I. 서론
치주질환은 치태세균에 의한 염증발생으로 치은, 치주인대, 백악질 및 치조골등으로 구성되는 치주조 직을 파괴시켜 결국에는 치아를 상실시킬 수도 있다.
치석제거술 및 치근면 활택술과 같은 기계적 치료 방법과 효과적인 구강위생교육은 세균성 치태의 제 거 및 치주병인균의 비율을 감소시킬 수 있다. 그러 나 이런 기계적 치료방법은 5mm이상의 깊은 치주낭 에서는 접근도 불량과 해부학적 복잡성때문에 그 효 과가 감소하며, 치주병인균이 상아세관내를 세균서 식처로 삼아 재집락함으로써 치주질환을 재발시킬 수도 있다1-3). 또한 치석제거술 및 치근면 활택술은 치은연하세균의 조성변화에 영향을 주지만 이런 변 화는 일시적이며 몇 주 후면 처음과 같은 상황으로 되 돌아 가는 경향이 있다. 따라서 치주질환의 치료 및 예방을 위해서는 치태내 세균의 제거가 필수적이다.
최근에는 치주질환의 시작과 진행에 세균의 역할 이 강조되면서 치료분야에서 항생제와 항균제의 사 용에 대한 관심이 점차 증가하고 있다4-6). 많은 연구 에서 광범위 항생제를 전신적으로 투여하였을 때 치 주질환의 치료에 효과적이었음이 보고되었다7). 그 러나 전신적으로 약물을 투여하는 경우에는 전체 구 강내 병소를 동시에 치료할 수 있다는 장점이 있는 반면에 병소부위에서 지속적인 약물농도유지를 위
하여 과량의 약물이 장기간 투여되어야 하는 단점이 있다8). 이로 인한 약물의 축적 및 부작용, 내성균 발 생 및 장내 유익한 세균들에 미치는 영향등 여러가 지 문제점들이 제기되어 왔다9-13).
전신적인 항생제 투여의 단점을 극복하기 위해서 치주낭내에 직접 항생제를 투여하는 국소약물송달 법(local drug delivery system)에 대한 연구가 1970 년대 후반부터 활발히 진행되어 왔다14-17). 치주감염 부위에 대한 국소약물송달법의 효과는 치주낭내에 직접 항생제를 투여하여 충분한 기간동안 약제가 유 지될 수 있게 하는 능력에 달려있다고 할 수 있다. 국 소약물송달법으로 사용되는 약제로는 tetracycline, minocycline, metronidazole, chlorhexidine등이 있으 며, fibers18-21), gel8, 22-27), ointments28), films29-30)과 같 은 형태로 항생제를 치주낭내에 전달하는 시도가 연 구되어 왔다.
minocycline은 반합성 tetracycline인 광범위 항생 제로 치주질환의 원인균주에 대한 감수성이 높고 이 약에 대한 내성균 발현율이 낮다는 장점이 있으며 조직친화성이 크고 특히 치면의 칼슘에 흡착되는 작 용이 있어 지속적인 항균작용을 나타낼 수 있다31). 게다가 치주조직내에서 교원질용해작용을 억제하는 능력이 있으며 지방용해성이 크고 혈장반감기가 길 며 뇨배출이 적고 치은열구내에는 혈장보다 5배나 높은 농도를 보이면서 치주병인균에 대해 항균효과 대한치주과학회지 : Vol. 28, No. 4, 1998
치근면 활택술후
2% minocycline gel의 치료효과
권영혁·박지원·허 익·박준봉 경희대학교 치과대학 치주과학교실
를 보이는 것으로 알려져 있다32-33). 따라서 minocy- cline은 방출조절시스템을 이용한 국소약물송달법으 로 가장 적절한 항생제 중 하나이다. 세균감수성에 대하여서는
Bacteroides species, Fusobacterium nucleatum, Actinobacillus actinomycetemcomitans 와 Capnocytophaga species
를 포함한 치주병인균에 대한 항균효과와 지속성이 tetracycline보다 더 좋기 때문에 국소약물송달제제로 선택하게 되었다29, 34).국소약물송달법으로 사용되는 fibers, gel, oint- ments, films과 같은 형태중에서 최근에는 사용하기 쉽게 제공되는 syringeable gel에 관심이 집중되고 있
으며35-37), van Steenberghe등(1993)22)과 Graca등
(1997)27)은 2% minocycline gel을 사용한 연구에서 치석제거술 및 치근면 활택술후 사용된 minocycline gel이 치주낭깊이를 더 많이 감소시켰고, 치은염증을 감소시키는 데 부가적으로 긍정적 효과가 있음을 보 여주었다.
본 연구에서는 중등도 및 진행된 치주염환자의 치 료를 위하여 치석제거술 및 치근면활택술후 2%
minocycline gel을 부가적으로 사용한 군과 치석제 거술 및 치근면활택술 후 생리식염수로 치은연하 세 척술을 시행한 군과의 비교를 통하여, minocycline gel의 부가적 사용이 치주질환치료에 미치는 미생물 학적, 임상적 효과를 비교 분석 평가하는데 그 목적 이 있다.
II. 연구대상 및 방법 1. 연구대상
중등도 이상의 성인형 치주염 환자 27명(남, 12명 여, 15명)을 대상으로 하였으며, 이들의 나이는 평균 42.7세(35-59세)였다. 또한 5mm이상 8mm이하의 치 주낭깊이를 가지고 방사선 소견상 명백한 치조골 소 실을 보이는 치아가 상하악 및 좌우에 적어도 2개이 상 존재하는 환자를 선택 하였다.
