472
서 론
소화관에 만성적인 자극이 지속되면 상피세포는 세포생 성 불안정성(cytogenetic instability)의 결과로 상이한 형태의 상피로 바뀌면서 여러 종류의 점액을 만들게 된다.(1) 위암 은 정상적인 위 점막의 점액분비 세포나 장상피화생이 일 어난 부위에서 발생한다.(2) 많은 위암에서 점액을 분비하 는데 세포 내로 분비되면 소위 인환 세포형(signet ring cell type)이라 분류되고 세포 외로 분비되면 종양세포가 풍부한 점액 풀에 부유하는 양상을 보이는데 이 경우는 성장시 그 부피가 크고 절단면은 반투명하면서 반짝이는 특성을 가진 점액성 위선암으로 분류된다.(2) 점액성 위선암은 전체 위 선암의 3∼7%를 차지하는 드문 조직형이다.(3-5) 연구자에 따라 점액성 위선암의 예후가 불량하다는 보고(3)와, 다른 조직형과 비교하여 종양의 크기, 림프절 전이 정도, 병기, 치유 절제율 등 대부분의 임상병리학적 인자들이 비슷한 생물학적 특성을 보이고 예후도 더 불량하지 않다는 보고 (4) 및 분화도가 좋은 점액성 위암의 경우는 오히려 다른 조직형에 비하여 예후가 좋다는 보고(2)가 있어 이의 임상 병리학적 특성을 이해하는 것이 필요한 시점이라 하겠다.
이에 저자들은 위선암을 점액성 위선암과 비점액성 위선암 으로 구분하여 그들의 여러 임상병리학적 인자들의 특성 및 예후를 비교 분석하였다. 또한 점액성 위선암은 점액의 점유 정도 및 세포의 분화도에 따라서도 구분하여 각각의
점액성 위 선암의 임상병리학적 특성
한양대학교 의과대학 외과학교실, 1병리학교실
권 성 준․박 재 정․백 승 삼1
책임저자:권성준, 서울시 성동구 행당동 17 ꂕ 133-792, 한양대학교병원 외과 Tel: 02-2290-8453, Fax: 02-2281-0224 E-mail: [email protected]
접수일:2003년 12월 4일, 게재승인일:2004년 3월 20일
Clinicopathologic Characteristics of Mucinous Gastric Adenocarcinoma
Sung Joon Kwon, M.D., Jae Jung Park, M.D. and Seung Sam Paik, M.D.1
Purpose: Clinicopathological characteristics of mucinous gastric adenocarcinomas (MGC) are unclear. Also, whether the surgical results of a MGC are unfavorable is still con- troversial. A tumor is defined as a MGC when more than 30% of the tumor area has mucin pools. Also, MGC are subdivided into the well-differentiated (WD) and poorly dif- ferentiated (PD) types, according to the degree of glandular formation of the tumor cells. To clarify the significance of MGC, the clinicopathological profiles and prognoses of patients were studied.
Methods: Thirty-four patients with MGC and 1,036 with non-mucinous gastric adenocarcinomas (NMGC) who were operated on between 1992 and 2002 at the Department of Surgery, Hanyang University Hospital, were included. Pa- tients were evaluated with regard to age, gender, tumor location, size, depth of wall invasion, lymph node status, distant metastasis, stage at presentation, lymphatic and vas- cular permeation, operative curability, and preoperative serum levels of CEA and CA19-9.
Results: MGC tumors, compared with NMGC tumors, had larger sizes (8.0 vs. 5.9 cm), more frequent incidences of T2 or more invasion (91 vs. 66%), positive lymph node meta- stasis (85 vs. 57%), distant metastasis (18 vs. 6%), stage III and IV (74 vs. 45%), noncurative surgery (32 vs. 10%), lymphatic permeation (88 vs. 63%), and abnormal serum CEA level (32 vs. 14%). However, the overall survival rate of those patients with a MGC was not significantly different from that of those with a NMGC. With a MGC, there was no significant correlation between the degree of mucin content and the prognosis. Conversely, the survival rate was higher
in the WD than in the PD types (100 vs. 45%, P=0.0185).
