Fig 1).
1) Step 1; 일단 수술이 응급상황인지 판단하는 것이 중요하다. 환자상태 또는 수술 적응증에 따라 심혈관계 질환에 대한 평가나 치료 없이 수술을 진행해야 되는 경우가 있다. 응급 비심장수술이 필요한 환자는 수술을 진행하고 수술 후에 수술기주위 감시와 함께 위험도 계층화와 위험인자 관리가 필요하다. 응급 수술이 아니라면 step 2로 진행한다.
2) Step 2; Active cardiac condition이 있는지 평가하고 만약 이에 해당되면 수술을 연기하고 A C C/A H A 가이드라인에 따른 평가와 치료를 한 후 수술을 결정한다. 많은 경우 추후 치료방침을 정하기 위한 심혈 관조영술을 시행하게 된다. 만약 이런 상태가 아니라면 step 3로 진행한다.
3) Step 3; 수술의 위험도를 판단한다. Vascular, intermediate, low risk로 분류하며, low-risk surgery를 하는 환자들은 대부분 추가적인 평가 없이 예정대로 수술을 진행한다. 이런 환자들에 있어서는 심혈관계 검사를 하더라도 대개는 환자 관리의 방침이 바뀌지 않기 때문에 추가적 검사나 조치 없이 예정된 수술을 진행한다.
4) Step 4; functional capacity를 평가한다. Metabolic equivalents (METs)가 4 이상이고 증상이 없는 경우 예정대로 수술을 진행한다.
5) Step 5; functional capacity가 불량하거나 (4 METs 미만) 거동이 불편하여 functional capacity를 평가할 수 없는 경우에 해당된다. 4 METs 미만은 1~2블록을 걷지 못하거나, 가벼운 집안일을 못하는 경 우, 계단이나 언덕을 오르지 못하는 경우 등에 해당된다.
이때는 다음의 clinical risk factor가 있는지 확인한다.
①2 허혈성심질환
②2 대상성 또는 기존의 심부전 Focused Issue - 당뇨병과 수술
144The Journal of Korean Diabetes
Emergent noncardiac surgery (1)
(2)
(3)
(4)
(5)
Surgery Preoperative surveillance &
postoperative risk stratification
& risk factor management Active cardiac conditions
Clinical risk factors
Low-risk surgery Proceed with planned surgery
Proceed with planned surgery
Proceed with planned surgery
Proceed with planned surgery with HR controla or consider noninvasive testing if it will change management No (elective)
No
No
No or unknown
0
Consider Surgery Evaluate & treat per
ACC/AHA guidelines
Functional capacity
≥4 METs without symtoms
1~2 ≥3
Vascular
surgery Vascular
surgery Intermediate-
risk surgery
Consider testing if it will change management Yes
Yes
Yes
Yes
Fig. 1.
Cardiac evaluation and care algorithm for noncardiac surgery. HR, heart rate; MET, metabolic equivalents.
aConsider perioperative beta-blockade for populations in which this has been shown to reduce cardiac morbidity/
mortality.
145The Journal of Korean Diabetes
③2 당뇨병
④2 신부전
⑤2 뇌혈관질환
Clinical risk factor의 개수와 수술방법의 위험도에 따라 추가적인 평가 및 조치 여부를 결정하게 된다.
Clinical risk factor가 없는 경우는 수술방법의 위험도에 상관없이 추가적인 검사 없이 예정대로 수술을 진행하는 것이 적절하다. 그러나 당뇨병환자는 다음 카테고리로 생각한다.
①2 3개 이상의 clinical risk factor를 갖고 vascular surgery를 예정하면 치료방침의 변경이 예상될 경우 비침습적 검사를 시행한다.
②2 3개 이상의 clinical risk factor를 갖고 intermediate surgery, 또는 1~2개의 clinical risk factor를 갖고 vascular/intermediate surgery가 예정되 있으면 심박수 조절을 하면서 계획대로 수술을 진행한다.
또는 비침습적 검사를 통하여 치료방침의 변경이 예상된다면 추가적으로 비침습적 검사를 시행할 수 있다.