환자의 전신적 상태는 최근 6개월 이내에 전신적 인 항생제를 복용한 경험이 있는 환자와 tetracycline 계 항생제에 과민증이 있는 환자는 대상에서 제외하
였으며, phenytoin, nifedipine, cyclosporin등 치은에 영향을 미칠 수 있는 약제를 투여받는 환자와 심한 치아우식증 및 타액선 장애가 있거나 1년이내에 포 괄적인 치주치료를 받은 환자도 제외하였다. 구강내 소견에서 국소의치의 지대치로 사용되거나 2급이상 의 동요도를 보이거나 예후가 불량하리라 예견되는 치아도 대상에서 제외하였고, 1년안에 치석제거술이 나 치근면 활택술과 같은 초기 치주치료이외의 외과 적 치주처치를 받지 않은 환자를 대상으로 하였다.
2. 연구방법
실험군은 치석제거술 및 치근면활택술 시행후 0, 1, 2, 3주차에 1회씩 각각 58곳의 치주낭내에 2%
minocycline gel(미노클린 치과용 연고, 동국제약, 한 국)을 주입하였고, 대조군에서는 동일술식을 시행후 0, 1, 2, 3주차에 생리식염수(n=40)로 치은연하 세척 술을 실시하였다.
환자에게 초진시부터 적절한 치태조절방법을 위 한 구강위생교육을 실시한 후, 초진시부터 0주차까 지 치석제거술 및 치근면활택술만을 시행하였다. 처 음 4주간은 매주 환자를 내원시켜 치주낭깊이 측정 을 제외한 각종 임상검사를 실시하였고, 그 이후는 4, 8, 12주차에 내원시켜 모든 임상검사 및 미생물학 적 검사를 각각 시행하였다.
가) 임상검사
임상검사는 초진시 William's probe(직경 0.5mm) 를 사용하여 치주낭깊이를 측정하고, 치태지수, 치은 지수, 치은열구출혈지수 및 치은퇴축량을 측정하였 다.
이번 실험에 이용한 임상검사방법을 구체적으로 살펴보면 다음과 같다.
(1) 치태지수(Plaque Index, Pl I - Silness and Lo..
e(1964)38))
0 : 치태가 부착되어 있지 않은 상태
1 : 치은변연에 치태가 엷게 부착되어 있어서 탐 침소자로 치면을 긁어 보아야 확인 할 수 있는 상태
2 : 치은변연을 따라 육안으로 확인가능하며 과량 의 치태가 부착되어 있으나, 치간 사이에는 치 태가 없는 상태
3 : 치은변연에 많은 양의 치태가 침착되어 있고 치간사이에도 치태로 채워져 있는 상태
(2) 치 은 지 수 (Gingival Index, GI-Lo..
e and Silness(1963)39))
0 : 정상 치은
1 : 경한 염증, 경미한 색조 변화, 가벼운 부종, 치 주탐침에 의한 출혈성향이 없는 경우
2 : 중증 염증, 발적, 부종, 치은의 색조 변화, 치주 탐침에 의한 출혈이 있는 경우
3 : 심한 염증, 상당한 발적과 부종, 궤양이 있으며 계속적인 출혈이 있는 경우
(3) 치은열구출혈지수(Sulcular Bleeding Index, SBI - Mu..
hlemann and Son(1971)40)) 0 : 치은이 건강하고 치은 출혈이 없는 경우 1 : 치은 출혈이 있으나 치은 변색과 부종이 없는
경우
2 : 치은 출혈과 변색이 있으나 부종이 없는 경우 3 : 치은 출혈, 변색 및 부종을 수반한 경우 4 : 치은 출혈, 변색, 부종 및 궤양을 수반한 경우 5 : 치은 출혈이 저절로 되고, 변색이 있으며 현저
한 부종 및 궤양이 있는 경우
(4) 치주낭깊이(Pocket Depth) : 치주낭 깊이는 William's 14W probe(직경 0.5 mm)를사용하여 치은변연으로부터 치주낭의 최심부까지를 치 아당 6점법으로 측정하여 평균값을 구하였다.
(5) 치은퇴축(Gingival Recession) : William's 14W probe를 사용하여 백악법랑경계와 치은변연 까지의 거리를 치아당 6점법으로 측정하여 평 균값을 구하였다.
나) 미생물학적 검사
미생물학적 검사는 초진, 0, 4, 8, 12주에 시행하였
으며, 검사방법은 선택된 치아의 치은연상치태 및 부 착물을 제거하고, 멸균된 큐렛으로 치은연하치태를 채취하여 glass slide에 놓고 생리식염수를 떨어뜨려 분산시킨 후 cover glass를 덮고 위상차현미경을 이 용하여 400배 배율로 관찰하였다41). 세균의 형태적 구분은 구균, 비운동성 간균(직선형 간균), 방추상균, 사상균, 나선균 및 운동성 간균의 6 가지로 구분하였 다. 각 slide 마다 최소 3군데 이상의 부위를 선정하 여 각 부위의 세균수를 측정하여 그 백분율을 구하 였으며, 모든 조작은 1 시간이내에서 완료하였다.
다) 통계학적 분석
2-way ANOVA Test를 통하여 군내 및 군간 분석을 시행하였으며, 실험군과 대조군사이의 유의성 검사 는 student's t-test를 이용하였다.
III. 연구성적
중등도 및 진행된 성인형 치주염이 있는 환자들을 대상으로 하여 1/4악당 적어도 2개이상의 치아가 5
∼8mm의 치주낭깊이를 보이는 환자 27명을 대상으 로 하였다. 치석제거술 및 치근면 활택술을 시행한 후, 실험군으로 58곳의 치주낭에 2% minocycline gel 을 1주 간격으로 4회 주입하였고, 대조군으로 생리식 염수를 치주낭에 적용하고 12주간 임상검사 및 세균 검사를 시행하여 다음과 같은 성적을 얻었다.
1. 임상검사
(1) 치태지수(Pl I)
실험군과 대조군 모두 초진에 비하여 8주까지 치 태지수가 현저히 감소하였으며 이러한 양상은 12주 까지 유지되었으며, 초진과 비교하여 각 기간간에는 실험군과 대조군 공히 유의성있는 차이를 보여 주었 다(p<0.05). 그러나 8주이후 12주까지에는 양군 공 히 치태지수가 다소 증가하였다. 각 기간별 실험군 과 대조군 간 치태지수의 비교에서 대조군에 비하여 실험군에서 다소 낮은 경향을 보였다(Table 1).
