Treatment Protocol for Cleft Lip and/or Palate Children in Kyushu University Hospital
14
0
0
전체 글
(2) Akira Suzuki. dren with cleft lip and palate (CL/P). Our team consists of Nurses, Oral surgeons, Anesthesiologists, Speech therapists, Pedodontists, Orthodontists, Prosthodontists, Dental technicians, Oral Hygienists, and the parents’ group. We held a family group “Tsubasa” for the CL/P patients in 1998, and many mothers of older patients supported our efforts. Our family group has two big events: an annual lecture-seminar and a family picnic. At the lecture-seminar, we study about multidisciplinary care for cleft palate children and their families, socio-educational problems from the experience-talk of patients and parents, and also discuss how to care for the growing children and young mothers. At the picnic, we enjoy games, and parents could form friendships and communicate each other. Treatment protocol in the team of the Kyushu University Hospital is thought to be divided into five stages as follows; The first stage is care in peri-natal care until the lip-repair. The second stage is care from lip repair to palatal repair.. consultation for the pregnant mother and her husband. Cleft lip & palate is visualized by a three dimensional ultrasound technique at 20 weeks gestation. An obstetrician tells the mother the findings over 32 week gestation and advises her prenatal consultation with our team; the over 32-weeks-gestation suggests to avoid an abortion. This is important to protect the human rights of a person with disabilities. Our oral surgeon and nurse consult for the couple; explain the epidemiology, pathology, surgical treatment of cleft lip and palate, and future comprehensive treatment after birth. Furthermore, they provide mental support and some information about social support and insurance system. As a result of the prenatal consultation, the mother can have her baby with confidence, her postnatal shock is smaller, and all of the family members can celebrate the delivery of the newborn. Neonatal care means the maternity clinic visit of our staff immediately after the birth. On the. The third stage is care in deciduous and early mixed dentitions. The fourth stage is care for peri-secondary bone grafting in mixed dentition. The fifth stage is management in permanent dentition.. birth of a baby with CL/P our nurse receives a phone call from the maternity clinic and arranges the staff schedules for visiting. An oral surgeon, nurse, and pedodontist will visit the baby in the maternity clinic soon after the birth, even if on the weekend or a national holiday. We make every effort to visit within two hours of. 1. Peri-natal care until the lip-repair. the birth. However, our hospital staffs are very busy, so they usually go to the maternity clinic. In the first stage, the care is divided into. after three PM. At our initial clinic visit, oral. three stages: namely prenatal care, neonatal. surgeon and nurse explain and support the fam-. care, and cheiloplasty. Prenatal care involves. ily members of the CL/P infant as mentioned be-. prenatal consultation after ultrasound diagnosis. fore, and the pedodontist takes an impression of. of the fetus. Since 2003, we started the prenatal. - 70 -.
(3) Treatment Protocol for Cleft Lip and/or Palate Children in Kyushu University Hospital. the maxillary dental arch to make a feeding. of one year, all infants are examined by an oto-. plate like a Hotz’s plate. The next day, the pedo-. laryngologist in our hospital. Children with cleft. dontist and nurse visit again, and provide the. palate are usually susceptible to middle-ear. infant a feeding plate and teach mother and. disease, almost certainly due to abnormalities of. staffs of the maternity clinic the feeding. Eustachian tube function. In Japan, the fre-. technique. Rates of prenatal consultations and. quency of exudative otitis media is over 50 per. neonatal clinic visits on the day of delivery are. cent in patients under 4 years of age [1], but it. increasing. About 40 per cent of our parents un-. decreases with growth [2]. Finally, one-third of. derwent prenatal consultation and 60 per cent. the cleft palate subjects have exudative otitis. of the newborn have undergone a doctor’s visit.. media in all age group.. Pedodontists and nurses guide bottle-feed-. Palatoplasty is carried out at 1.5 years old us-. ing, check the condition of the baby, and adjust. ing modified VY-push back method (modified. the feeding plate every two-weeks until the. Wardill’s procedure). Prior to palatoplasty, we. labioplasty. When the infant has cleft lip, a na-. have a meeting with the family members of CL/P. soalveolar molding (NAM) plate is used as soon. infants and every specialist explains future. as possible in order to get a symmetrical nasal. treatment.. form. This plate is remodeled by putting a nasal stent on the Hotz’s plate. The nasal stent elon-. 3. Care in deciduous and early mixed. gates the columella and corrects the alar. dentitions. cartilage. Cheiloplasty is usually carried out at 3-4 months old. Prior to this operation, the infant undergoes examination by a special pediatrician in our hospital in order to check other congenital disorders. Lip repair is carried out using the modified Cronin’s procedure in unilateral cleft lip cases, and the Manchester’s procedure in bilateral cases.. For CL/P subjects, hearing and speech are the most important social functions. After palatal repair, speech therapists help to train CL/P children to attain complete velopharyngeal function in this third stage. Orthodontists sometimes provide support by expanding the collapsed maxillary dental arch at their request. We hope to complete this training before they enter elementary school.. 2. Care from lip repair to palatal repair. An orthodontist monitors dentofacial growth and takes records every six months from the age. In second stage, after the lip repair, pedo-. of four years. If the patient has severe un-. dontists and oral surgeons check the feeding,. der-growth of maxillary complex, a maxillary. baby food, and dentoalveolar growth, and adjust. protractor is applied. When the patient has se-. the Hotz’s plate until palatoplasty. At the age. vere collapse of maxillary dental arch, maxillary. - 71 -.