수술기주위 약물치료
관상동맥질환을 가진 환자에서 베타차단제의 사용은 비심장수술 전후의 심근허혈의 감소, 심근경색 및 사망의 위험성을 감소시키는 것으로 보고되고 있다. 베타차 단제는 수술 이전부터 협심증, 증상이 있는 부정맥, 고혈 압 또는 현재의 가이드라인 적응증에 따라 써온 환자에서 는 금기증이 없다면 지속한다. 그러나, 기존에 베타차단 제를 써오지 않았다면 고용량의 베타차단제를 용량 titration 없이 관례적으로 사용하는 것은 유용성이 없고 때로는 해로울 수 있다. 가능하면 수술 전 수일 내지 수주 전에 시작하는 것이 좋고 지속성 제재가 속효성 제 재보다 좋을 것으로 보고되었다.
수술이전부터 스타틴을 복용하던 환자는 계속 복용 하는 것이 좋다. 또한 vascular surgery에서도 스타틴의 사용이 권고된다.
결 론
주요한 비심장수술을 받는 대부분의 환자들은 수술기 주위 심혈관사건이 발생할 위험이 크다.
적절한 수술전 평가는 추가적인 심장검사가 필요한 고위험군 환자를 식별해내고 적절한 치료를 시작함 으로써 수술기주위, 그리고 장기적인 결과의 호전을 가져 온다. 수술기주위 검사는 환자의 관리에 명백히 영향을
미칠 수 있는 경우에 제한적으로 시행하여야 하며 일반 적으로, 추가적인 심장검사와 재개통술의 적응증은 수술이 아닌 일반적인 상황에서와 유사하다. 단, 수술의 긴급성, 환자의 위험 인자, 수술자체의 위험 등 여러 요 소를 고려하여 판단한다. 당뇨병환자는 무증상 관상 동맥질환의 유병률이 높으므로 적응증이 되면 추가적인 비침습적 스트레스 검사를 고려한다.
허혈성심질환을 발견하기 위해 가장 흔히 쓰이는 비침습적 심장 스트레스 테스트로는 treadmill 또는 bicycle ergometry이 있다. 그러나, 비심장수술을 받는 환자의 상당수가 동반질환으로 운동능력이 제한돼 있으므로 이때는 약물부하 테스트(d o b u t a m i n e echocardiography, dipyridamole myocardial perfusion scintigraphy)를 시행한다.
수술기 주위 심장위험을 최소화하기 위해 약물치료로 관상동맥질환이 의심되는 환자들은 베타차단제, 스타 틴을 투여한다. 수술기주위 심장 위험도를 줄이기 위해 예방적 관상동맥재개통술 실시하는 것은 효용성이 없음 이 시사되었다.
비심장수술전 평가는 많은 환자들에의 단기적, 장기적 심장 위험도에 대한 종합적인 평가를 제공해주어 수술 기주위 위험을 줄일 뿐 아니라, 적절한 근거에 기인한 치 료로 장기간 결과를 호전시킬 수 있다.
참고문헌
01. S
Airaksinen KE. Silent coronary artery disease in diabetes--a feature of autonomic neuropathy or accelerated atherosclerosis? Diabetologia 2001;44:259- 66.02.S
Gu W, Pagel PS, Warltier DC, Kersten JR. Modifying cardiovascular risk in diabetes mellitus. Anesthesiology 2003;98:774-9.03.S
Rabbitts JA, Nuttall GA, Brown MJ, Hanson AC, Oliver WC, Holmes DR, Rihal CS. Cardiac risk of noncardiac surgery after percutaneous coronary intervention with drug-eluting stents. Anesthesiology 2008;109:596-604.04.S
Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof EL, Fleischmann KE, Freeman WK, Froehlich JB, Kasper EK, Kersten JR, Riegel B, Robb JF. 2009 ACCF/AHA focused update on perioperative beta blockade incorporated into the ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American college of cardiology foundation/American heart association task force on practice guidelines. Circulation 2009;120:e169- 276.
05.S
Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, Sugarbaker DJ, Donaldson MC, Poss R, Ho KK, Ludwig LE, Pedan A, Goldman L.146The Journal of Korean Diabetes
Focused Issue - 당뇨병과 수술
Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999;100:1043-9.
06.S
Boersma E, Kertai MD, Schouten O, Bax JJ, Noordzij P, Steyerberg EW, Schinkel AF, van Santen M, Simoons ML, Thomson IR, Klein J, van Urk H, Poldermans D.Perioperative cardiovascular mortality in noncardiac surgery: validation of the Lee cardiac risk index. Am J
Med 2005;118:1134-41.