(2) 치은지수(GI)
기간에 따른 평균치은지수의 변화는 실험군과 대 조군 모두에서 초진에 비하여 12주까지 점차 감소하 는 경향을 보였으며, 초진과 비교하여 실험군과 대조 군 모두에서 유의성있는 차이가 나타났다(p<0.05).
각 기간별 양군간의 치은지수의 비교는 대조군보다 실험군에서 각각 낮게 나타났다(Table 2).
(3) 치은열구출혈지수(SBI)
기간별 치은열구출혈지수의 변화는 실험군과 대 조군 모두에서 초진에 비하여 12주까지 유의하게 감 소하였으며(p<0.05), 특히 실험군에서는 초진시 3.04±0.32의 치은열구출혈지수가 매주 감소하여 약 제 투여후인 4주째에 0.28±0.10으로 가장 낮게 나
타났으며(p< 0.05), 이 후 12주까지 지속적으로 유지 되었다. 이에 반해 대조군에서는 초진시 2.96±0.24 의 평균지수가 1주째에 0.97±0.17로 감소하여 (p<0.05), 12주째까지 거의 평행을 유지하였다. 각 기간별 양군의 치은열구출혈지수를 비교하면, 실험 1주째에 이미 실험군(0.66±0.20)이 대조군(0.97±
0.17)에 비하여 통계학적으로 유의하게 낮게 나타났 으며(p<0.05), 이 후 12주째까지 각각 실험군에서 유 의하게 낮게 나타났다(p<0.05),(Table 3).
(4) 치주낭 깊이(Pocket Depth)
기간에 따른 평균 치주낭깊이의 변화를 살펴보면, 실험군에서는 초진시 5.55mm에서 8주에 4.13mm로
week Initial 0 1 2 3 4 8 12
group exam.
saline 2.40±0.28 1.30±0.32† 0.89±0.23† 0.78±0.17† 0.75±0.18† 0.75±0.18† 0.73±0.18†0.74±0.12† minocycline 2.48±0.27 1.25±0.24† 0.71±0.19† 0.63±0.21† 0.63±0.18† 0.56±0.18† 0.48±0.10†0.53±0.09†
week Initial 0 1 2 3 4 8 12
group exam.
saline 2.44±0.28 1.20±0.28† 0.89±0.16† 0.81±0.15† 0.79±0.18† 0.74±0.17† 0.67±0.16† 0.66±0.16† minocycline 2.50±0.18 1.51±0.53† 0.72±0.18† 0.61±0.18† 0.66±0.17† 0.59±0.18† 0.54±0.13† 0.48±0.11†
week Initial 0 1 2 3 4 8 12
group exam.
saline 2.96±0.24 1.41±0.26† 0.97±0.17† 0.89±0.19† 0.89±0.15† 0.89±0.16† 0.93±0.13† 0.96±0.13† minocycline 3.04±0.32 1.39±0.30† 0.66±0.20†* 0.44±0.18†*0.33±0.18†* 0.28±0.10†*0.29±0.14†* 0.34±0.08†*
Table 1. Plaque index (mean ± S.D.)
† : Statistically significant difference at each group from the initial examination.(p<0.05, two-way analysis of variance) No statistically significant difference between two groups. (p<0.05, student's t-test)
† : Statistically significant difference at each group from the initial examination. (p<0.05, two-way analysis of variance) No statistically significant difference between two groups. (p<0.05, student's t-test)
Table 2. Gingival index(mean±S.D.)
Table 3. Sulcular bleeding index(mean±S.D.)
† : Statistically significant difference at each group from the initial examination.(p<0.05, two-way analysis of variance)
* : Statistically significant difference between two groups. (p<0.05, by student's t-test)
1.42mm감소하였으며 12주에서는 1.38mm 감소하 였다. 대조군에서는 초진시 5.17mm에서 4주에 4.05mm로 약 1.12mm 감소하였으나 8주에는 1.10mm, 12주에는 0.96mm로 다소 증가하였다. 초 진과 비교시 각 기간간에는 실험군과 대조군 모두에 서 통계학적으로 유의성있는 차이를 보였으며 (p<0.05), 실험군에서 대조군에 비하여 치주낭깊이 가 더욱 많이 감소하였다(Table 4).
(5) 치은퇴축(Gingival Recession)
초진시에 대조군에서는 0.84mm, 실험군에서는 0.67mm의 치은퇴축양이 치석제거술 및 치근면 활 택술후에 1.53mm, 1.43mm로 각각 유의성있는 증가 를 보였으며(p<0.05), 이러한 증가양상은 실험12주 까지 양군 모두 지속되었다(Table 5).
2. 미생물검사
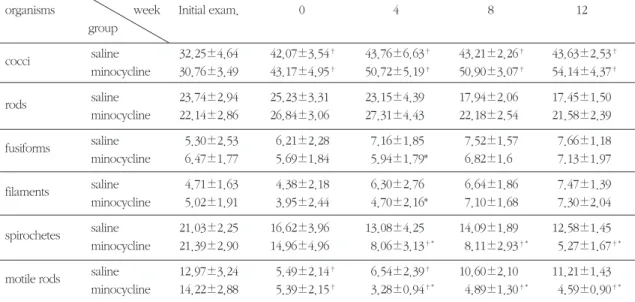
실험기간별 각 세균군의 변화를 관찰하면, 구균, 방추상균 및 사상균은 실험군과 대조군 공히 0, 4, 8, 12주로 이행됨에따라 점차 증가하는 경향을 보였고, 특히 구균에서는 실험군 12주에서 전체의 54.14%를
차지하였으며, 양군간에는 유의한 차이가 없었다.
