Cleft Lip and Palate Surgery in Kyrgyzstan -Two Times of Our Experiences in Central Asia
Joo-Young Park1,2, Byoung-Moo Seo1,2, Pill-Hoon Choung1,2*Department of Oral and Maxillofacial Surgery, School of Dentistry, Seoul National University1, Korean Association of Research and Charity for
Craniofacial Deformity2
ABSTRACT
중앙아시아 키르기즈스탄에서의 구순구개열 봉사활동
박주영
1,2, 서병무
1,2, 정필훈
1,2*서울대학교 치의학대학원 구강악안면외과1, 한국얼굴기형환자후원회2
키르기즈스탄은 옛 실크로드의 한 가운데에 위치한 중앙아시아 국가로서 소련연방이 해체된 뒤 1991년에 독립한 신독립국(Newly Independent States ,NIS)의 일원이다. 대한민국과의 공식적인 수 교가 1992년에 이루어진 이후 18년이 지났지만 키르기즈스탄 거주 한국인의 숫자는 약 900명에 불 과하며 특히 이들 중 대부분은 수도인 비쉬켁(Bishkek)에 살고 있다. 남 키르기즈스탄 제 1의 도시 이자 옛 실크로드의 중심지로 유명했던 오쉬(Osh)시에는 2009년 말 기준 약 50여명의 한국인이 살 고 있다.
한국얼굴기형환자후원회의 후원으로 구순구개열 자선수술팀은 2002년 ~ 2009년까지 11개국, 19회 의 자선수술 활동을 다녀왔으나 중앙아시아 국가로의 방문은 키르기즈스탄이 최초였다. 많은 봉사활 동국에서 지역적, 문화적 그리고 의료환경적인 어려움이 있었지만 2008년 12월, 2009년 7월 두 번 의 키르기즈스탄 오쉬시로의 활동도 예외는 아니었다. 본 논문에서는 최초의 중앙아시아 키르기즈스 탄 구순구개열 자선봉사활동에 대한 자세한 보고를, 준비과정에서부터 활동 완료시점까지 서술하고 자 한다.
Key words : Cleft lip and palate, Volunteering surgery, Kyrgyzstan, Central Asia
I. INTRODUCTION
Kyrgyzstan is known as a Central Asian country located at a crossroads along the Great Silk Road and one of the Former - Soviet Union (FSU) or Newly Independent States (NIS)1). As Kyrgyzstan achieved inde-
pendence in 1991 when the USSR dissolved, diplomatic relation between Kyrgyzstan and South Korea only began in January, 1992.
After 18 years of the relation, the number of Koreans residing in Kyrgyzstan reached ap- proximately 900, most of them live in the capital city, Bishkek, where as only around
Table 1. Constitution of the volunteering surgery team
Dec, 2008 Jul, 2009
OMFS surgeons 3 3
Trainees and fellowship surgeons 2 2
Scrub nurses 1 2
Anesthesiologist 1 1
Administrative officer 0 1
General dentist 0 1
Dental hygienist 0 1
Etc. 0 1
Total 7 12
Figure 1. The map of Kyrgyzstan. Kyrgyzstan is known as a Central Asian country located at a crossroads along the Great Silk Road and borders on Kazakstan, Uzbekistan, Tajikistan and China. Osh is the second largest and 3,000 year-old ancient trading city, whereas Bishkek is the current capital city of the Kyrgyz republic.
50 Koreans live in Osh, the second largest and 3,000 year-old ancient trading city (Figure 1). This small number of Korean res- idents implies us cultural and social distance of this city and nation, although the physical distance from Korea is much closer than any
European and North American countries.
It was the first time for the surgery team of Korean Association of Research and Charity for Craniofacial Deformity to visit a Central Asian country, although the team has visited 11 foreign countries through 19 times from 2002 to 2009. Every visiting country had its own difficulties and facilities in carrying out the surgery missions, and visiting Osh, was not an exception. In this report, our two times of cleft lip and palate charity operation experiences in Osh, Kyrgyzstan, were described in detail, from preparation process before the departure, to the successful completion of visits in December 2008 and July 2009.
