http://dx.doi.org/10.5763/kjsm.2016.34.1.10 pISSN 1226-3729 eISSN 2288-6028
중년 마라토너의 심혈관 적응과 부작용
인제대학교 상계백병원 재활의학과
김 영 주
Cardiovascular Adaptation and Side Effects in Middle-Aged Marathoners
Young-Joo Kim
Department of Rehabilitation Medicine, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea
Regular exercise brings about various positive effects on cardiovascular, oncological, psychiatric, neurological, and endocrinological systems of human body. According to exercise types with cardiovascular adaptation, endurance exercise is characterized by eccentric hypertrophy; resistance exercise is characterized by concentric hypertrophy;
and the combination of the eccentric hypertrophy and concentric hypertrophy is seen in cycling and rowing. Although the cardiac functions of athletes are not different from those in general population, athletes show higher exercise capacities because of the increased diameter of ventricle. Atrial fibrillation which is the most common in middle-aged marathoners shows 5.3 times higher prevalence compared to that in general population. In addition, higher arterial stiffness is shown in marathoners, and higher resting blood pressure is shown in sub-3 hours-marathoners. Especially the runners with higher resting blood pressure or severe arrhythmia showed superior cardiopulmonary functions and excessive exercise habits when compared to the normal runners. The runners with exercise-induced hypertension are prone to show increased levels of cardiac markers by increasing cardiac muscle burden in exercise, and then be taken with resting hypertension in the future. The major cause of sudden deaths in marathon race of middle-aged marathoners is coronary artery disease (CAD), and the higher prevalence of CAD is shown in middle-aged marathoners being manifested by the exercise stress test or cardiac computed tomography. Therefore, middle-aged marathoners who regularly participate in marathon race are required to undergo annual exercise stress test, and their additional checkups for cardiovascular system should be supervised by specialized medical doctors.
Keywords: Marathon, Cardiac hypertrophy, Arrhythmia, Hypertension, Sudden death
Received: May 2, 2016 Revised: May 20, 2016 Accepted: May 24, 2016
Correspondence: Young-Joo Kim
Department of Rehabilitation Medicine, Sanggye Paik Hospital, Inje University College of Medicine, 1342 Dongil-ro, Nowon-gu, Seoul 01757, Korea
Tel: +82-2-950-1383, Fax: +82-2-938-4109 E-mail: [email protected]
Copyright ©2016 The Korean Society of Sports Medicine
CC
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/
licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
운동에 의한 심혈관 효과와 그 밖의 유익성들
규칙적인 운동은 심혈관 위험요인들을 개선시키고 심혈관
사건의 위험을 줄이며 1,2) , 혈압과 혈중지질을 개선시키고 3) ,
인슐린 저항성 조절과 사망률 감소 및 심혈관 건강에 유익하다 4) .
조깅 같은 유산소 운동이 대중화된 미국의 경우 1970년대
중반부터 다양한 마라톤 경기에 참여하는 사람들이 크게 증가
하였으며, 실제 42.195 km, 하프 마라톤, 90 km 울트라 마라톤
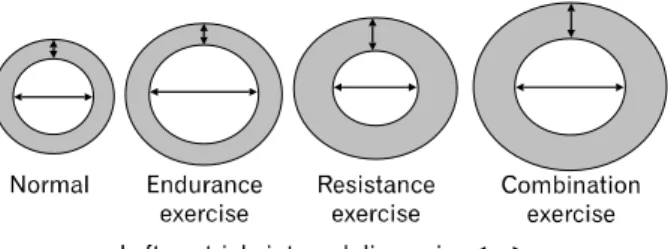
Fig. 1. Left ventricle adaptation according to exercise types.
등의 경기 참여자들에게서 만성 심장질환이 감소되었다 5) . 이러한 효과들 외에 운동은 골다공증 예방 6) 과 치매의 발병을 늦추며 7) , 체력과 자신감 증진 그리고 항우울 효과 8) 와 전립선암 과 유방암의 위험을 낮춘다 9) .