비운동성 간균은 초진에서부터 12주째까지 거의 평 행을 유지하였다. 반면, 나선균 분포의 기간별 변화 양상은 구균과는 반대로 기간이 경과함에따라 상대 적으로 감소하는 경향을 보였으며, 특히 실험군에서 는 2% minocycline gel 사용후 4주째부터 현저히 감 소하여(8.06%) 12주째는 5.27%로 더욱 낮아졌으며 대조군에 비하여 통계학적으로 유의한 차이를 나타 내었다(p<0.05). 운동성 간균의 기간에따른 변화를 살펴보면, 대조군에서는 12주에서 초진의 분포비율 과 동일한 수준으로 회복되는 양상을 보였으나, 2%
minocycline gel 투여군에서는 초진시(14.22%)에 비 해서 0주(5.39%)부터 현저히 감소하여 12주(4.59%) 까지 지속되었으며, 두군간의 유의성은 실험 4주째 이후부터 인정되었다(p<0.05)(Table 6, Fig. 1).
IV. 총괄 및 고찰
치주질환의 예방과 치료는 세균의 집락화와 성장 을 억제하는 방법에 기초하고 있으며 치은연상치태 의 제거는 구강관리능력에 따라 염증을 예방하기에 충분하지만 모든 형태의 치주염을 효과적으로 치료
week Initial 0 4 8 12
group exam.
saline 5.17±0.42 4.11±0.42† 4.05±0.39† 4.07±0.38† 4.21±0.37†
minocycline 5.55±0.74 4.44±0.64† 4.27±0.60† 4.13±0.57† 4.17±0.54†
Table 4. Pocket depth (mean±S.D., mm)
† : Statistically significant difference at each group from the initial examination. (p<0.05, two-way analysis of variance) No statistically significant difference between two groups. (p<0.05, student's t-test)
week Initial 0 1 2 3 4 8 12
group exam.
saline 0.84±0.60 1.53±0.63† 1.53±0.63† 1.53±0.63† 1.55±0.61† 1.60±0.57† 1.59±0.60† 1.59±0.60† minocycline 0.67±0.61 1.43±0.59† 1.46±0.60† 1.45±0.61† 1.48±0.58† 1.50±0.58† 1.53±0.56† 1.53±0.56†
Table 5. Gingival recession(mean±S.D., mm)
† : Statistically significant difference at each group from the initial examination. (p<0.05, two-way analysis of variance) No statistically significant difference between two groups. (p<0.05, student's t-test)
하기 위해서는 치은연하치태의 조절이 필수적이다.
많은 연구들로부터 치주질환과 연관된 세균의 분류 가 이루어졌다. Listgarten과 Hellden(1978)41)은 질환 의 심도가 깊은 성인형 치주염에서 나선균과 운동성 간균의 비율이 높게 나타난다고 보고하였으며,
Tanner등(1979)42)은
Porphyromonas gingivalis
가 빠 르게 진행되는 성인형 치주염과 연관된다고 하였다.Armitage등(1982)43)은 건강한 사람과 치주질환이 있 는 사람에서 치은연하 치태세균의 분포를 비교하며 건강한 사람에서는 구균이 우세하고 치주질환이 있
organisms week Initial exam. 0 4 8 12
group
cocci saline 32.25±4.64 42.07±3.54† 43.76±6.63† 43.21±2.26† 43.63±2.53†
minocycline 30.76±3.49 43.17±4.95† 50.72±5.19† 50.90±3.07† 54.14±4.37†
rods saline 23.74±2.94 25.23±3.31 23.15±4.39 17.94±2.06 17.45±1.50
minocycline 22.14±2.86 26.84±3.06 27.31±4.43 22.18±2.54 21.58±2.39
fusiforms saline 5.30±2.53 6.21±2.28 7.16±1.85 7.52±1.57 7.66±1.18
minocycline 6.47±1.77 5.69±1.84 5.94±1.79* 6.82±1.6 7.13±1.97
filaments saline 4.71±1.63 4.38±2.18 6.30±2.76 6.64±1.86 7.47±1.39
minocycline 5.02±1.91 3.95±2.44 4.70±2.16* 7.10±1.68 7.30±2.04
spirochetes saline 21.03±2.25 16.62±3.96 13.08±4.25 14.09±1.89 12.58±1.45
minocycline 21.39±2.90 14.96±4.96 8.06±3.13†* 8.11±2.93†* 5.27±1.67†*
motile rods saline 12.97±3.24 5.49±2.14† 6.54±2.39† 10.60±2.10 11.21±1.43 minocycline 14.22±2.88 5.39±2.15† 3.28±0.94†* 4.89±1.30†* 4.59±0.90†*
Table 6. Percent of distribution of subgingival bacteria(mean % ±S.D)
† : Statistically significant difference at each group from the initial examination. (p<0.05, two-way analysis of variance)
* : Statistically significant difference between two groups. (p<0.05, by student's t-test)
Fig. 1. Schematic illustration of % variation of cocci, rods, fusiforms, filaments,spirochetes and motile rods between each group at the time interval.
는 사람에서는 운동성세균이 우세함을 보고하였고, Slots 등(1982)44)은
Actinobacillus actinomycetem- comitans
가 국소유년형 치주염의 주요 원인균이라 하였다. 치은연하치태세균의 분포는 특이 치주병인 균의 발현율과 임상지수와의 관계에 영향을 미치게 되며 치주질환의 치료는 이러한 세균의 제거가 주 목적이 되었다.치은연하 치태세균의 조절은 환자 스스로 하는 방 법 및 전문적인 기계적 치태조절법과 약물효과에 의 해 치태내 세균의 수를 감소시키는 화학적 치태조절 법으로 대분해 볼 수 있다. 환자 스스로 하는 구강위 생관리는 일반적인 치주치료의 중요한 부분을 차지 하지만 깊은 치주낭에서의 치은연하치태세균에는 큰 효과를 미치지 못한다45). Lavancy등(1987)46)은 전 문적인 구강위생 교육과정을 배웠다 하더라도 치은 연하치태세균에는 영향을 주지 못하며 기계적 치주 치료후에 치주낭에 잔존하는 세균은 치은연하치태 세균의 재형성 및 재집락에 중요한 역할을 한다고 하였다. 전문적인 기계적 치태조절법인 치석제거술 및 치근면 활택술은 염증발생인자를 제거하는 측면 에서 볼 때 가장 기본적인 치료법이며 치주조직의 건강을 회복시킬 수 있으나 치주낭이 깊을수록 기구 도달의 어려움이나 해부학적 복잡성의 문제때문에 그 효율성이 감소한다28). 따라서 이러한 한계점을 극 복하기위하여 치석제거술 및 치근면 활택술에 다양 한 항생제 및 항균제를 전신적 또는 국소적 용법으 로 부가하여 사용하게 되었다.