II. REPORT AND DISCUSSION
1. Cleft team constitution
The volunteering cleft surgery team con-
Figure 2. The communicating surgeons at the operating room. The oral and maxillofacial surgeons in Osh were eager to learn about the principles and techniques of cleft lip and palate surgery. The Korean OMF surgeon (in the middle front) discussed with the Kyrgyz OMF surgeons (in the most right and left front). The Korean dentist who were residing and practicing in Kyrgyzstan acted as a medical interpreter and his role was essential during the volunteering surgery works (in the middle back).
sisted of 3 operators who were mostly fac- ulty members at the department of oral and maxillofacial surgery (OMFS) of university hospitals, 2 trainees who were usually resi- dents or fellowship surgeons at the depart- ment of OMFS of university hospitals, 1 an- esthesiologist and 1 or 2 scrub nurses (Table 1).
The total number of the team usually did not exceed 10, except for the administrative and etc. personnel.
There were only 7 members at the first visit in 2008, which was the minimal number of the surgical team. Because the medical
information about the surgical and anesthesia equipment and staff had not been available from the local hospital, minimal numbers of the team had to join the activity. From the first visit, scrub nurses and anesthesiologists were turned out to be the most necessary manpower during the surgery, one nurse was added and the anesthesiologist joined again at the second visit (Table 1). Besides, Russian is a second language in Kyrgyzstan instead of English, so a Russian interpreter was essential inside and outside the operat- ing room. As a Russian-English or Russian- Korean interpreter who also had medical and dental backgrounds was rare, some Korean dentists who had resided and practiced in Kyrgyzstan for their missionary work helped the team (Figure 2).
2. Preparation process before departure
There is no direct flight from Seoul, Korea to Osh, Kyrgyzstan at this point in time, April, 2010. The surgery team transferred the flight two times at Almaty, Kasakstan and at Bishkek, Kyrgyzstan and it took ap- proximately 20 hours all the way from Seoul to Osh in total. The flight from Almaty to Bishkek and from Bishkek to Osh was run by small propeller planes, which was un- familiar to the surgery team who usually had travelled abroad by jet air planes.
The surgical instruments and disposable supplies consisted of 10 to 11 packages and cargoing them to the small planes generated cargo overcharging at some airports. Therefore
Primary Diagnosis Dec, 2008 Jul, 2009 Total (%)
UCLP Right 2 4 6 (12)
Left 3 10 13 (26)
UCL Right 2 1 3 (6)
Left 1 0 1 (2)
BCLP 2 2 4 (8)
BCL 0 2 2 (4)
CP 3 0 3 (6)
Facial Scar 5 2 7 (14)
Etc. facial deformity 4 7 11 (22)
Total 22 28 50 (100)
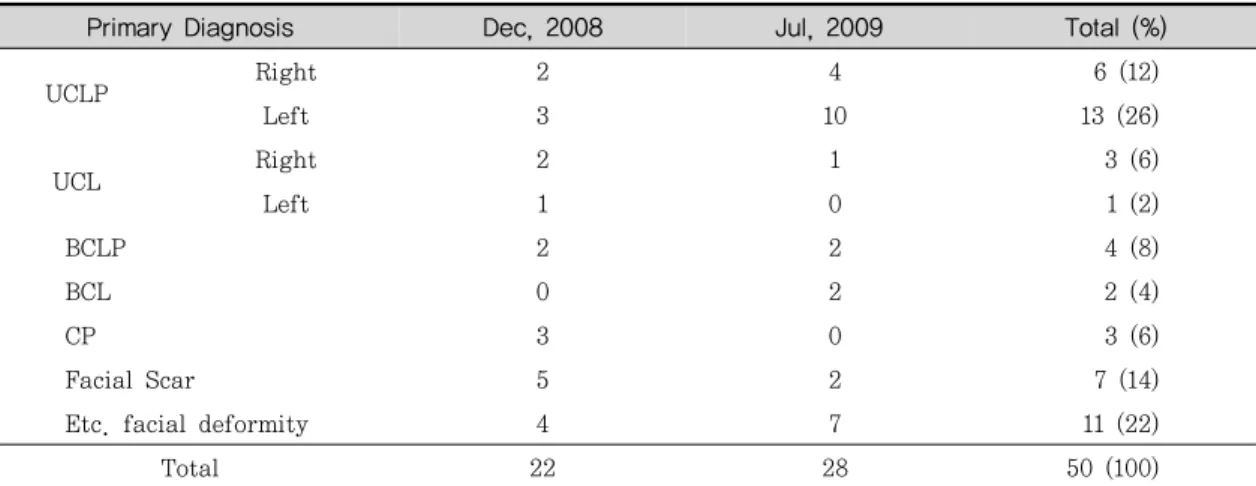
Table 2. Distribution of cleft diagnosis
the surgery team should be aware of the ex- act weight of the cargoes when packaging them in Korea.