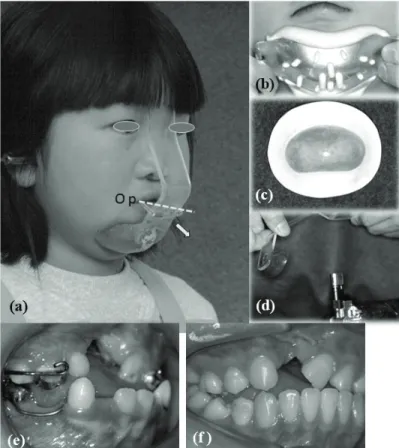
(4) Akira Suzuki. expansion is carried out. In almost all of the. steep mandibular plane angle.. cases, we only monitor dentofacial growth until. In our clinic, a maxillary protraction is occa-. the eruption of the maxillary central incisors.. sionally carried out to correct concave facial. However, even in deciduous dentition, we can see. profile using our designed maxillary protracting. a concave facial profile, which is caused by in-. bow appliance (MPBA, Figure 1) [3, 4, 5]. To. sufficient forward and/or vertical growth of the. evaluate the effects of maxillary protraction [6],. maxillary complex. Maxillofacial characteristics. the maxillofacial change was compared among. on lateral cephalometric films are as follows: a). three groups: the control group “O”, cleft group,. short anterior cranial base (S-N), b) large sad-. and control group “M”. The control group “O”. dle angle (N-S-Ar), c) lack of forward and. consisted of normal children whose maxillofacial. downward growth of the maxillary complex, this. growth was monitored in crossbites without. brings the maxillary complex into an upward and. treatment. The Cleft group consisted of the CL/P. backward position, d) short ramus, e) large. children treated by maxillary protractor. The. mandibular gonial angle, f) backward and down-. control “M” consisted of the normal children. ward rotation of the mandibular body, and g). treated by MPBA. Maxillary protraction was. Figure 1. Maxillary protractor, our designed maxillary protracting bow appliance (MPBA, a): When we make an MPBA, first we take an impression of the mental chin (b) and make a chin pad from acrylic (c). The intra-oral part of the protractor is the soldered four bands on maxillary canines and molars. The acrylic face mask plate is adjusted to the facial profile by heating (d), and the forehead and chin pad anchor the face mask (a). Also, two hooks for elastics are bonded onto the acrylic plate (a). The direction of protracting force is 30 degrees downward from the occlusal plane. The magnitude of protracting force is from 150 to 200 gram unilaterally. The acrylic plate is 30mm in width, 3mm in thickness. Here, from the age of six (e), MPBA was used for 18 months, then canine relationship has been improved (f).. - 72 -.