운동유형에 따른 심장의 구조와 기능
운동선수들은 종목에 따라 신체의 체형이 다르듯이 심장의 구조 또한 다른 변형을 가져온다. 운동유형은 크게 지구성 운동, 저항성 운동 그리고 이 둘의 성향이 합쳐진 복합식 운동 으로 나눌 수 있다(Fig. 1). 마라톤 같은 지구성 운동 종목의 선수들은 일반인이나 저항성 종목 선수들에 비해 심근 벽두께 보다 심실의 내경이 유의하게 넓은 특징을 갖는 편심성 비대 (eccentric hypertrophy)를 갖고 있다 10) . 역도 같은 저항성 운동종 목의 선수들은 심실의 내경 보다 심근벽의 두께가 일반인이나 지구성 종목보다 유의하게 두꺼운 동심성 비대(concentric hypertrophy)의 특징을 갖는다 11) . 그리고 지구성과 저항성의 특징을 모두 갖는 사이클이나 조정종목 선수들은 심실의 내경 과 심근벽 두께가 모두 증가되어 있는 특징을 나타낸다 11) . 이러한 현상들은 운동으로 인한 혈압과 심박수의 정도가 심근 형태에 영향을 미치기 때문으로 생각한다 . 지구성 운동은 트레 드밀(treadmill)에서 중-고강도로 달리는 지구성 운동 시 개인 차는 있으나 심박수 상승과 함께 수축기 혈압을 평균 175/69 mm Hg까지 상승시킨다 12) . 저항성 운동은 젊고 건강한 사람의 최대 수축기 혈압을 250–350 mm Hg까지 증가시키며 심박수 는 102–170 범위를 나타낸다 13) . 복합식 운동선수 중에서 특히 조정선수는 심박수가 거의 최대 가까이 증가하며 수축기 혈압 도 200 mm Hg까지 상승한다 14) . 결국 운동선수들의 심근유형 을 결정 짓는 요인은 운동지속시간에 따라 심박수와 혈압 상승을 조절하는 심실에 영향을 미쳐 심실내경과 심실벽 두께 에 변형을 가져와 1회 박출량과 심박출량의 변화를 야기한다 15) .
운동선수의 심근 수축과 이완기능은 일반인 보다 뛰어날 것으로 예상되나 모두 정상범위 안에서 기능을 나타낸다. 수축 기능을 나타내는 ejection fraction은 지구성선수나 저항성선수 모두 정상범위이며 이완기능의 지표인 E (E-velcocity; peak mitral velcocity of early filling)/A (A-velocity; peak atrial velocity of atrial filling), deceleration time, E’ (E’-velocity; early diastolic annulus velocity)/A’ (A’-velocity; late diastolic annulus velocity), E/E’ 지표들에서도 일반인과 차이가 없다 16) . 단, 지구성 선수가 저항성선수보다 E/A가 더 높은 것으로 보고 되었지만 이 역시 정상범위이다 10) . 선수들에게서 심실의 기능이 일반인과 차이 가 없는 대신 지구성 선수들은 심실내경이 크기 때문에 좌심실 용적이 크며 이것은 1회 박출량을 증가시켜 안정 시 심박수를 낮추고 운동 시에는 높은 심박출량으로 최대산소섭취량의 증가와 함께 높은 운동능력 수행에 적응되어 있다 17) .