The local collaborators were concerned about Kyrgyz custom inspection as it was known for slow processing and unexpected disapproval for foreigners and finally fol- lowed confiscation for some unidentified medical goods. It was essential to communi- cate with the Kyrgyz Ministry of Health about approval of importing the medical goods 1 or 2 months before the departure.
No vaccination or medication for endemic diseases was necessary for travelling in Kyrgyzstan.
3. Patient distribution and characteristics
On the day of preliminary examination, 22 and 28 patients were diagnosed and con- sulted at the first and second visit re- spectively (Table 2). The first diagnosis of the facial deformity was recorded regardless
of the previous surgery performed. For ex- ample, when a 3 year old patient who was born with unilateral complete cleft lip and palate at his left side already had received primary lip closure, his original diagnosis was recorded as UCLP (Left), although his chief complaint was a palate closure. The diagnosis criteria was followed as unilateral or bilateral cleft lip with or without cleft palate and cleft palate alone, since the lip and primary palate have distinct devel- opmental origins from the secondary palate (Table 2)3).
Among every 50 patient consulted prelimi- narily, the percentage of unilateral cleft lip with cleft palate was the highest as 38%
(right or left side), whereas unilateral cleft lip alone was 8%, bilateral cleft lip 4% and cleft palate alone 6% respectively. The per- centage of bilateral cleft lip and palate was slight higher as 8%. Although the birth fre- quency of cleft lip, cleft lip and palate, and cleft palate alone is not known in Central
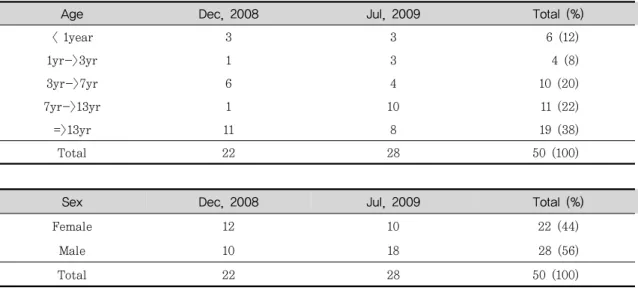
Table 3. Distribution of patients’ age and sex
Age Dec, 2008 Jul, 2009 Total (%)
< 1year 3 3 6 (12)
1yr->3yr 1 3 4 (8)
3yr->7yr 6 4 10 (20)
7yr->13yr 1 10 11 (22)
=>13yr 11 8 19 (38)
Total 22 28 50 (100)
Sex Dec, 2008 Jul, 2009 Total (%)
Female 12 10 22 (44)
Male 10 18 28 (56)
Total 22 28 50 (100)
Asian countries, international data from 57 registries for 1993 – 98 suggested prevalence at birth of cleft lip with or without cleft palate of 3.4 – 22.9 per 10,000 births, and of isolated cleft palate of 1.3 ~ 25.3 per 10,000 births.5 However, no consistent time trends or seasonal patterns in prevalence at birth of either defect have been recorded6-8). In our cases, it was also difficult to find some trends of the disease incidence in such a small number of the patients.