Conclusion: The mucinous histological type itself is of no prognostic significance in patients with gastric carcinomas.
The biological behavior of MGC is determined by the degree of glandular formation of the tumor cellss (i.e., histologic differentiation). (J Korean Surg Soc 2004;66:472-477) Key Words: Gastric cancer, Mucinous type, Nonmucinous
type
중심 단어: 위암, 점액형, 비점액형
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Departments of Surgery and 1Pathology, College of Medi- cine, Hanyang University, Seoul, Korea
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 임상병리학적 특성을 비교 분석하였다.
방 법
1992년 7월부터 2002년 2월까지 한양대학교병원 외과에 서 위선암으로 진단받고 수술받은, 1,070명의 추적이 가능 한 환자를 대상으로 하였다. 대상 환자들의 조직절편은 H&E 염색 후 현미경적 관찰을 시행하여 종양 면적의 30%
이상에서 세포외성 점액 풀(mucin pools)이 있는 경우를 점 액성 위선암으로 정의하였다. 모든 환자에 있어 성별, 나이, 종양의 크기 및 위치, 위벽 침윤 정도, 림프절 전이상태, 원 격전이 여부, 복막 파종 여부, 간 전이 여부, 병기, 위 절제범 위, 림프관 침습 여부, 혈관 침습 여부, 신경주위 침윤 여부, 수술 전 CEA/CA19-9 혈중 농도, 치유도에 대하여 생존 여 부 등을 후향적으로 조사하였다. 병기 구분은 제5판 UICC TNM classification의 규약(6)을 따랐다. 수술 중 종양이 완전 히 제거되었고, 수술 후 절제연에 대한 조직검사에서 5 mm 이내에 암세포가 없는 경우를 치유 절제예로 정의하였다.
최종 추적 검사일은 2003년 6월 30일로 하였으며 추적률은 97.7% (1,070/1,095)였고 추적 기간의 중간치는 37개월 (2∼
130개월)이었다. 통계적 유의성에 대한 검사는 X2 test 및 student t-tests로 하였으며 생존곡선은 Kaplan-Meier 방법에 의하여 구하였고, 생존율의 차이는 log rank test로 구하였 다. 통계분석을 위하여 SPSS 9.0 for Window Program (SPSS Inc. Chicago, Illinois, U.S.A.)이 사용되었고 통계적 유의성은 P값이 0.05 이하인 경우로 하였다.
결 과
1) 임상 병리학적 인자
34예의 점액성 위선암과 1,036예의 비점액성 위선암의 임상 병리학적 인자 가운데 성별, 나이, 종양의 위치, 위 절 제 범위, 혈관 침습 여부, 신경 주위 암 침윤 여부, 술 전 CA19-9 혈중 농도는 통계적으로 유의한 차이를 보이지 않 았다.
그러나 점액성 위선암은 비점액성 위선암에 비하여 통계 적으로 유의하게 위벽 침윤 정도가 깊고, 전이 림프절의 빈 도가 높고, 원격전이 빈도가 높았다. 또한 진행된 병기예의 빈도가 높았고, 림프관 암침윤의 빈도가 높고, 비치유 절제 예의 빈도가 높았으며, 종양의 크기가 크고, 술 전 CEA 혈 중 농도가 높은 경우가 많았다(Table 1).