과도한 운동에 따른 심장사건들과 혈역학 반응
1. 부정맥
심방세동(atrial fibrillation, AF)은 대중에게 보편화된 부정
맥이며 중년의 연령대에서 대략 0.5%의 유병률을 갖고 있고
심부전과 뇌졸증의 위험을 5배까지 증가시킨다 18) . 걷기나 중
등도 달리기 같은 유산소운동은 심장 부정맥의 유병률을 감소
시킨다 19) . 그러나 최근에 만성적인 극심한 운동이 심방세동이
나 심방조동 그리고 심실빈맥 같은 부정맥을 유발시킬 수
있음이 보고되어 왔다 20-22) . AF에 대한 메타분석에서 선수들의
AF는 비선수들 보다 AF의 진행이 상대적으로 5.3배의 위험이
높은 것으로 조사되었다 23) . 지구성 선수들에게서 AF는 가장
높은 빈도를 차지하며 AF의 발생률을 10년간 추적했을 때
통제군(0.9%)보다 지구성 선수들(5.3%)이 더 높고 중년의 연
령에서 더욱 뚜렷하다 24) . 그러나 젊은 운동선수들에게서는
AF의 유병률이 일반대중과 유의한 차이가 없는 것으로 연구
됐다 25) . Baldesberger 등 26) 은 전문사이클 선수였던 중년남성과
비슷한 조건의 골퍼집단을 비교한 결과 사이클선수에게서
낮은 심박수와 높은 유병률의 AF, 심방조동 그리고 심실빈맥
을 발견하였다 . AF는 여성보다도 남성에서 빈도가 4:1 정도로
높으며 첫 번째 증상이 나타나는 연령은 임상적으로 40대와
50대 사이이다 27) . AF의 원인 중 가장 설득력 있는 가설은
고혈압이나 구조적 심질환이 있는 환자에게서 심방의 2차적
만성용적과 압력과부하에 의한 구조적 변화로 인한 심방확장
과 섬유화의 진행으로 설명될 수 있다 28) . Mont 등 29) 은 AF가
Table 1. Exercise times, number of finished races, finishing time, exercise habits, and VO
2maxin ARG
Factor NRG (n=538) ARG (n=14) Total (n=552) p-value
Training history (mo) 83.9±43.8 128.5±73.4* 85.0±45.2 0.041
Marathons completed (n) 42.2±41.5 37.2±21.0 42.1±41.1 0.652
Marathon time (min) 219.7±30.6 206.3±29.2 219.4±30.6 0.106
Exercise intensity (Borg’s RPE scale) 12.9±1.5 14.3±0.9
§13.0±1.5 0.002
Exercise time (min/day) 96.1±37.3 87.9±22.0 95.9±37.0 0.410
Exercise frequency (time/wk) 3.7±1.2 4.0±1.1 3.7±1.3 0.391
VO
2max(mL/kg/min) 49.2±6.5 53.1±6.8* 49.3±6.5 0.030
Values are presented as the mean±standard deviation.
ARG: arrhythmia runners group, NRG: normal runners group, RPE: rating of perceived exertion.
*Significantly different from NRG at p<0.05;
§Significantly different from NRG at p<0.01.
있는 환자들을 통제군과 비교하였을 때 더 큰 심방을 갖고 있었고 심방에 구조적 변화들이 AF의 유발을 일으켰다고 제안하였다 . 이러한 연구들은 일반인과 지구성 운동을 수행하 는 아마추어 중년선수들과 비교한 연구들이 대부분이다. 본 저자는 아마추어 마라톤 선수 552명 중 운동부하검사상 14명 (2.5%)의 심각한 부정맥을 보인 주자들을 정상주자들과 비교 하였는데 심방세동(n=10)과 비지속성 심실빈맥(n=4)이 유발 된 집단에서 최대산소섭취량과 운동경력 그리고 운동강도가 높은 것으로 조사되었다 (Table 1) 30) . 일반적으로 경쟁성 울트 라 마라톤 선수들은 하루에 대략 90–300분 동안 매일 격렬한 유산소 운동에 참여하며 주당 200–300 대사당량시간 (metabolic equivalent×hours)의 일량을 축적하는데 이것은 관상 동맥질환의 예방을 위한 권고된 운동량 보다 5–10배 더 높은 수준이다 31) . 지속적인 운동이 건강에 유익함에도 불구하고 과도한 운동은 치료가 필요한 부정맥 발생의 빈도를 높여 우려를 야기한다.