As for the age distribution of the pre- screened patients, the patients over 13 years numbered 19 (38%), whereas the patients un- der 3 years reached only 10 (20%) (Table 3).
The distribution of the patients where young adult and adult outnumbered infants might be caused by several factors, and one of the most influential reasons was poor accessi- bility in summer and winter season. At the first visit it was December and one of the
coldest and snowiest months in Osh, which makes patients not be able to travel to see the doctor. On the other hand, in July when the team visited for the second time, it was one of the hottest and the busiest months for the Osh farmers. Therefore, the parents of the cleft patients could not bring their infants in such hard seasons, the local doc- tors said.
Although it was known that the sex ratio varies with severity of the cleft and across various ethnic groups4), there was no sexual inclination found among the prescreened fe- male and male patients. However, these re- sults originated from the outnumbered adult patients who had various facial deformities other than cleft lip and palate (Table 3). The facialde formities the patients complained were hemangioma on the lip, burn scar un- der the neck, ruling out lymphangioma, de- viated nose, osteomyelitis and screw ex-
A B
Figure 3. The surgery team in the extreme weather condition in Osh. A : Snow piled up all over the hospital at the first visit in December, 2008. Young adult and adult patients could come to see the doctor in the cold weather but infant patients might be hard to get through the snow. B : As temperature was high as 37°C and above, the surgery team was suffered from the extremely hot weather especially inside the operating room. The air-conditioner did not work well and it was almost 40°C during the operation.
Figure 4. Limited surgical illumination and anesthesia equipment in the local operating room. The high request for the palatorrhaphy might attribute to lower performance of the palate surgery in the local hospital. Better surgical light was required for appropriate illumination of the deep palate area, as well as modernized anesthetic equipment and airway maintenance was necessary. There was no effective pediatric anesthetic ventilator and the repeatedly repaired circuit was shown in the picture.
posure, facial pigmentation, ruling out fi- brous dysplasia covering the half of lower face, mild anterior openbite after orthodontic treatment and so on ( Figure 6). The dis- tribution of these facial deformity and path- ology patients proved us that the Inter-re- gional united clinical hospital of Osh ( IUCHO) was the one and only oral and
maxillofacial clinic in the south Kyrgyzstan and there were abundant patients who need- ed good oral and maxillofacial surgeons.
4. Surgery records
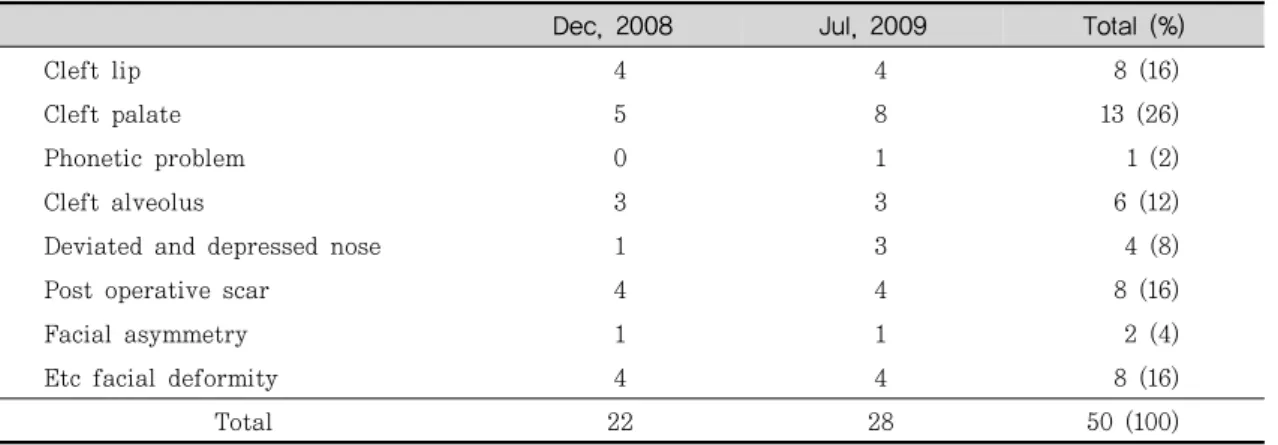
The patients’chief complaints were re- corded at preliminary examination and listed (Table 4). The request for cleft palate clo-
Name of surgery performed Dec, 2008 Jul, 2009 Total (%)
Primary cheiloplasty 4 4 8 (24.2)
Palatorrhaphy 3 6 9 (27.3)
Pharyngoplasty 1 1 2 (6.1)
Alveolorrhaphy 2 3 5 (15.2)
Rhinoplasty 1 0 1 (3.0)
Scar revision 4 3 7 (21.2)
Etc. facial plastic surgery 1 0 1 (3.0)
Total 16 17 33 (100)
Table 4. Distribution of patients’ chief complaint