점액성 위선암의 분화도(Fig. 1)에 따른 임상병리학적 인 자들의 비교 분석결과 고분화형 점액성 위선암은 미분화형 점액성 위선암에 비하여 통계적으로 유의하게 발병 당시 연령이 높았고(P=0.006), 혈관 침습 양성예가 경계 유의치 (P=0.058)를 보이며 낮은 빈도를 보였다. 그러나 그 밖의 인 자 즉 성별, 병소의 위치나 크기, 위벽의 침윤정도, 림프절
Table 1. Clinicopathologic profiles of all patients with MGC and NMGC
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
MGC NMGC
P-value (n=34) (n=1036)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Age (yr)
(Mean±SD) 55.8±11.0 55.7±11.8 NS
Sex
Male 20 673 NS
Female 14 363
Location
Lower third 21 537 NS
Midle third 11 372
Upper third 1 94
Whole 1 33
Size
(Mean±SD) 8.0±3.5 5.9±3.3 0.000
Depth of wall invasion
T1 3 353 0.001
T2 6 211
T3 17 395
T4 8 77
Lymph node metastasis
N0 5 442 0.001
N1 8 265
N2 11 157
N3 10 172
Distant metastasis
M0 28 978 0.016
M1 6 58
Stage of disease
I, II 9 570 0.001
III, IV 25 466
Curability
Curative 23 929 0.001
Noncurative 11 107
Lymphatic permeation
Absent 4 385 0.004
Present 30 651
Vascular permeation
Absent 28 886 NS
Present 6 150
CEA (serum level)
≤4.5 ng/L 23 890 0.029
>4.5 ng/L 11 146
CA 19-9 (serum level)
≤37 ng/L 27 933 NS
>37 ng/L 7 103
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ MGC = mucinous gastric carcinoma; NMGC = nonmucinous gastric carcinoma; SD = standard deviation; NS = not significant.
Table 2. Clinicopathologic features of mucinous gastric adenocar- cinoma with different histologic subtypes
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Differentiated Undifferentiated
Variables P-value
type (n=8) type (n=26)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Age (yr)
Mean±SD 63.8±7.3 53.0±10.6 0.006
Gender
Male 3 17 NS
Female 5 9
Location
Lower third 6 15 NS
Middle third 2 9
Upper third 0 1
Whole 0 1
Size (cm)
Mean±SD 6.4±2.6 8.5±3.7 NS
Depth of invasion
Not to serosa 2 7 NS
To or beyond serosa 6 19
Lymph node involvement
Absent 1 4 NS
Present 7 22
Distant metastasis
Absent 7 21 NS
Present 1 5
Stage
I/II 2 7 NS
III/IV 6 19
Lymphatic permeation
Absent 2 2 NS
Present 6 24
Venous permeation
Absent 8 20 0.058
Present 0 6
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ SD = standard deviation; NS = not significant.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
전이상태, 원격전이 여부, 병기 분포, 림프관 침습 등은 유 의한 차이를 보이지 않았다(Table 2).
2) 생존율
(1) 전체 예에서 조직형에 따른 생존율 비교: 조직형에 따 른 1,070예의 생존율 분석 결과 고분화암(53예, 5.0%), 중분 화암(374예, 35.0%), 미분화암(251예, 23.4%), 인환세포암 (358예, 33.4%), 점액성암(34예, 3.2%)의 수술 후 5년 생존율 은 각각 89.7%, 69.9%, 59.3%, 66.1%, 61.3%로 유의한 차이 (P=0.0002)를 보였다(Fig. 2).
반면에 점액성 위선암(34예)과 비점액성 위선암(1,036예)으 로 양분하여 5년 생존율을 비교한 결과 각각 59.9% 및 67.0%
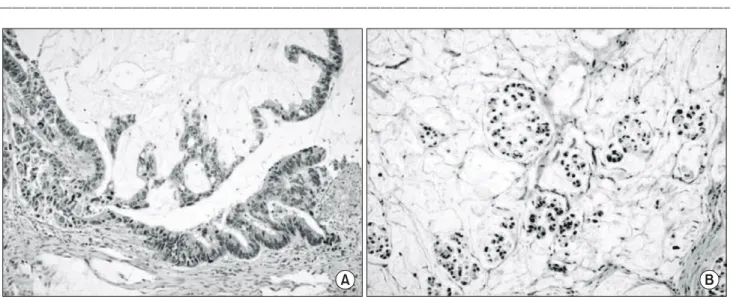
Fig. 1. Mucinous gastric adenocarcinoma of well-differentiated type (A) and poorly differentiated type (B) (H&E, ×100).
