DOI 10.17480/psk.2020.64.4.243
종 설(Review)
거세저항성 전립선암 치료제 개발 동향
김지원*·이준녕**·하윤석**·권태균**·이상규*,#
*경북대학교 약학대학 약학연구소, **경북대학교 의과대학 비뇨기과학교실
Trends in the Development of Castration-resistant Prostate Cancer Treatment
Jiwon Kim*, Jun Nyung Lee**, Yun-Sok Ha**, Tae Gyun Kwon**, and Sangkyu Lee*,#
*Research Institute of Pharmaceutical Sciences, College of Pharmacy, Kyungpook National University
**Department of Urology, School of Medicine, Kyungpook National University
(Received June 4, 2020; Revised July 20, 2020; Accepted July 22, 2020)
Abstract Prostate cancer is one of the most common male cancer. It tends to be known as “mild cancer” due to its high five-year survival rate. However, some patients develop castration-resistant prostate cancer (CRPC) during androgen deprivation therapy (ADT) treatment, with high metastasis and poor prognosis. In addition to conventional ADT treatments, specific treatments are implemented for CRPC. There are four second-generation anti-androgen drugs, taxane chemotherapy, and immunotherapy using vaccines and monoclonal antibodies. This review paper outlines the mechanism of prostate cancer leading to CRPC and reviews the standard treatment of CRPC. It also summarized the trends of anticancer drugs under clinical trials to obtain CRPC as an additional indication.
Keywords castration-resistant prostate cancer, anti-androgens, prostate cancer, chemotherapy
서 론(Introduction)
세계 보건기구의 World Cancer report에 따르면 전립선 암은 전 세계 남성암 중 발병률 2위를 차지하고 있다.
1)미국이나 영 국보다는 발병률이 낮지만, 우리나라에서도 전체 남성암 발생률 4 위를 기록할 정도로 흔한 암이다.
2)전립선 암의 5년 생존율은 94.1%로 ‘순한 암’으로 인식되는 경향이 있지만, 호르몬차단요 법(androgen deprivation therapy, ADT)에 실패한 환자들은 거세 저항성 전립선암(Castration-Resistant Prostate Cancer, CRPC)으로 진행되는 경우 생존율이 급격히 감소한다.
3)CRPC 는 지난 10년 동안 docetaxel을 기반으로 치료가 이루어졌고, 최근에는 CRPC 로 진행되는 기전을 선택적 표적 하는 치료제들이 개발되고 있 다. 하지만 현재까지 CRPC를 적응증으로 FDA 승인을 받은 약 제는 6종에 불과하다.
4)추가적인 치료제 개발과 함께, 치료제 내 성 및 변이에 대한 대비책 연구가 활발히 진행되고 있으며, 정 밀의학을 기반으로 한 유전자 연구 또한 진행 중에 있다. 이번 논문에서는 전립선 암에서 CPRC로 진행되는 분자학적 기전을
고찰하고, 표적에 따른 현재 CRPC 치료에 사용되는 표준요법 약물을 고찰하였다.
1. 전립선암의 CRPC로의 진행 기전 1) Intra-tumoral Androgen Biosynthesis
CRPC 환자들은 ADT요법을 통해 혈중 testosterone 농도를 거 세수준(<50 ng/dL)으로 유지함에도 불구하고 PSA 수치의 증가 나 임상소견의 악화를 보인다.
5)성공적인 ADT 치료에도 종양 이 거세저항성을 띄는 것은 세포 내 미량의 androgen 전구체 만 으로 testosterone 및 dihydrotestosterone (DHT)을 생성할 수 있도 록 세포 내 스테로이드 합성효소 유전자의 발현을 증가시키기 때문이다.