2. 마라토너의 동맥경직도와 안정 시 고혈압 심혈관계의 위험도를 평가하는데 중요한 항목인 대동맥의 맥파전달속도(pulse wave velocity)는 심혈관계 질환의 표지자 이며 심혈관계 사건 위험의 독립적인 강력한 예측인자이다 32) . 만성적으로 수행해 온 근력운동 선수에게 동맥경직도가 증가 하는 것으로 알려진 반면 지구성 종목의 선수들을 포함한 지구력운동, 여가 운동을 하는 사람들에게서 동맥경직도가 감소한다고 보고되었다 33,34) . 그러나 최근 연구에 의하면 마라 토너의 만성적인 지나친 달리기는 오히려 동맥경직도를 증가 시켜 동맥경화의 진행을 빠르게 할 수 있다고 보고하였다 35) . 이러한 이유는 반복적이고 지나친 동맥의 압박이 대동맥 벽의 탄성요소에 영향을 주어 기계적 피로를 야기하기 때문이라고 하였다 . 즉 운동강도나 높은 혈압이 대상자들의 증가된 대동맥
경직도의 독립인자임을 기술하고 있다. 또 한 가지 극단적인 지구성 운동에서 동맥경직도를 증가시키는 원인은 순환하는 카테콜아민(catecholamine)의 농도 증가에 의해 지속적인 교감 신경의 아드레날린의 혈관수축 상태가 대동맥경직도를 증가 시킬 수 있기 때문이라고 하였다 36) . 고혈압과 운동에 대한 29개 연구를 분석한 결과 운동의 긍정적 효과는 수축기와 이완기 혈압이 정상집단에서 4/4 mm Hg 정도 감소하고 고혈압 집단에서는 11/6 mm Hg 정도 감소하는 것으로 보고되었다 37) . 그러나 운동을 지속해온 마라토너들에게서 안정 시 높은 혈압 이 나타난 집단에서는 운동을 통한 혈압 감소 효과는 더 이상 기대할 수 없는 조건일 것이다. 국내 아마추어 마라토너들 중 3시간 이내로 완주하는 빠른 주자들의 50%가 안정 시 혈압이 140/90 mm Hg 이상으로 나타났다 38) . 이는 국내 고혈압 유병률이 3명 중 1명(32%)이 고혈압 39) 인 것에 비해 높은 비율 이며 완주에 3시간 이상 걸리는 마라토너보다도 역시 유의하 게 높은 비율로 나타났다 38) . 그러나 아직까지 대규모로 극단적 인 운동에 참여하는 아마추어 선수들의 동맥경직도와 혈압과 의 상관관계를 규명하거나 추적 관찰한 연구가 없어 향후 이에 대한 연구가 필요하겠다.
3. 마라토너의 운동유발성 고혈압
규칙적인 신체운동은 심혈관 위험요인들을 개선시키고 심
혈관 사건의 위험을 줄이지만 2) 극심한 운동은 심혈관사건과
관상동맥의 경화반파열의 위험을 증가시켜 급사의 원인이
될 수 있다 40) . 극심한 운동 중 급사를 일으킬만한 수많은 증거들
중 cardiac markers의 상승은 중요한 이슈로 다루어져 왔다 41) .