(5) Treatment Protocol for Cleft Lip and/or Palate Children in Kyushu University Hospital. Figure 2. Sectional rotation arch appliance: (a, b) Central incisor on cleft side erupts with torsion. Sectional rotation arch appliance was applied with a sectional Nickel-Titanium arch wire. (c, d) One month later, the twisted central incisor is corrected without any trouble for vitality of dental pulp and root absorption.. performed at about six years of age. As results,. cisor on the cleft-side were rotated much more. non-cleft children treated by MPBA showed. outwardly and inclined more distally than that. maxillary advancement, while cleft children did. on the non-cleft side. Those torsiversion of. not show maxillary advancement. The subjects. maxillary central incisor on the cleft site must. treated by MPBA showed mandibular clockwise. be corrected as soon as possible. Various types. rotation compared with non-treated subjects,. of orthodontic appliances can be applied to cor-. control “O”. On the subjects with CL/P, it is hard. rect this, but they are not effective. At this. to achieve maxillary advancement using a max-. stage, maxillary permanent teeth are only cen-. illary protractor. However, the recovery of an-. tral incisors and first molars. I designed a new. terior crossbite may be achieved by mandibular. sectional rotation arch appliance, which was a. backward and downward rotation.. modified lingual arch appliance uses a sectional. In deciduous dentition, deciduous maxillary. Nickel-Titanium arch wire (Figure 2) [7]. The. incisors erupted normally, but in early mixed. free-end of this kind of wire shows high. dentition, the permanent maxillary central in-. resilience.. cisor on the alveolar cleft site erupts with some torsion and it will disturb the normal alignment. 4. Care for peri-secondary bone grafting in. of mandibular anterior teeth and sometimes may. mixed dentition. cause a traumatic occlusion and gingival recession. The distribution of torsion of the maxillary central incisors was measured on both cleft and non-cleft sides of study models of 59. In mixed dentition following the correction of torsiversion of maxillary central incisor, the collapsed maxillary buccal segments must be. UCLA and 169 UCLP subjects [7]. The central in-. - 73 -.
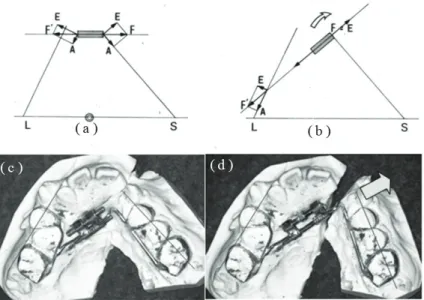
(6) Akira Suzuki. corrected into the normal arch form or slightly. cause collapse of the maxillary arch is not so. over-expanded arch form by maxillary ex-. severe. However in mixed dentition, fan-type. pansion prior to the secondary autogenous bone. expansion is needed, because the anterior part. grafting (SBG). Just before the eruption of the. of small segment shows more collapse, then a. maxillary canine on the alveolar cleft is the best. Quad-helix appliance, W-arch appliance, or. time of performing the SBG. One year before the. another kind of fan-type expander are often. SBG, the collapsed maxillary dental arch is ex-. used. But some problems occur when applying. panded and retained. Deciduous lateral incisor. these conventional expansion appliances. For. on the alveolar cleft is extracted one or two. example, it is very hard to expand the buccal. months before the SBG to make new wide palatal. segments unilaterally, and the large segment is. mucosa.. usually more expanded than the small segment.. We have two types of expansion: namely lat-. Consequently, when the small segment gets. eral expansion and fan-type expansion. Lateral. normal buccolingual relationship, the posterior. expansion is suitable in deciduous dentition us-. teeth are already over-expanded or they have. ing Haas-type expander, Hyrax expander,. occluded in scissors bite. To resolve these prob-. bonded expander, or an expansion plate, be-. lems, I designed a new appliance, a jointed. Figure 3. Jointed fan-type expander: The expanding force (F) is divided into two force elements: namely the expanding element (E) and the anchorage element (A). In a conventional expander (a), the expanding element (E) on the large segment is larger than that on the small segment, consequently the large segment is more expanded than the small one. But, in the Jointed fan-type expander (b), the expansion screw is installed perpendicular to the small segment, most of the expanding force works as an expanding element (E) on the small buccal segment. The pictures (c and d) show the results of using this appliance; before (c) and after expansion (d). Herein, the characters L and S show large and small segments.. - 74 -.