A B
Fig. 2. Survival curves for patients with gastric adenocarcinoma according to histologic types. WEL = well differentiated tubular adenocarcinoma; MOD = moderately differentiated tubular adenocarcinoma; SIG = signet ring cell carcinoma;
POR = poorly differentiated adenocarcinoma; MUC = mucinous adenocarcinoma.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
로 그 차이는 통계적인 유의성을 보이지 않았다(Fig. 3).
(2) 점액성 위선암에서 여러 임상병리학적 특성에 따른 비교: 점액성 위선암의 분화도에 따른 5년 생존율 비교에서 고분화형은 미분화형에 비교하여 통계적으로 유의하게 좋 은 생존율을 보였고(Fig. 4), 점액량에 따른 구분 즉 종양면 적의 50% 이상에서 세포외형 점액풀이 보이는 경우를 우성 형(dominant type), 30% 이상인 경우를 부분형(partial type)으 로 구분하여 비교한 결과 양 군 간의 생존율은 유의한 차이 를 보이지 않았다(Table 3).
병기별로 점액성 위선암과 비점액성 위선암의 5년 생존 율을 비교한 결과 제1, 제2, 및 제3 병기에서는 두 군 간에 유의한 차이를 보이지 않았으나 제4 병기에서는 점액성 위 선암 환자의 생존율이 비점액성 위선암 환자보다 유의하게 좋았다(Table 4).
고 찰
위암의 조직학적 분류 가운데 가장 많이 사용되는 것은 World Health Organization, Lauren 및 Ming 분류이다.(7) 그 러나 위암의 많은 경우는 단일한 조직형으로 구성되어 있 기보다는 여러 조직형이 서로 혼재하고 있기 때문에 어느 분류법도 전체적인 조직의 특성을 이상적으로 표시하기엔 부적절하다. 조직형의 분류 시 보다 널리 퍼져 있는 유력한 조직 세포형을 따르는데 임상병리학적 특성이 바로 이런 보다 널리 퍼져 있는 유력한 조직 세포형에 의해서 결정되 지 않을 가능성도 있다고 본다. 점액성 위선암은 WHO 국 제 조직학적 분류의 정의(8)에 따르면 종양의 50% 이상에 이르는 상당량의 세포외성 점액이 보유된 선암이며, 일본 위암학회에서는 종양 실질내 점액풀에 의해 상당량의 점액 호수(mucous lakes)가 특징적인 선암으로 정의(9)하고 있다.
반면에 형 등(10)은 종양 면적의 30% 이상에서 점액이 발견 되는 예의 생물학적 특성이나 예후가 50% 이상에서 점액이 발견되는 예와 비교하여 유사한 양상을 보임을 근거로 종 양 면적의 30% 이상에서 점액이 발견되는 예들을 점액성 위선암으로 정의하였으며 본 연구에서도 이들의 주장과 같 은 범주를 이용하였다. 점액성 위선암은 다른 전형적인 위 선암과 동일하게 생겨나지만 나중에 종양이 진행되는 과정 에서 점액성으로 변하는 것으로 일반적으로 알려져 있 Fig. 3. Survival curves according to histologic types. MUC = mu-
cinous gastric adenocarcinoma; NMUC = non-mucinous gastric adenocarcinoma.
Fig. 4. Survival curves according to histologic subtypes in mucin- ous gastric adenocarcinoma.
Table 3. Five-year survival rate for patients with mucinous gastric cancer
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ No. 5-year survival rate P-value ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Differentiated type 8 100.0% 0.0185
Undifferentiated type 26 45.4%
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Dominant type 23 61.7% NS
Partial type 11 53.0%
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ NS = not significant.