Dec, 2008 Jul, 2009 Total (%)
Cleft lip 4 4 8 (16)
Cleft palate 5 8 13 (26)
Phonetic problem 0 1 1 (2)
Cleft alveolus 3 3 6 (12)
Deviated and depressed nose 1 3 4 (8)
Post operative scar 4 4 8 (16)
Facial asymmetry 1 1 2 (4)
Etc facial deformity 4 4 8 (16)
Total 22 28 50 (100)
Table 5. Performance of surgery
sure was relatively high as 26%, whereas the chief complaint for cleft lip closure marked as 16%. Lack of appropriate illumination at the operating room and anesthetic problem might attribute to lower performance of the palatorrahphy at the local hospital, which caused the high demand for palatorrhaphy from the patients (Figure 4).
Cleft alveolus and oronasal fistula seemed unfamiliar to the local OMF surgeons, the pa- tients and their parents were neither well aware of the disease state. The surgery de- mand for alveolorrhaphy was also high and
some local plastic and OMS surgeons said that they observed the iliac bone graft for the first time ( Table 5). As for the general surgical equipments such as operation room, bed, illu- mination light and surgical instruments, they seemed never been changed from the Soviet Union era. One of the most necessary equip- ments was a handy autoclave machine, so it was donated to the local hospital after the first visit. At the second visit, the vital sign monitoring kit was donated (Figure 5).
HIV infected patients were one of the dif- ficulties to the surgery team in some African
Figure 5. The general surgical and anesthesia equipments seemed never been changed from the Soviet Union era in the Inter-regional united clinical hospital of Osh (IUCHO). One of the most necessary equipments, the vital sign monitoring kit was donated.
Figure 6. Primary lip closure and palatorrhaphy performed. 33 patients were operated in total among 50 prescreened patients, 8 primary lip closure and 9 palatorrhaphy were performed.
countries, but Kyrgyzstan was not included in such countries. The adult prevalence rate of HIV infection was relatively low, and the official statistics said the rate was less than 0.1% in 2007 and ranked as the world 120th
2). Comparing to the rate of Korea as 0.1%
in the same year and world 151st, Kyrgyzstan
is not a HIV-dangerous country so far.
In total 33 patients were operated among 50 prescreened patients, 8 primary lip clo- sure and 9 palatorrhaphy were performed (Figure 6, Table 5).
Figure 7. Various oral and maxillofacial deformities and pathology in preliminary examination.
Many adult patients with various facial deformities came in preliminary examination. The deformities were hemangioma on the lip, burn scar under the neck, ruling out lymphangioma, osteomyelitis and screw exposure, hemifacial microsomia, and so on.
5. Regional distinctive features
The city of Osh is located just under the high Tien Shan Mountains and the most consist of valleys and basins (Figure 1). The general climate is dry continental, because this nation does not have seaside. Therefore, the city of Osh has 4 distinct seasons, aver- age temperature varies -3 to -5℃ in winter and 25 to 27℃ in summer. The highest tem- perature in July and August often recorded up to 40℃, whereas heavy snow and polar weather often paralyze the city in December and January. These extreme seasons made the surgery team not to be easily adapted (Figure 3A and 3B).