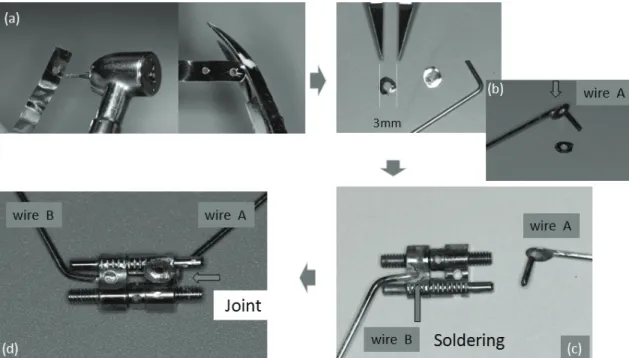
(7) Treatment Protocol for Cleft Lip and/or Palate Children in Kyushu University Hospital. fan-type expander [8, 9] (Prof. Son in the Pusan. large segment is more expanded than the small. National University calls this a differential ex-. one. While in my jointed fan type expander (b. pander).. in Figure 3), most of the expanding force (F). In the Jointed fan-type expander [8], the ex-. works as an expanding element (E) on the small. pansion jackscrew is installed perpendicular to. buccal segment. Thus, we can correct the cross-. the small segment (Figure 3). As a result, the. bite of the small segment.[9] However, the joint. small segment moves mesiobuccally, and a small. of this appliance is loose especially in bilateral. joint is placed in this appliance in order to re-. cleft lip and palate cases, so recently the joint. lease the mesial-directing force. The expanding. was improved to be rigid (Figure 4). (1) Cut two. force (F) on a jackscrew is divided into two force. round washers from metal roll-band material.. elements: namely the expanding element (E) and. (2) Bend a orthodontic wire at right angles (0.9. the anchorage element (A). In a conventional. mm, .036 inch) and solder a washer to the bent. expander, the expanding element (E) on the. wire (to make a sectional wire A) (3) Solder an-. large segment is larger than that (E) on the. other orthodontic wire B at a hole of expansion. small segment (a in Figure 3), consequently the. screw (4) Pass a wire A through another hole of. Figure 4. New version of a Jointed fan-type expander: (a) Cut two round washers from metal roll-band material. (b) Bend an orthodontic wire (0.9 mm, .036 inch) and solder a washer to the bent wire (to make a sectional wire A). (c) Solder another orthodontic wire B at a hole of the expansion screw. (d) Pass wire A through another hole of the screw and solder the second washer to make a joint.. - 75 -.
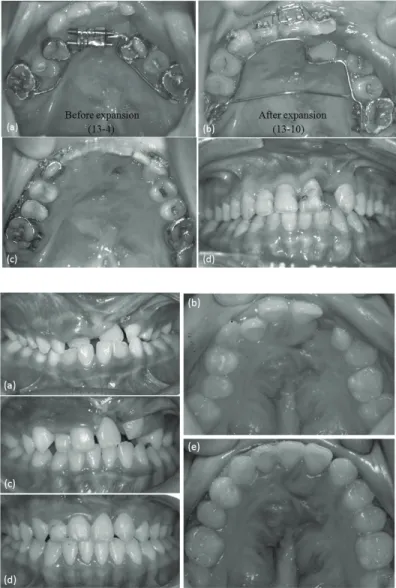
(8) Akira Suzuki. the screw and solder the second washer to make. through the ages from four to ten. We will ex-. a joint.. pand the maxillary dental arch over these values. How should we expand the maxillary dental arch? Based on the study which measured the. taking into account the relapse in retention (Figure 5).. inter-canine widths on both maxillary and. Many aims of bone grafting are reported [11,. mandibular dental arches in normal Japanese. 12, 13, 14], the aims of secondary bone grafting. from three to twenty years of age [10], the aver-. in our protocol [14] are a) stabilizing the ex-. age maxillary inter-canine widths were about. panded maxillary buccal segments and the mo-. 5-6 mm larger than the mandibular ones. bile premaxilla, b) non-prosthetic rehabilitation. Figure 5. Maxillary expansion by Jointed fan-type expander: Almost all the teeth exhibit crossbite, and the small segment shows severe collapse at 13 years old. A Jointed fan-type expander was applied (a), at 6 months later (b), the maxillary dental arch is sufficiently expanded (c). After this, late secondary bone grafting was carried out and maxillary teeth were aligned by a fixed appliance. (d) Eighteen months later, the maxillary dental arch reached to a point almost matching the mandibular dental arch. At the age of 18 years, mandibular sagittal split ramus osteotomy was carried out. Figure 6. (a) At the age of six, maxillary central incisors erupted in crossbite relationship, it was corrected by lingual arch appliance. (b) Before secondary bone grafting at ten years. (c) Four months after the SBG, maxillary left canine is erupting in the transplanted bone. (d, e) All teeth on the maxillary small segment moved forward in the 1.5 years after the SBG, the alveolar defect was closed without any prosthetic operation.. - 76 -.