Table 4. Five-year survival rate for patients with MGC and NMGC ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
MGC NMGC
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ P-value No. 5 YSR (%) No. 5 YSR (%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Stage I 5 75.0 428 94.4 NS
Stage II 4 75.0 142 89.8 NS
Stage III 8 37.5 249 54.2 NS
Stage IV 17 54.5 217 23.3 0.0207
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ MGC = mucinous gastric carcinoma; NMGC = nonmucinous gas- tric carcinoma; NS = not significant.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 다.(2) 대장-직장암 환자에 있어 점액성분은 일반적으로 불
량 예후와 관련이 있고,(11,12) 유방암 환자에서는 양호한 예후와 관련이 있는 것으로 알려져 있다.(13,14) 점액성 위 선암은 발생 초기엔 일반적인 위선암의 형태이나 종양이 점차 진행하는 과정에서 점액성으로 변하는 것으로 알려져 있다.(4,15) 점액성 위선암은 오랜 기간에 걸쳐 불량한 예후 를 보이는 위선암의 유형으로 알려져 왔으나(16) Hoerr 등 (17)은 점액을 분비하여도 림프절 전이가 없으면 반드시 예 후가 불량하지는 않다고 보고하였다. Adachi 등(4)은 세포 외성 점액량이 50% 이상인 경우를 점액성 위선암으로 정의 하고 전체 1,255명의 위암환자 가운데 42명의 점액성 위선 암 환자의 특성을 비교 분석한 결과 종양의 크기나 위치, 위벽 침윤정도, 림프절 전이상태, 병기 등이 점액성 위선암 과 그 이외 조직형의 위선암 사이에 의미 있는 차이가 없었 으며 예후는 점액의 양이 아니라 조직형의 유형에 의해 기 본적으로 결정된다 하였다. 즉 점액성 위선암의 예후가 다 른 유형의 위선암과 비교하여 불량하지 않다 하였다. 더욱 이 Brander 등(2)은 점액성 위선암의 예후가 다른 유형의 위 선암과 비교하여 우월하다는 상반된 주장을 하기도 하였 다. Wu 등(3)은 동일한 연령 및 성별 조건하에서의 비교에 서 점액성 위선암은 비점액성 위선암에 비하여 종양의 크 기가 크고 위상부에 위치하며 장막 침윤예가 많고 림프절 전이예가 많고 높은 병기가 많으며 불량한 예후를 보여 점 액성 위선암은 보다 호전적인 성격을 가지며 진행된 병기 에서 발견되는 경우가 많은 특성을 가진다 하였다. Yasuda 등(18)은 17예의 점액성 위선암 환자와 614명의 비점액성 위선암 환자를 대상으로 동일한 조건의 종양크기, 위벽 침 윤정도, 림프절 상태 및 병기에 있는 예들을 대상으로 생존 율을 비교하였는데 5 cm 이상의 크기 예(45 vs. 53%), 장막 침윤 예(29 vs. 36%), 림프절 전이 예(37 vs. 50%), 제3 병기 예(47 vs. 49%)의 5년 생존율이 어느 경우에서도 통계적으 로 유의한 차이를 보이지 않는다 하였다. 또한 다변량 분석 에서 점액성의 조직형은 독립적인 예후 관련인자가 아니었 고 점액성 위선암의 생물학적 호전도는 비점액성 위선암과 크게 다르지 않다 하였다. 점액성 위선암은 종양 세포의 선 형성(glandular formation) 정도에 따라 두 가지의 아유형 즉 분화도가 좋은 것과 그렇지 못한 것으로 구분 할 수 있 다.(4) Brander 등(2)은 분화도가 좋은 점액성 위선암의 경우 림프절에 전이가 있는 예를 포함하여도 수술 후 생존 기간 이 평균 9년으로 혼합형의 21개월이나 인환 세포형의 5개 월에 비하여 의미 있게 좋은 예후를 보인다 하였다. 본 연구 에서는 전체 대상환자 1,070명 중 분화도가 좋은 53명의 5 년 생존율은 89.7%로 나머지 환자 1,017명의 5년 생존율 65.6%보다 통계적으로 유의하게(P=0.0003) 좋았다. 또한 34 예의 점액성 위선암 가운데 8예(24%)가 고분화형이었으며 이들 중 7예(88%)에서 림프절 전이 양성이었으나 평균 생 존기간 72개월, 5년 생존율 100%로 미분화형(림프절 전이