Cardiac markers 중 임상에서 심근손상의 지표인 cardiac
troponin (cTn)과 심근의 긴장도를 나타내는 n-terminal pro-brain
natriuretic peptide (NT-proBNP)가 비정상적으로 상승한다는
것은 심근경색 42) 이나 심부전 43) 을 의미한다. 이와 같은 cardiac
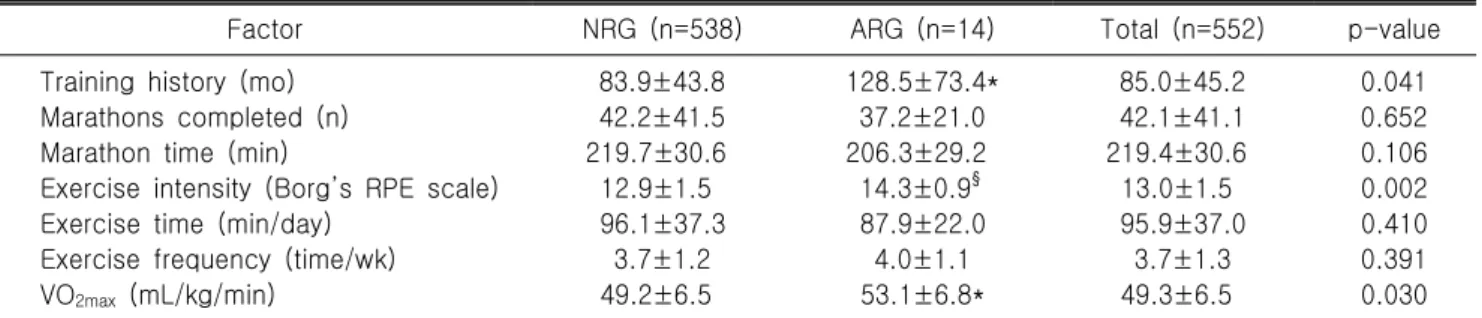
Fig. 2. (A) Changes in cardiac troponin I (cTnI) in ex- ercise-induced hypertension (EIH) and control (CON) groups before and after the marathon. (B) Changes in N-terminal pro B-type natriuretic peptide (NT-proBNP) in EIH and CON before and after the marathon (C) Changes in endothelin-1 in EIH and CON groups before and after the marathon. *Significantly different from CON at p<0.05;
§
Significantly different from baseline (Pre) at p<0.05.
markers는 마라톤, 울트라 마라톤, 철인삼종경기 같은 장기간 운동에서도 기준치 이상 증가된다 44,45) . 이러한 cardiac markers 가 극심한 운동 중 증가되는 것은 아직 까지 명확한 기전이 밝혀지지 않았다. 그러나 현재까지 극심한 운동으로 인해 cardiac markers가 의미 있게 증가하더라도 영구적 손상을 의미 하지는 않는 것으로 나타났다 46,47) . 이러한 반응이 실제로 영구 적 손상을 의미한다면 향후 선수들은 심부전을 격어야만 했을 것이기 때문이다.
운동유발성 고혈압(exercise-induced hypertension, EIH)은 안 정 시는 정상이나 최대 운동시 수축기가 ≥ 210 mm Hg 과도하 게 상승되는 것으로 정의된다 48) . EIH가 있는 사람은 향후 안정 시 고혈압으로 이환될 비율이 5–10배 높으며 49) , 뇌졸증 50) 과 심혈관 사망률의 위험 예측인자이다 51) . 운동 중 과도한 혈압 상승은 혈관의 내피세포기능장애가 중요한 원인으로 알려져 있다 52) . 이러한 반응은 말초혈관 저항을 높여 운동 중 혈압 상승 53) 과 함께 골격근에 혈류장애를 일으킬 수 있을 것이다. 이러한 가설은 EIH를 갖고 있는 장거리 주자들에게 경기 중 심근의 스트레스 증가뿐만 아니라 동맥혈관확장 장애 로 골격근에도 영향을 미칠 것이다 . 본 저자는 EIH가 포함되어
있는 마라톤 경기와 100 km 울트라마라톤 경기 그리고 초울트 라마라톤인 308 km에서의 심장마커와 근손상마커를 조사하 였다. 마라톤 경기 결과는 EIH 주자에게 심근손상마커인 cardiac troponin I (cTnI), 강력한 혈관수축물질인 endothelium-1 그리고 심근의 긴장도를 반영하는 NT-proBNP가 정상혈압주 자 보다 완주 후 높게 증가하여 운동 중 높은 혈압상승이 심근세포막의 투과성을 높여 cTnI의 유출과 심근부담을 상승 시켰던 것으로 보였지만 creatine kinase (CK)와 high sensitive C-reactive protein (hsCRP)은 집단 간 차이를 보이지 않았다(Fig.