전신적인 항생제 투여는 치주낭의 기저부까지 약 제도달을 가능케하며 전체 구강내 병소들을 동시에 치료할 수 있어서 비용절감과 다양한 약제사용이 가 능하다는 장점이 있는 반면에 병소부위에서 지속적 인 약물농도를 유지하기 위하여 과량의 약물을 장기 간 투여하여야 하는 단점이 있다. 이에 반해 국소약 물 송달법을 이용한 항생제 투여는 직접 치주낭내에 약제를 적용함으로써 치주낭내에서 고농도의 약제 농도를 얻을 수 있으며 최소한의 부작용과 내성균주 의 발달 가능성을 감소시킨다. 또한 지각과민증을 유발시킬 수 있는 백악질제거를 하지 않아 시간소모 가 적다는 장점을 가진다47). 전신적 투여시 얻을 수
있는 약제농도는 정균작용의 효과만을 나타내는 반 면 국소약물 송달법으로 제공된 고농도의 약제농도 는 살균작용의 효과를 제공하게 된다25).
본 연구에서 사용한 2% minocycline gel을 치은연 하부위로 주입할 경우 약 72시간 후에도 대부분의 치주병인균을 제거할 수 있는 3.4㎍/㎖의 농도를 유 지하며 이런 농도가 약 1주일 정도 지속적으로 치주 낭내에서 방출된다48). 대부분의 치은연하세균은 1∼
2㎍/㎖ 이하의 최소억제농도(minimum inhibitory concentration)에서도 효과적으로 억제되기 때문에 이 연구에 사용된 국소약물 송달제제는 치주병인균 에 아주 효과적이라고 할 수 있다.
이번 연구에서는 초진시 구균과 비운동성 간균의 비율이 각각 전체세균의 30∼32% 와 22∼23%를 차 지하였고, 치석제거술 및 치근면 활택술후에는 각각 42∼43% 와 25∼26%로 증가한 반면에 나선균과 운 동성 간균의 비율은 초진시에는 21% 와 12∼14%이 었던 것이 치석제거술과 치근면 활택술 후에는 14∼
16%와 5%정도로 감소하였다. 2% minocycline gel을 국소적용한 후인 4주 때에는 구균과 비운동성 간균 의 비율이 각각 50%와 27%로 약간 더 증가하였고 나 선균과 운동성 간균의 비율은 8% 와 3%로 초진시와 비교하여 유의성있게 감소하였으며, 나선균의 비율 은 12주때까지 지속적으로 감소하는 경향을 보여 주 었으나 운동성 간균의 경우는 4주 때보다 약간 증가 하는 경향을 보였으나 초진시와 비교시에는 운동성 간균의 비율이 유의성있게 감소하였다. 생리식염수 로 치은연하 세척술을 시행한 경우에는 치석제거술 및 치근면 활택술 후에 감소된 나선균의 비율이 12 주 때까지 유지되었으나 운동성 간균의 경우에는 12 주 때에는 초진시와 비슷한 수준으로 반전되려는 경 향을 보였다. 이는 치은연하 세척술의 효과라기보다 는 기계적 치주치료방법과 효과적인 구강위생교육 에 의해서 일시적으로 개선된 치은연하 환경이 부여 되었으며, 이런 결과가 5mm이상의 깊은 치주낭에서 는 제한적일 수 밖에 없다는 것을 보여주었다. 이런 결과를 미루어 볼 때 본 연구에서 사용한 2%
minocycline gel은 기계적 치주치료후에 남을 수 있 는 치주병인균을 제거하는데 효과적이라고 한
Hagiwara등(1998)49)과 정 등(1998)50)의 결과와 유사 한 효과를 보였다.
임상지수측면에서는 치석제거술 및 치근면 활택 술 후에 실험군과 대조군에서 모두 큰 차이를 보이 지 않았으나 2% minocycline gel을 사용하기 시작한 1주 때부터 12주 때까지 지속적으로 치은열구출혈지 수가 유의성있게 감소하였으며, 치주낭 깊이의 변화 는 2% minocylcine gel 사용군에서 생리식염수로 치 은연하 세척술을 시행한 군에 비해 큰 차이의 감소 량을 보여주었으나 통계학적 유의성은 보이지 않았 다. 이런 임상지수의 변화는 일반적으로 처음 3개월 동안에 주로 나타났으며 이전의 다른 연구들에서도 3개월간 개선된 임상지수가 유지되었다고 보고하였
다8, 23). van Steenberghe등(1993)22)과 Graca등
(1997)27)은 기계적 치주치료에 대한 보조제로서 2%
minocycline gel을 반복적으로 치은연하부위로 투여 한 경우 탐침시 출혈지수와 치주낭깊이의 향상을 가 져왔으며 이는 초진시 치주낭깊이가 7mm이상되는 부위에서 가장 큰 효과가 있다고 하였다.