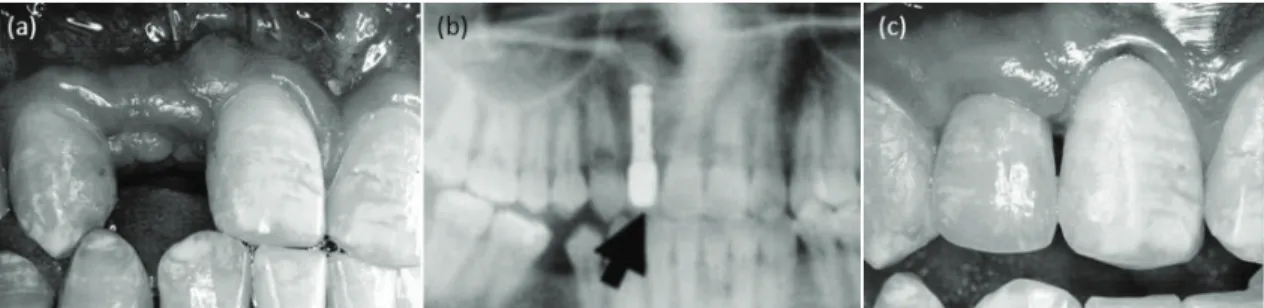
(9) Treatment Protocol for Cleft Lip and/or Palate Children in Kyushu University Hospital. by orthodontic tooth movement into the grafted. prosthetic operation will be done after 18 years. alveolus (Figure 6), c) making the artificial. of age, in this period the gingival tissue is. teeth as small as possible, d) providing bony. stable. Late secondary bone grafting provides. support for the closure of oro-nasal fistulae, e). bony support for subsequent placement of os-. correction of nasal asymmetry due to lack of bo-. seo-integrated dental implants (Figure 7).. ny support for the alar base, and f) providing. Some cases may require mandibular and/or. bony support for subsequent placement of os-. maxillary osteotomy. And others may require. seo-integrated dental implants. The SBG is per-. secondary rhinoplasty, or surgical closure of. formed just before the eruption of the maxillary. oro-nasal fistula. In our team, the performance. canine on the alveolar cleft. Immediately after. of a pharyngeal flap surgery is very rare, how-. the SBG, the erupted canine and posterior teeth. ever in mixed dentition the push back is occa-. on the cleft side will be moved into the trans-. sionally reproduced to lengthen the palate [16].. planted bone using a fixed appliance to prevent. As the cleft palate patients show maxillary un-. the absorption of the transplanted alveolus. It. dergrowth, maxillary osteotomy, maxillary ad-. is very important to provide mechanical stress. vancement is indicative essentially. In our hos-. on the transplanted bone in earlier. The. pital, two-jaw orthognathic surgery is carried. oro-nasal fistula is closed simultaneously dur-. out currently the most common on the subjects. ing the operation.[15]. without cleft lip and palate. However, maxillary advancement or two-jaw surgery are not performed on the CL/P subjects, because they might. 5. Management in permanent dentition. cause poor velopharyngeal closure followed by Final tooth alignment is carried out using the. advancement of the soft palate. In our team, one. fixed appliance after the eruption of maxillary. or two per cent of all the subjects with cleft lip. second molars. Permanent oral habilitation by. and palate have undergone such orthognathic. Figure 7. Secondary bone grafting provides bony support for subsequent placement of the osseo-integrated dental implant. (a) Maxillary right lateral incisor is congenitally missing. Late secondary bone grafting was practiced. (b) Osseo-integrated dental implant was placed in the transplanted bone, and (c) the artificial tooth was made over it.. - 77 -.