The official name of the Osh municipal hospital was Inter-regional united clinical hospital of Osh ( IUCHO) and it has the one
and only maxillofacial clinic for the Kyrgyz people who reside in the south side of the Tien Shan Mountains. The more organized and modernized clinics exist in Bishkek, but patients have to make a long journey to see the doctors in Bishkek. As there are lack of convenient transportation and asphalt pave- ment, it usually takes 2-3 days to reach Bishkek by car. Therefore, the IUCHO should consider almost every south Kyrgyz people as its patients. It was reported that the pop- ulation of inhabitants in Kyrgyzstan reached 5,431,747 in 2009, so the absolute number of patients who can come to the IUCHO should not be many2). However, as the department of OMFS in IUCHO was the one and only clinic to take care of facial deformity pa- tients in south Kyrgyzstan, charity operation
in IUCHO has such a valuable and sig- nificant meaning.
As for the religion of Kyrgyzstan, the of- ficial statistics said 75% Kyrgyz people were Muslims, 20% were Russian orthodox and 5%
were any others2). The city of Osh was re- ported as a more Muslim inclinated city, but Christian missionaries from various countries were trying to nest in Osh in the recent years. Because Osh has been an important trading city from the ancient times, prop- agation of religion could be started from this city. In opposition to the foreign religious action, the Kyrgyz government announced the new law regarding the national religion in January, 2009 and any foreign travelers related to the foreign religious action have to be precautious.
III. CONCLUSION
It was the first time for our surgery team to visit a Central Asian country and some unique difficulties existed on visiting Osh, Kyrgyzstan. Although only 7 to 12 surgery team members joined the volunteering cleft surgery camp, 33 patients were operated among 50 prescreened patients, 8 primary lip closures and 9 palatorrhaphy were performed in two times of visit. Reflecting the hospital situation in Osh, scrub nurses and anes- thesiologists were turned out to be the most necessary manpower during the surgery, as well as a Russian-English or Russian-Korean
interpreter who also had medical and dental backgrounds was essential. It was not an easy journey from Seoul to Osh, which took approximately 20 hours with two transfers, but the surgery team was pleased to see the Kyrgyz patients smile after the operation.
The Inter-regional united clinical hospital in Osh has the one and only clinic dealing with OMFS patients in south Kyrgyzstan, charity operations in IUCHO were meaningful expe- riences to the surgery team. With better an- esthetic environment and traveling condition, volunteering cleft surgery in Osh could be valuable for all of the Korean surgery team, local patients and local medical staff.
IV. REFERENCES
1. Managing Conflict in the Former Soviet Union: Russian and American Perspectives, Cambridge, The MIT Press 1997:30-31.
2. Central Intelligence Agency, T he world factbook- Kyrgyzstan 2009.
3. Mossey PA, Little J, Munger RG, Dixon MJ, Shaw WC. Cleft lip and palate. Lancet 2009;374:1773-1785.
4. Mossey PA, Little J. Epidemiology of oral clefts: an international perspective. Cleft lip and palate: from origins to treatment.
New York: Oxford University Press 2002;
127–58.
5. Mossey P, Castillia E. Global registry and database on craniofacial anomalies. Geneva:
World Health Organization 2003.
6. International Clearinghouse for Birth
교신 저자 정필훈
서울대학교 치의학대학원 구강악안면외과 서울특별시 종로구 연건동 28 서울대학교 치의학대학원 110-749/
Tel : 02-740-8717 / Fax : 02-740-8717 / E-mail : [email protected] Defects Monitoring Systems. Annual report
2001 (with data for 1999). Rome: ICBDMS 2001.
7. Castilla EE, Orioli IM, Lugarinho R.
Monthly and seasonal variations in the
frequency of congenital anomalies. Int J Epidemiol 1990;19:399–404.
8. Fraser FC, Gwyn A. Seasonal variation in birth date of children with cleft lip.
Teratology 1998;57:93–95.