국소약물 송달법을 이용한 약제투여는 주변 연조 직의 염증소견에 부가적인 영향을 미치며 이런 효과 는 치은연하 세균에 영향을 주는 직접적인 효과와 더불어 간접적인 항염증효과를 제공하게 됨으로써 치석제거술 및 치근면 활택술 후에 얻을 수 있는 효 과에 부가적으로 임상적, 미생물학적 효과를 부여하 였다. 지금까지 단일치료로써 국소약물송달법을 이 용한 많은 연구들에서도 치석제거술 및 치근면 활택 술만 한 경우와 비교하였을 때 치주낭 깊이의 감소 및 임상부착수준의 증가를 보였다고 보고하였으나22,
27), 병든 치근면에 대한 처지없이 주변 연조직의 조 건을 향상시키기 위한 국소약물 송달법의 단일치료 보다는 기계적 치주치료방법에 보조적으로 사용하 는 것이 더 효과적일 것이다.
이번 연구결과를 비추어 볼 때 치석제거술 및 치근 면 활택술만을 단독으로 시행하는 것보다 2%
minocylcine gel을 병행하여 사용하는 것이 임상적, 미생물학적으로 더 효과적이었다. 그러나 향상된 임 상상태 및 치은연하환경을 유지하는데 필요한 minocylcine의 최소억제농도(1㎍/㎖)가 언제까지 유
지될 수 있는지에 대해서는 알 수 없었다. 앞으로 특 이치주병인균을 억제하는데 필요한 국소약물송달제 제의 약제농도를 규명하며, 생흡수성 합성체로 제공 될 경우 정확한 투여량의 결정 및 전신적으로 흡수 되는 약제량, 그리고 국소약물송달법의 장기간 효과 에 대한 더 많은 연구가 필요하리라 사료된다.
V. 결론
성인형 치주염 환자 27명을 대상으로 초기치료후 2% minocycline gel의 부가적 사용의 치료효과에 대 한 평가를 위하여 이 연구를 시행하였다. 검사항목 으로 치태지수, 치은지수, 치은열구출혈지수, 치주낭 깊이, 치은퇴축양의 5개의 임상지수와 치은연하치태 에대한 미생물검사를 시행하였다. 치석제거술과 치 근면활택술후에 실험군으로 2% minocycline gel을, 대조군으로 생리식염수를 해당 치주낭내에 0, 1, 2, 3 주째에 주입하였다. 치태지수, 치은지수, 치은열구출 혈지수 및 치은퇴축양은 초진, 0, 1, 2, 3, 4, 8, 12주에, 치주낭깊이 및 미생물검사는 초진, 0, 4, 8 12 주에서 각각 검사하여 그 변화를 분석검토하여 다음과 같은 결론을 얻었다.
1. 각종 임상지수의 변화를 관찰하면, 2% minocy- cline gel을 국소약물송달제제로 사용한 실험군 에서는 생리식염수로 치은연하세척술을 시행한 대조군에 비하여 치은열구출혈지수의 유의한 감소를 보였으며(p<0.05), 치주낭깊이 또한 대 조군에 비하여 더 많이 감소하였다.
2. 세균분포의 변화는 2% minocylcine gel 사용군 과 생리식염수로 치은연하세척술을 시행한 두 군 모두에서 구균과 비운동성 세균의 분포비율 은 시간경과에 따라 점차 증가하 는 경향을 보 였으나, 양 군간에 유의한 차이는 없었다.
3. 나선균의 비율은 대조군에서 시간 경과에 따라 서 서 히 감 소 하 였 으 나 , 실 험 군 에 서 는 2%
minocycline gel 주입후 4주째부터 현저히 감소 하여 12주에서는 더욱 낮아졌다(p<0.05).
4. 운동성 간균의 변화는 대조군에서는 초진에 비
하여 실험 시작시에 급속히 감소하였으나 이 후 서 서히 증가하여 12주째에서는 초진시와 동일한 비율 을 차지하였다. 반면에 2% minocylcine gel을 주입한 실험군에서는 초진에 비하여 실험시작시에 현저히 감소 하여 이 비율이 12주째까지 유지되었다.
이상의 결과를 통해 볼 때, 2% minocylcine gel을 이용한 국소약물송달법을 치석제거술 및 치근면 활 택술과 함께 사용하였을 때 임상지수의 개선과 치은 연하치태의 세균분포의 개선측면에서 성인형 치주 염 치료에 부가적인 효과가 있다고 사료된다.
VI. 참고문헌
1. O'Leary, T. J., Barrington, E. P., and Gottsegen, R. : Periodontal therapy. A summa- ry status report 1987-1988. J. Periodontol. 59:
306-310, 1988.
2. Adrianes, P. A., De Boever, J. A., and Loesche, W. J. : Bacterial invasion in root cementum and radicular dentine of periodontally diseased teeth in humans. J. Periodontol., 59: 222-230, 1988.
3. Caffesse, R. G., Sweeney, P. L., and Smith, B.
A. : Scaling and root planing with and without periodontal flap surgery. J. Clin. Periodontol., 13: 205-211, 1986.
4. Johnes, A. A., Kornman, K. S., Newbold, D.
A., and Manwell, M. A. : Clinical and microbi- ological effects of controlled-release locally delivered minocycline in periodontitis. J.
Periodontol., 65: 1058-1066, 1994.
5. Lo..
e, H., Theilade, E., and Jensen, S. B. : Experimental gingivitis in man. J. Periodontol., 36: 177-187, 1965.
6. Slots, J. : Subgingival microflora and periodon- tal disease. J. Clin. Periodontol., 6: 351-382, 1979.
7. Slots, J., and Rams, T. E. : Antibiotics in peri-
odontal therapy : advanatages and disadvan- tages. J. Clin. Periodontol., 17: 479-493, 1990.
8. Ainamo, J., Lie, T., Ellingsen, B. H., Hansen, B. F., Johansson, L-A., Karring, T., Kisch, J., Paunio, K., and Stoltz, K. : Clinical response to subgingival application of a metronidazole 25% gel compared to the effect of subgingival scaling in adult periodontitis. J. Clin.
Periodontol., 19: 723-729, 1992.