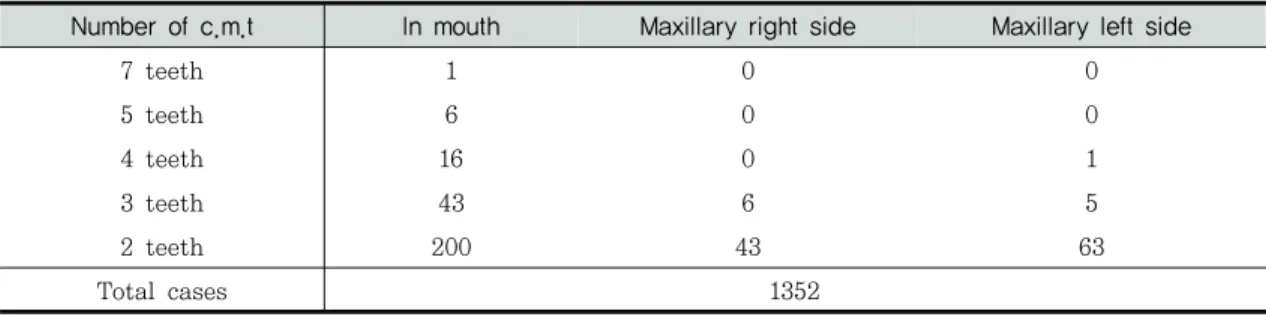
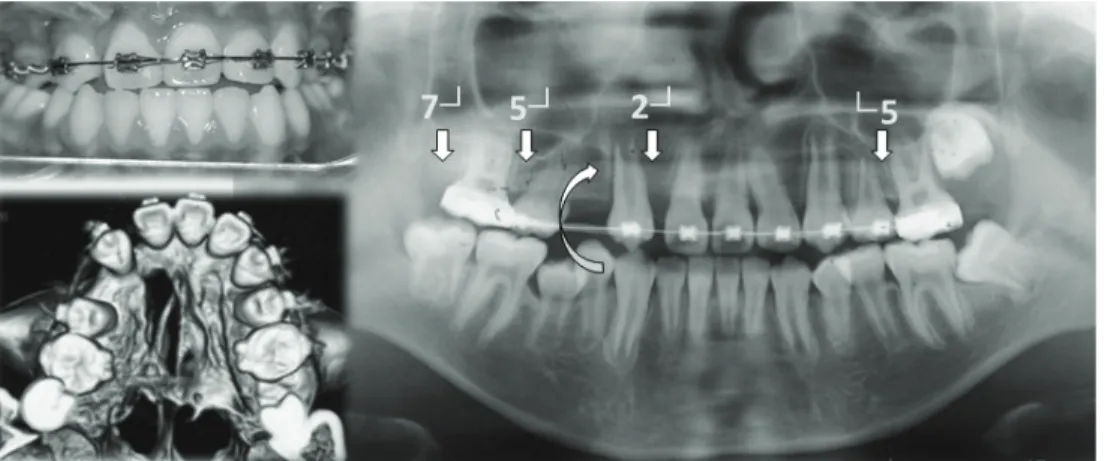
(10) Akira Suzuki. Table 1. Dental abnormality of permanent teeth on the subjects with cleft lip an/or palate (N = 2352) R7. R6. R5. R4. R3. R2. R1. 13. 1. 86. 2. 6. 326. 18. 1.0%. 0.1% 6.4% 0.1% 0.4% 24.1% 1.3%. 1. . 2. . . 262. . 0.1%. . 0.1%. . . 19.4%. . 1338. 1351. 1264. 1350. 1346. 764. 1334. 99.0% 99.9% 93.5% 99.9% 99.6% 56.5% 98.7%. Maxillary Missing Conical Normal. L1. L2. L3. L4. L5. L6. L7. 15. 449. 6. 6. 105. . 8. 1.1% 33.2% 0.4% 0.4% 7.8%. . 0.6%. . . . . . . . . . . 1346. 1346. 1247. 1352. 1344. 1. 345. 0.1% 25.5% 1336. 558. 98.8% 41.3% 99.6% 99.6% 92.2% 100.0% 99.4%. . . . . . . . . . . . . . . . R7. R6. R5. R4. R3. R2. R1. Mandibular. L1. L2. L3. L4. L5. L6. L7. 5. 2. 40. 4. 8. 16. 13. 11. 24. 4. 3. 45. . 3. . 0.2%. 0.4% 0.1% 3.0% 0.3% 0.6% 1.2%. 1.0%. . . . . . . . . . . . . . . 1347. 1350. 1312. 1348. 1343. 1332. 1336. 99.6% 99.9% 97.0% 99.7% 99.3% 98.5% 98.8%. Missing Conical Normal. 0.8% 1.8% 0.3% 0.2% 3.3% 1. . . . . . . 0.1%. . . . . . . 1340. 1328. 1348. 1349. 1307. 1352. 1349. 99.1% 98.2% 99.7% 99.8% 96.7% 100.0% 99.8%. Table 2. Number of congenital missing tooth (c.m.t.) in subjects with cleft lip and/or palate Number of c.m.t. In mouth. Maxillary right side. Maxillary left side. 7 teeth. 1. 0. 0. 5 teeth. 6. 0. 0. 4 teeth. 16. 0. 1. 3 teeth. 43. 6. 5. 2 teeth. 200. 43. 63 1352. Total cases. operations, usually mandibular sagittal split ra-. incisor and second premolar, and sometimes. mus osteotomy (SSRO) or intraoral vertical ra-. second molar. This tendency was similar in. mus osteotomy (IVRO).. mandibular dentition. Four to five per cent of. Finally, the congenital missing of permanent. CL/P subjects showed multiple congenital miss-. teeth is the most frequent problem in many den-. ing teeth in maxillary unilateral dentition (Table. tal difficulties which CL/P subjects have. The. 2 and Figure 8). There are many approaches to. dental abnormality; the frequency of missing. treat and to attain sufficient occlusion in those. teeth, conical teeth, and normal, was surveyed. cases: making prosthetic bridge work, dental. on 1352 CL/P subjects (Table I). The congenital. implants, or dentures. Many CL/P patients show. missing is more frequent in maxillary lateral. anterior crossbite due to undergrowth of the. - 78 -.