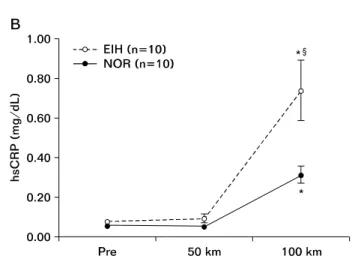
2) 54) . 100 km 울트라마라톤 경기에서는 EIH 주자에서 cTnI가 완주 직후 증가하였지만 집단간 차이가 없었으며 NT-proBNP 와 hsCRP 그리고 CK는 EIH 주자에서 유의하게 높아졌다(Fig.
3) 55) . 이는 EIH 주자가 장거리를 달리는 동안 혈관확장장애로
인한 활동근의 허혈로 근손상이 증가되면서 염증반응을 높였
던 것으로 보여진다. 308 km 초울트라마라톤 대회에서는 EIH
주자와 정상주자간에 심장마커에서 특별한 차이를 발견하지
못하여 두 집단을 통일하여 조사하였다. 이들에게서 특이한
것은 308 km를 달렸을 때 100 km 구간별로 심근손상마커인
cTnI의 증가를 확인할 수 없었으며 단, CK, hsCRP, NT-proBNP
Fig. 3. (A) Creatinine Kinase’s response to the 100 km ul- tramarthon between exercise-induced hypertension group and normal group. (B) C-reactive protein’s response to the 100 km ultramarthon between exercise-induced hy- pertension group and normal group. (C) N-terminal pro- brain natriutretic peptide’s response to the 100 km ultra- marthon between exercise-induced hypertension group and normal group. CK: creatine kinase, EIH: exercise-in- duced hypertension, NOR: normal group, Pre: pre-race, hsCRP: high sensitive C-reactive protein, NT-proBNP:
N-terminal pro B-type natriuretic peptide. *Significantly different from the previous distance at p<0.05;
§Signifi- cantly different from NOR at p<0.05.
의 증가만이 나타났다(Fig. 4) 56) . 이러한 결과들은 마라톤이나 100 km 울트라마라톤 같은 비교적 중등도 이상의 고강도에서 cTnI가 발현되며 54,57) , NT-proBNP의 상승은 운동시간과 관련 있는 것으로 보여진다 55,58) . 이러한 결과를 토대로 살펴보면 EIH를 갖고 있는 주자들은 특히 마라톤이나 100 km 울트라마 라톤 달리기에서 과도한 혈압상승으로 높아진 심근의 부담률 (심박수×수축기혈압)로 인한 부정맥이나 심근의 허혈 유발과 급사의 가능성을 배제하지 못하기 때문에 향후 추가 연구들이 필요할 것으로 보인다.
4. 마라토너의 급사
우리나라의 경우 최근 마라톤인구가 2백만 명 이상으로 급증하였고 매년 120개 이상의 각종 마라톤 대회가 개최되고 있다. 그러나 건강을 위한 국민적 스포츠로 급부상한 마라톤 대회에서 경기 도중 수많은 참가자들이 돌연사하는 사고가 잇따라 발생되면서 심각한 사회문제로 대두되고 있다. 외국의 경우 운동과 관련된 돌연사는 운동선수의 경우 연간 100,000명 당 0.13–0.75명이고, 중년 일반인의 경우 연간 100,000명당 6명 수준으로 보고하였다 59) . 1976–1994년 동안 평균 37세의 미국 마라톤 참가자 총 215,413명 중 4명이 돌연사하여 50,000
명당 1명 꼴로 사망한다 60) . 우리나라의 경우 2000–2008년까지 마라톤과 관련한 돌연사는 총 33건(남성 32명, 여성 1명)이 발생하였지만 외국의 돌연사와 비교 할 수는 없었다 61) . 연령층 은 40대(16건, 48%)와 50대(8건, 24%)가 가장 많은 빈도로 나타났고, 사망한 지점은 절반 이상이 마라톤 완주 직전에 발생한 것으로 볼 때 경기 기록의 단축, 완주에 대한 과욕, 결승점을 향상 전력질주가 돌연사의 간접 원인으로 추정된다 고 하였다 61) . 이들 사망자 중 마라톤 경력자들이 다수 포함되어 있다는 사실이 더욱 충격적이지 않을 수 없다.