양성 예; 22/26, 85%)의 평균 생존기간 68개월, 5년 생존율 45%에 비하여 통계적으로 의미 있게(P=0.0185) 좋은 예후 를 보였다. 이처럼 좋은 생존율을 보이는 분화도가 좋은 조 직형을 보이는 환자는 전체 234명의 제4 병기 환자 가운데 점액성 위선암 환자에서는 23.5% (4/17명)이고 비점액성 환 자에서는 1.4% (3/217명)로 통계적으로 유의하게(P=0.000) 점액성 위선암에서 많았다. 또한 17예의 제4 병기 점액성 위선암 가운데 고분화형 4예의 평균 생존기간(72.0±29.7개 월)은 전체 1,070예에서의 분석결과와 마찬가지로 미분화 형 13예의 평균 생존기간(29.2±29.0개월)보다 통계적으로 의미 있게(P=0.021) 좋았는데 이런 복합적인 사실들로 인해 제4 병기 점액성 위선암의 5년 생존율(54.5%)이 제4 병기 비점액성 위선암의 5년 생존율(23.3%)보다 통계적으로 의 미 있게(P=0.0207) 좋을 수 있었던 것으로 생각된다. 점액성 위선암은 조기에 발견되는 예가 극히 드물어 Hirota 등(19) 은 전체 조기 위선암의 0.7%였고 형 등(10)은 1.9%를 차지 한다고 하였다. 본 연구에서는 0.8%(3예/356예)를 차지하고 있었다. Adachi 등(4)도 전체 점액성 위선암의 98%가 진행 성 위암으로 71%가 진행성 위암인 비점액성 위선암에 비하 여 높은 빈도를 나타냈고 이러한 사실 때문에 점액성 위선 암이 임상적으로 더욱 악성도가 높다고 여겨지는 것이라 하였다. 또한 이들은 진행된 점액성 위선암의 경우 일반적 인 진행성 위선암과 비교하여 생물학적 특성이 다르지 않 고 더욱이 특이한 임상양상도 나타내지 않는다 하였다. 형 등(10)은 점액성 위선암이 다른 조직형에 비하여 임상적으 로 보다 악성도가 높게 여겨지는 이유는 종양 자체의 생물 학적 성상 그 자체보다는 조기 진단이 안되어 불량한 예후 를 보이기 때문일 것이라 하였고, 조기에 발견이 잘 안 되는 이유에 대한 가정으로 Ma 등(1)은 첫째 점액성 위선암이 발 생할 때는 다른 일반적인 위선암이었다가 후에 진행을 하 는 과정에서 점액성 위선암으로 되는, 즉 dedifferentition process를 생각할 수 있고 둘째, 종양이 위벽을 침윤해 들어 갈 때 내강(intraluminal) 내로의 점액 분비는 줄어들고 벽내 (intramural)에의 점액의 축적이 늘어나는 사실 등을 들었다.
Adachi 등(4)은 분비된 점액의 양에 따라 점액성 위선암의 생존율에 차이를 나타내지는 않았으며 대장 직장암 가운데 점액성의 예후가 나쁘다는 보고(11,12)와는 달리 위암환자 에 있어서는 점액을 분비하는 암이라는 사실 그 자체만으 로는 불량한 예후를 항시 나타내지는 않는다 하였다. 본 연 구에서도 점액의 분비량에 따른 비교에서 우성형과 부분형 사이의 예후의 차이를 발견할 수 없었다. 결론적으로 점액 성 위선암은 독특한 실재로서의 위선암의 유형이 아니고, 두 가지의 조직학적 아유형(고분화형 및 미분화형)에 의한 분류는 그들의 예후 예측에 유용하게 이용할 수 있을 것으 로 보인다.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
REFERENCES
1) Ma J, Boer W, Nayman J. Intestinal mucinous substances in gastric intestinal metaplasia and carcinoma studied by immu- nofluorescence. Cancer 1982;49:1664-7.