(11) Treatment Protocol for Cleft Lip and/or Palate Children in Kyushu University Hospital. Figure 8. A case with multiple congenitally missing teeth: Maxillary dental arch has four missing teeth: right lateral incisor, second premolar, second molar, and left second premolar.. Figure 9. In the case showed in Figure 8, after secondary bone grafting (a, b, c), anterior crossbite must be corrected by extraction of mandibular first premolars and retraction of the mandibular anterior teeth. Then the mandibular first premolar (★) was extracted and transplanted into the place of maxillary right first premolar (d, e, h). Radiographs were taken at the operation (h) and 3 months later following the auto-transplantation (i). At first, the dental pulp did not show a vital response soon after transplantation, but it became to be vital in about four months after the operation (f, g). As this patient is too young to undergo final tooth alignment, maxillofacial growth is monitoring now.. - 79 -.
(12) Akira Suzuki. maxillary. complex.. Orthodontic. treatment. Ⅱ. Acknowledgement. sometimes requires extraction of mandibular first premolars to correct anterior crossbite. To. The author wishes to thank Prof. Baik HS.,. utilize these extracted mandibular premolars,. the president of Korean Cleft Lip and Palate. the autogenous transplantation was performed. Association and Prof. Son WS., the Pusan. without pulpectomy on the tooth in six cases. National University, for their kind invitation. (Figure 9). All of the transplanted teeth had vi-. and supports to the Sixteenth Congress of. tal pulp as the pulp-test shows to be vital over. Korean Cleft Lip and Palate Association.. four months following the transplantation, and it was possible for the transplanted teeth to undergo orthodontic tooth movement. We wish to. References. use the vital tooth that will be extracted to correct anterior crossbite in future in the multiple missing cases. A big problem in orthodontic. 1. Tasaka Y. Middle ear disease and eustachian tube function in patients with cleft. treatment is to decide the timing of trans-. palate. Jibi inkōka rinshō. 1989; 82(8):. plantation, which must be before the closure of. 1155-1167. (In Japanese with English ab-. the root apex, but not too early in maxillofacial growth and development. The autogenous transplantations were carried out at average age of. stract). 2. Yabe R, Abe M, Sawashima M. Otitis media with effusion in patients with cleft palate. 11.5 years.. and congenital velopharyngeal insufficiency.. These are our treatment protocol for the pa-. Nippon Jibiinkoka Gakkai kaiho. 1989; 92:. tients with cleft lip and/or palate in Kyushu. 1012-1020. (In Japanese with English ab-. University Hospital. Our team consisted of dentists and speech therapists actually, but many medical doctors in Kyushu University Hospital. stract). 3. Murakami T, Yokota S, Shimizu K, Takahama Y. A simple maxillary protract-. know of our team activity and support and share. ing bow appliance and its treatment effects. their specialty. For satisfactory care for the. on deciduous reversed occlusion. J Nishi-. subjects with CL/P, more multidisciplinary cooperation and efforts will be needed in the fields of. Medicine,. Dentistry,. Psychology,. and. Nippon Orthod Soc. 1988;33(1):15-23. 4. Kajiyama K, Murakami T, Suzuki A. Evaluation of the modified maxillary pro-. Education.. tractor applied Class III malocclusion with retruded maxilla in early mixed dentition. Am J Orthod Dentofac Orthop, 2000;118(5): 549-559. 5. Kajiyama K, Murakami T, Suzuki A.. - 80 -.