운동 중 돌연사의 원인으로 35세 이하에서는 비후성 심근병
증과 선천성 심장기형이며 35세 이상에서는 70% 이상이 허혈
성 심혈관 질환으로 보고되었다 62) . 이와 같이 돌연사 위험은
마라톤 같은 과도한 운동이 중정도 운동에 비해 5–7배 이상
높은 것으로 알려져 있다 5) . 즉 운동 중 심근허혈과 심장부정맥
의 임상적 관찰들은 한차례 격렬한 운동이 심장급사를 촉발하
는 것으로 제안하고 있다 63) . 이러한 발생이 안정 시 보다 운동
시에 대부분 발생하는 이유는 운동 중 심근이 받는 부담이
증가하기 때문이다. 심근부담률(rate-pressure product, RPP)은
심장이 받는 부하량지수로 심박수와 수축기혈압의 곱으로
나타내며 심근산소섭취량(myocardial oxygen uptake)이라고도
Fig. 4. (A) Changes in the creatinine kinase (CK) levels by each check point. (B) Changes in the cardiac troponin I (cTnI) levels by each check point. (C) Changes in the N-terminal pro-brain natriutretic peptide (NT-proBNP) levels by each check point. CK: creatine kinase, Pre:
pre-race, cTnI: cardiac troponin I, NS: no significant, NT-proBNP: N-terminal pro B-type natriuretic peptide.
a
Significant difference compared to the pre-race value;
b
Significant difference compared to the 100 km check point;
cSignificant difference compared to the 200 km check point; *p<0.001; **p<0.05.
한다 64) . 심근부담률이 높을 수록 심장의 일량이 증가되어 심근 에서 요구하는 산소소비량이 증가하는데 이는 잠재된 심혈관 질환자에게는 중요한 의미를 가진다 . 예를 들어 허혈성 심혈관 질환자에게 협심증이 나타나는 역치는 같은 심근부담률에서 흉통이 발생하며 65,66) , 심전도 상에서도 허혈성 ST 분절의 변화 가 발생하는 시기가 상대적으로 일정한 RPP에서 발생한다 67) . 임상에서 사용되는 약물 중 협심증환자에게 심근부담률을 감소시키고 허혈역치를 낮추기 위해 베타차단제 약물이 사용 되는 것은 심장사건을 예방하며 안전한 강도에서 운동하기 위해서이다 68) . 특히 심장급사들의 50%는 사전에 환자들이 관상동맥질환임을 알지 못한 채 발생한다 69) . 이와 같은 우려로 본 저자가 249명의 마라토너들 중 운동부하 검사를 시행한 결과 5명(2%)에서 치료가 필요한 심근허혈이 나타났다 70) . 그 러나 최근 Tsiflikas 등 71) 은 45세 이상의 아마추어 남자 마라토 너 50명(평균연령: 52.7±5.9세)을 대상으로 관상동맥혈관을 촬영한 결과 24명(48%)에서 의미 있는 관상동맥폐색을 발견 하였으며 운동부하 검사상에는 발견되지 않았다고 하였다.
이러한 결과들은 중년의 마라토너들에게는 운동부하 검사에 서 발견되지 않은 잠재된 관상동맥질환이 있을 가능성이 있음 을 시사한다. 따라서 마라톤 참여자 중 40대 이상 중년 마라토
너들에게 보다 적극적이고 주기적인 심혈관 관찰이 요구된다 .
결 론