2) Brander WL, Heedlam PRG, Morgan AD. Indolent mucoid carcinoma of stomach. J Clin Pathol 1974;27:536-41.
3) Wu CY, Yeh HZ, Shih RTP. A clinicopathologic study of mucinous gastric carcinoma including multivariate analysis.
Cancer 1998;83:1312-6.
4) Adachi Y, Mori M, Kido A. A clinicopathologic study of mucinous gastric carcinoma. Cancer 1992;69:866-71.
5) Woo LS, Kim DY, Kim YJ, Kim SK. Clinicopathologic features of mucinous gastric carcinoma. Dig Surg 2002;19:
286-90.
6) Sobin LH, Wittekind CH. TNM classification of malignant tumors (5th ed). International Union Against Cancer (UICC).
New York, Wiley, 1997.
7) Lewin KJ, Appelman HD. Carcinoma of the stomach. In: Rosai J, Sobin LH. Atlas of tumor pathology: tumors of the esoph- agus and stomach. Washington, DC: Armed Forces Institute of Pathology 1996:285-300.
8) Watanabe H, Jass JR, Sobin LH. Histological typing of esoph- ageal and gastric tumors, 2nd ed. WHO international histolo- gical classification of tumors. Berlin:Springer-Verlag; 1990.
p.1-26.
9) Japanese Research Society for Gastric Cancer. Japanese classi- fication of gastric carcinoma. 1st English ed. Tokyo:Kanehara;
1993.
10) Hyung WJ, Noh SH, Shin DW, Yoo CH, Kim CB, Min JS,
et al. Clinicopathologic characteristics of mucinous gastric adenocarcinoma. Yonsei Medical Journal 1999;40:99-106.
11) Sadahiro S, Ohmura T, Saito T. An assessment of the mucous component in carcinoma of the colon and rectum. Cancer 1989;64:1113-6.
12) Connelly JH, Robey-Cafferty SS, Cleary KR. Mucinous carci- noma of the colon and rectum: an analysis of 62 stage B and C lesions. Arch pathol Lab Med 1991;115:1022-5.
13) Clayton F. Pure mucinous carcinomas of breast: morphologic features and prognostic correlates. Hum Pathol 1986;17:34-8.
14) Rosen PP, Groshen S, Kinne DW. Factors influencing prog- nosis in node-negative breast carcinoma: analysis of 767 T1N0M0/T2N0M0 patients with long-term follow-up. J Clin Oncol 1993;11:2090-100.
15) Caruso RA. The histogenesis of mucinous adenocarcinoma of the stomach from observations in early gastric cancer. Ann Diagn Pathol 1999;3:160-4.
16) Boland CR, Scheiman JM. Tumors of the stomach. In:Yamada T, Alpers DH, Owyang C, Powell DW, Silverstein FE.
Textbook of gastroenterology. 2nd edition. Philadelphia; J.B.
Lippincott, 1995:1494-502.
17) Hoerr SO, Hazard JB, Bailey D. Prognosis in carcinoma of the stomach in relation to the microscopic type. Surg Gynecol Obstet 1966;122:485-94.
18) Yasuda K, Adachi Y, Shiraishi N, Yamaguchi K, Shiromizu A, Kitano S. Pathology and prognosis of mucinous gastric carcinoma. J Surg Oncol 2001;76:272-7.
19) Hirota T, Ming SC, Itabashi M. Pathology of early gastric cancer. In: Nishi M, Ichikawa H, Nakajima T, Maruyama K, Tahara E, editors. Gastric Cancer. Tokyo: Springer-Verlag;
1993. p.66-87.