9. O‘Conneor, B. C., Newman, H. N., and Wilson, M. : Susceptibility and resistance of plaque bacteria to minocycline. J.
Periodontol., 61: 228-233, 1990.
10. Fiehn, N. E., and Westergaard, J. : Doxycycline-resistant bacteria in periodontally diseased individuals after systemic doxycy- cline therapy and in healthy individuals. Oral Microbiol. Immunol., 5: 219-222, 1990.
11. Rams, T. E., Babalola, O. O., and Slots, J. : Subgingival occurrence of enteric rods, yeasts and staphylococci after systemic doxycycline therapy. Oral Microbiol. Immunol., 5: 166- 168, 1990.
12. Kornman, K. S., and Karl, E. H. : The effect of long-term low-dose tetracycline therapy on the subgingival microflora in refractory adult periodontitis. J. Periodontol., 53: 604-610, 1982.
13. Lundstro..
m, A., Johansson, L. A., and Hamp, S. E. : Effect of combined systemic antimicro- bial therapy and mechanical plaque control in patients with recurrent periodontal disease. J.
Clin. periodontol., 11: 321-330, 1984.
14. Goodson, J. M., Haffajee, A. D., and Socransky, S. S. : Periodontal therapy by local delivery of tetracylcine. J. Clin. Periodontol., 6: 83-92, 1979.
15. Addy, M., Rawle, L., Handley, R., Newman, H. N., and Coventry, J. F. : The development
and in vitro evaluation of acrylic strips and dialysis tubings for local drug delivery. J. Periodontol., 53:
693-699, 1982.
16. Goodson, J. M., Hloborow, D., Dunn, R. L., Hogan, P. E., and Dunham, S. : Monolithic tetracycline-containing fibers for controlled delivery to periodontal pockets. J.
Periodontol., 54: 575-579, 1983.
17. Norling, T., Landing, P., Engstro..
m, S., Larsson, K., Krog, N., and Nissen, S. S. : Formulation of drug delivery system based on mixture of monoglycerides and triglycerides for use in the treatment of periodontal dis- ease. J. Clin. Periodontol., 19: 687-692, 1992.
18. Heijl, L., Dahle′n, G., Wenander, Y., and Goodson, J. M. : A 4-quadrant comparative study of periodontal treatment using tetracy- cline-containing drug delivery fibers and scal- ing. J. Clin. Periodontol., 18: 111-116, 1991.
19. Newman, M. G., Kornman, K. S., and Doherty, F. M. : A 6-month multi-center eval- uation of adjunctive tetracycline fiber therapy used in conjunction with scaling and root planing in maintenance patients : Clinical results. J. Periodontol., 65: 685-691, 1994.
20. Radvar, M., Pourtahi, N., and Kinane, D. F. : Comparison of 3 periodontal local antibiotic therapies in persistent periodontal pockets. J.
Periodontol., 67: 860-865, 1996.
21. Somayaji, B. V., Jariwala, U., Jayachandran, P., Vidyalakshmi, K., and Dudhani, R. V. : Evaluation of antimicrobial efficacy and release pattern of tetracycline and metronida- zole using a local delivery system. J.
Periodontal., 69: 409-413, 1998.
22. van Steenberghe, D., Bercy, P., Kohl, J., De Boever, J., Adriaens, P., Vanderfaeillei, A., Adriaenssen, C., Rompen, E., De Vree, H., McCarthy, E. F., and Vandenhoven, G. :
Subgingival minocycline hydrochloride oint- ment in moderate to severe chronic adult peri- dontitis : A randomized, double-blind, vehicle- controlled, multi-center study. J. Periodontol., 64: 637-644, 1993.
23. Pedrazzoli, V., Kilian, M., and Karring, T. : Comparable clinical and microbiological effects of topical subgingival application of a 25% metronidazole gel and scaling in the treatment of adult periodontitis. J. Clin.
Periodontol., 19: 715-722, 1992.
24. Timmerman, M. F., van der Weijden, G. A., van Steenbergen, T.J.M., Mantel, M.S., de Graaff, J., and van der Velden, U. : Evaluation of the long-term efficacy and safety of locally- applied minocycline in adult periodontitis patients. J. Clin. Periodontol., 23: 707-716, 1996.
25. Preus, H. R., Lassen, J., Aass, A. M., and Ciancio, S. G. : Bacterial resistance following subgingival and systemic administration of minocycline. J. Clin. Periodontol., 22; 380- 384, 1995.
26. Hey-Ri Yeom, Yoon-Jeong Park, Seung-Jin Lee, In-Cheol Rhyu, Chong-Pyoung Chung, and Russel J. Nesengard. : Clinical and micro- biological effects of minocycline-loaded microcapsules in adult periodontitis. J.
Periodontol., 68: 1102-1109, 1997.
27. Graca, M. A., Watts, T. L. P., Wilson, R. F., and Palmer, R. M. : A randomized controlled trial of a 2% minocycline gel as an adjunct to non-surgical periodontal treatment, using a design with multiple matching criteria. J. Clin.
Periodontol., 24: 249-253, 1997.
28. Hitzig, C., Fosse, T., Charbit, Y., Bitton, C., and Hannoun, L. : Effects of combined topical metronidazole and mechanical treatment on the subginigival flora in deep periodontal
pockets in cuspids and bicuspids. J.
Periodontol., 68: 613-617, 1997.
29. Kim, W-K., Chung, C-P., and Choi, S-M. : Clinical & microbiological effects of minocy- cline-loaded polycarprolactone film on adult periodontitis. 대한치주과학회지, 21: 248-262, 1991.
30. 김강주, 김동균, 김형욱, 정서영, 정종평 : 30%
minocycline을 함유한 polycaprolacton filem 의 생체내 방출역학에 관한 연구. 대한치주과 학회지. 20: 28-35, 1990.
31. Ciancio, S. G., Reynolds, H., Slots, J., Golub, L., and Zambon, J. J. : Comparison of tetracy- cline and minocycline as adjunctive antimicro- bial agents in the treatment of adult periodon- titis. J. Dent. Res., 63(Spec. Issue): 267(Abstr.
