Invasive Pulmonary Aspergillosis after Influenza A Infection in an Immunocompetent Patient
Oh Kyung Kwon, M.D.
1, Myung Goo Lee, M.D., Ph.D.
2, Hyo Sun Kim, M.D.
1, Min Sun Park, M.D.
1, Kyoung Min Kwak, M.D.
1and So Young Park, M.D.
31
Department of Internal Medicine,
2Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Hallym University Chuncheon Sacred Heart Hospital, Hallym University College of Medicine, Chuncheon,
3Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Hallym University Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea
Invasive aspergillosis has emerged as a major cause of life-threatening infections in immunocompromised patients.
Recently, patients with chronic obstructive pulmonary disease, who have been receiving corticosteroids for a long period, and immunocompetent patients in the intensive care unit have been identified as nontraditional hosts at risk for invasive aspergillosis. Here, we report a case of invasive pulmonary aspergillosis after influenza in an immunocompetent patient.
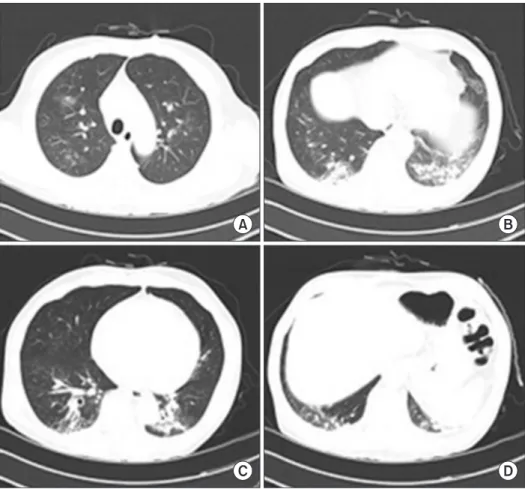
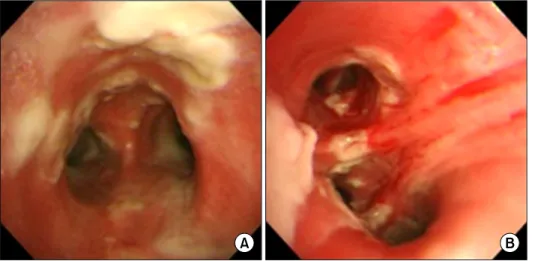
The patient’s symptoms were nonspecific, and the patient was unresponsive to treatments for pulmonary bacterial infection. Bronchoscopy revealed mucosa hyperemia, and wide, raised and cream-colored plaques throughout the trachea and both the main bronchi. Histologic examination revealed aspergillosis. The patient recovered quickly when treated systemically with voriconazole, although the reported mortality rates for aspergillosis are extremely high. This study showed that invasive aspergillosis should be considered in immunocompetent patients who are unresponsive to antibiotic treatments; further, early extensive use of all available diagnostic tools, especially bronchoscopy, is mandatory.
Keywords: Invasive Pulmonary Aspergillosis; Influenza A Virus; Immunocompetence
of morbidity and mortality in immunocompromised patients.
However, during recent years, several reports have described a rising incidence of invasive aspergillosis in critically ill patients admitted to the intensive care unit, even in the absence of an apparent predisposing immunodeficiency. In this situation is related to difficulties in timely diagnosis, caused by insensitive and non-specific clinical signs and lack of unequivocal diag- nostic criteria
1.
After the 2009 A/H1N1 influenza pandemic, it has been shown that invasive aspergillosis is a much more frequent complication in critically ill H1N1 patients and that use of sys- temic steroids contribute to this superinfection
2.
The authors report this case study, along with a literature re- view, which involves invasive pulmonary aspergillosis occur- ring after influenza infection in an immunocompetent patient who did not use systemic steroids.
Copyright © 2013
The Korean Academy of Tuberculosis and Respiratory Diseases.
All rights reserved.
Introduction
Invasive aspergillosis is known to have an important cause
CASE REPORT
http://dx.doi.org/10.4046/trd.2013.75.6.260ISSN: 1738-3536(Print)/2005-6184(Online) • Tuberc Respir Dis 2013;75:260-263
260
Address for correspondence: So Young Park, M.D.
Department of Internal Medicine, Hallym University Kangdong Sacred Heart Hospital, Hallym University College of Medicine, 150 Seongan-ro, Gangdong-gu, Seoul 134-701, Korea
Phone: 82-2-2224-2213, Fax: 82-2-2224-2213 E-mail: [email protected]
Received: Jul. 30, 2013 Revised: Aug. 27, 2013 Accepted: Sep. 10, 2013
cc