(13) Treatment Protocol for Cleft Lip and/or Palate Children in Kyushu University Hospital. Comparison of orthodontic and orthopedic. Adolescence. Jpn J Pediatric Dentistry.. effects of a modified maxillary protractor. 1997;35(4):670-683. (In Japanese with English. between. abstract). deciduous. and. early. mixed. dentitions. Am J Orthod Dentofac Orthop,. 11. Boyne PJ, Sands NR. Combined orthodontic-surgical management of residual. 2004;126(1):23-32.. palato-alveolar cleft defects. Am J Orthod.. 6. Kawano M, Suzuki A, Han BJ, Sasaguri A.. 1976;70:20-37.. orthodontic treatment of patient with cleft lip and palate (part 3): Maxillary protraction.. 12. Koberg WR. Present view on bone grafting. J Jpn Cleft Palate Assoc. 1995; 20(3):. in cleft palate (a review of literature). J. 135-145. (In Japanese with English ab-. Maxillofac Surg. 1973;1:185-193. 13. Witsenburg B. The reconstruction of ante-. stract) 7. Kawano M, Suzuki A, Han BJ. Orthodontic. rior residual bone defects in patients with. treatment of patient with cleft lip and pal-. cleft lip, alveolus and palate: A review. J. ate (part 2). – treatment of rotated maxil-. Maxillofac Surg. 1985; 13: 197-208.. lary incisor by sectional rotation arch -. J. 14. Suzuki A, Han BJ. Bone grafting on the al-. Jpn Cleft Palate Assoc. 1993;18(1): 107-. veolar cleft in Orthodontic management of. 116. (In Japanese with English abstract). patients with cleft lip and palate. J Korean Cleft Lip Palate Assoc.1998;1(2):7-23.. 8. Suzuki A, Takahama Y. A Jointed fan-type expander: A newly designed expansion ap-. 15. Honda Y, Nakamura N, Goto K, Yoshikawa. pliance for the upper dental arch of patients. H, Suzuki A, Ohishi M. Retrospective eval-. with cleft lip and /or palate. Cleft Palate. uation of oronasal fistula closure. J Jpn. J. 1989;26(3):239-241.. Cleft Palate Assoc. 1997;22(2):41-46. (In Japanese with English abstract).. 9. Suzuki A, Han BJ. Orthodontic treatment of patient with cleft lip and palate by a Jointed. 16. Ninomiya T, Kubota Y, Yahara Y, Suzuki A,. fan-type expander. J Jpn Cleft Palate Assoc. Matsuzaki S, Ogata Y, Shirasuna K.. 1992;17(2):106-113. (In Japanese with English. Evaluation of repushback surgery on velo-. abstract). pharyngeal incompetence in cleft palate. 10. Tsujino K. Machida Y. A Longitudinal Study. patients. J Jpn Cleft Palate Assoc 2008;. on the Growth and Development of the. 33(3):273-279. (In Japanese with English. Dental Arch Width from Childhood to. abstract). 교신 저자. Akira Suzuki Department of Orthodontics, Kyushu University Hospital, Fukuka, Japan Tel : +81-92-6426460 / E-mail : [email protected]. - 81 -.
(14)
(15)
수치

+5
관련 문서
In summary, it was shown that medication and stress during the first trimester of pregnancy were fre- quently associated with cleft lip and cleft palate, adequate timing
This clinical report described the oral rehabilitation of a cleft lip and palate patient with removable partial denture.. Although implant-supported fixed treatment was present- ed
Long-term Orthodontic Treatment and Phonetic Assessment of a Congenital Cleft Lip and Palate Patient
Tindlund RS, et al., Intercanine widening and sagittal effect of maxillary transverse expansion in patients with cleft lip and palate during the deciduous and mixed
Dental anomalies of the permanent lateral incisors and prevalence of hypodontia outside the cleft area in complete unilateral cleft lip and palate.
The third case is the application of transport distraction osteogenesis for closure of the wide cleft alveolus and oroantral fistula in growing bilateral cleft lip and
This study examined the patients with cleft lip and/'or palate who came to the Clinics for Maxillo-Oml Disorders of Tohoku University Dental Hospital for the past 17 years from
However, because of the use of inhalation anesthesia in children and the physiological characteristics of the cleft palate itself combined with the particularities of cleft
Key words : Cleft lip and palate, adult, pentahelix, Tiggle, TG line, Trifocal Circled Pentagon, Malformation,