870), 1984.
32. Ciancio, S. G., Mather, M. L., and McMullen J.
A. : An evaluation of minocycline in patients with periodontal disease. J. Periodontol., 51:
530-534, 1980.
33. Baker, P. J., Evans, R. T., Coburn, R. A., and Genco, R. J. ; Tetracycline and its derivatives strongly bind to and are released from the tooth surface in active form. J. Periodontol., 54: 580-585, 1983.
34. 신형식, 한경윤, 정종평 : 미노클린 첨부제의 만성 변연성 치주염의 치료효과에 대한 유효 성과 안전성의 평가. 대한 치주과학회지, 24:
493-502, 1994.
35. Stoltze, K. : Concentration of metronidazole in periodontal pockets after application of metronidazole 25% dental gel. J. Clin.
Periodontol., 19: 698-701, 1992.
36. Stoltze, K. : Elimination of elyzol 25% dental matrix from periodontal pockets. J. Clin.
Periodontol., 22: 185-187, 1995.
37. Goodson, J. M. : Antimicrobial strategies for treatment of periodontal disease. Periodontol
2000, 5: 142-168, 1994.
38. Silness, J. and Lo..
e, H. : Periodontal disease in pregnancy. II. Correlation between oral hygiene and periodontal condition. Acta.
Odontol. Scand., 22: 121-135, 1964.
39. Lo..
e, H. and Silness, J. : Periodontal disease in pregnancy. I. Prevalence and severity. Acta.
Odontol. Scand., 21: 533-551, 1963.
40. Mu..
hlemann, H. R., and Son, S. H. : Gingival sulcus bleeding a leading symptom in initial gingivitis. Helv. Odonto. Acta., 15: 107, 1971.
41. Listgarten, M. A., and Hellde′n, L. : Relative distribution of bacteria at clinically healthy and periodontally diseased sites in humans. J.
Clin. Periodontol., 5: 115-132, 1978.
42. Tanner, A. C., Haffer, C., Bratthall, G. T., Visconti, R. A., and Socransky, S. S. : A study of the bacteria associated with advancing peri- odontitis in man. J. Clin. Periodontol., 6: 278- 307, 1979.
43. Armitage, G. C., Dickinson, W. R., Jenderseck, R. S., Levine, S. M., and Chambers, D. W. : Relationship between per- centage of subgingival spirochetes and the severity of periodontal disease. J.
Periodontol., 53: 550-556, 1982.
44. Slots, J. : Subgingival microflora and periodon- tal disease. J. Clin. Periodontol., 6: 351-382, 1979.
45. Loos, B., Claffey, N., and Crigger, M. : Effects of oral hygiene measures on clinical and microbiological parameters of periodontal dis- ease. J. Clin. Periodontol., 15: 211-216, 1988.
46. Lavanchy, D. L., Bickel, M., and Baehni, P. C.
: The effect of plaque control after scaling and root planing on the subgingival microflora in human periodontitis. J. Clin. Periodontol., 14:
295-299, 1987.
47. Greenstein, G., and Polson, A. : The role of
local drug delivery in the management of periodon- tal diseases : A comprehensive review. J.
Periodontol., 69: 507-520, 1998.
48. Satomi, A., Uraguchi, R., Noguchi, T. et al. : Minocycline-HCl concentration in periodontal pocket after administration of LS-007. J. Japan Soc. Periodontol., 29: 937-943, 1987.
49. Hagiwara, S., Takamatsu, N., Tominaga, Y., and Umeda, M. : Subgingival distribution of
periodontopathic bacteria in adult peridontitis and their susceptibility to minocyclie-HCl. J.
Periodontol., 69: 92-99, 1998.
50. 정미현, 권영혁, 허 익, 이만섭, 박준봉 : Minocycline 국소 약물 방출제제의 치주질환 치료효과. 대한치주과학회지 28: 37-56, 1998.
-Abstract-
Effects of 2% minocycline gel as an adjunct to scaling and root planing on the treatment of adult periodontitis
Young-Hyuk Kwon, Ji-Won Park, Yeek Herr, Joon-Bong Park Department of periodontology, College of Dentistry, Kyung Hee University
The objective of the present study was to evaluate the clinical and microbiological effects of scaling and root planing combined with local application of 2% minocycline gel to patients with moderate to advanced chronic adult periodontitis. 27 healthy patients with moderate to advanced chronic adult periodontitis were enrolled in the study. The quadrants that had 2 or more teeth with 5∼8mm probing pocket depth and radiographic evi- dence of alveolar bone loss were selected and divided into test side and control side according to the split- mouth design.
All patients received standardized oral hygiene instructions at the beginning of the study. Subsequently scal- ing and root plaining was performed on all remaining teeth until 0 week. The 2% minocycline gel was applied to periodontal pocket at 0, 1, 2, 3week in the test side. The normal saline was irrigated subgingivally for about 30 seconds in the control side. The clinical and microbiological analysis was carried out at 0, 4, 8, and 12weeks.
The results of this study were as follows;
1. 2% minocycline gel delivered subgingivally as an adjunct to scaling and root planing provided benefit in reducing sulcular bleeding index and pocket depth than the use of normal saline.
2. The relative proportion of cocci and non-motile bacteria was increased in the test and control groups with time, and there was no statistically significantdifference between two groups.
3. The proportion of spirochetes was slowly reduced in the control group, but, inthe test group, they were remarkably reduced from the 4th week, and there was a statistically significant difference between two groups.
4. In both groups, the relative proportion of motile rods was notably decreasedat the beginning of the study, and remained until 12th week in the test group,but, in the control group, they were slowly increased from the 4th weekand finally similar to that of the initial examination.
In conclusion, local application of 2% minocycline gel may be effective in the clinical and microbiological aspects as an adjunct to scaling and root planing in periodontal disease sites.