6)그 중 cytochrome P450 17A1 (CYP17A), aldo-keto reductase family 1 member C3 (AKR1C3,17 β-HSD5), 17β- hydroxysteroid dehydrogenase type 3 (17-HSD3), 5 α-reductase (SRD5A) 등의 스테로이드합성 효소들은 치료약물개발의 대표적 표적이 되고 있다(Fig. 1). 스테로이드 합성효소의 유전자의 발 현의 증가는 전립선 암 세포 내의 testosterone 및 DHT 농도를 ADT 치료 이전과 비슷한 수준으로 되돌리기 때문에암세포의 분 화와 항상성이 회복된다.
7)현재 CRPC의 androgen 생합성 억제 단계를 표적으로 하는 FDA 승인 치료제는 Abiraterone acetate (ZYTIGA
®) 가 유일하다.
TAK-700 (Oteronel), TOK-001 (Galeterone) 등 유망한 신약후보 물질의 임상이 연이어 실패하였고, 또 다른 CYP억제제인 keto-
#
Corresponding author
Sangkyu Lee, Ph.D., Associate Professor, College of Pharmacy, Research Institute of Pharmaceutical Sciences, Kyungpook National University, 80 Daehak-ro, Buk-gu 41566, Republic of Korea Tel: +82-53-950-8571, Fax: +82-53-950-8557
E-mail: [email protected]
conazole (Antifungal)
8)의 경우, 낮은 CYP 특이성과 높은 독성으 로 off-label로 사용되나 선호되지 않는다.
9)하지만 최근 CYP17 효소를 표적으로 하는 안드로겐 생합성 저해물질 VT-464 (Sevit- eronel) 의 임상(2상)이 FDA의 Fast-track 지정을 받아 진행 중이 고, androgen 생합성 과정의 중요 효소인 SRD5A를 표적으로 하 는양성 전립선 비대증 치료제 Dutasteride (AVODART
®) 을 CRPC 치료에 적용을 위한 연구가 수행되고 있다.
10)2 세대 항 androgen 약물의 첫 번째 주자인 Abiraterone acetate 은 CYP17을 비가역적으로 저해하여 testosterone 합성을 억제한 다. Glucocorticoid, mineralcorticoid 형성에 관여하는 CYP11B1과 CYP11B2를 저해하지 않으면서 androgen 생합성과 관련된 CYP17A 만을 저해하는 높은 선택성을 가진다.
11)약물은 경구 pro-drug 인 acetate염으로 투여되며 스테로이드(prednisolone)와 함 께 병용하여야 한다. 환자 전신의 순환 testosterone 농도를 줄여 주어 암의 진행을 저지하고 전반적인 생존율 개선효과를 보인 다.
12)주요 부작용으로는 mineralcorticoid 저하로 인한 저칼륨혈 증, 고혈압, 체액과잉 등이 나타날 수 있다.
13)2) Persistent Androgen Receptor activity
대부분의 거세저항성 전립선암은 거세수준의 androgen 농도에
도 불구하고 androgen receptor (AR)의 지속적인 전사활동으로 인해 종양세포가 성장한다. 지속적인 AR의 전사활동을 유도하 는 다양한 기전이 있지만, 위의 Fig. 1에 제시된 9가지의 경우 가 주요인으로 작용한다.
(1) AR gene amplification, protein over-expression
ADT 요법으로 인해 매우 낮아진 혈중 androgen 농도에도 전 립선 종양세포는 증식과 분화를 지속할 수 있도록 수용체를 조 절한다. CRPC 환자 30-50%에서 AR gene 증폭이 발견되며 유 전자 증폭은 AR 단백질의 과발현을 유도한다.
14,15)CRPC 환자 들은 AR 단백질의 발현이 약 80% 이상 증가되어 있으며,
16)Enzalutamide 치료를 받은 환자에서 증폭현상이 빈번히 관찰된다.
17)(2) AR gain of function mutation
약 15-30%의 CRPC 환자가 AR 유전자에 점 돌연변이를 갖
고 있다.
18)가장 빈번한 돌연변이는 Ligand-Binding domain
(LBD) 부분에서 일어나며 N-Terminal domain (NTD)에서의 돌
연변이가 그 뒤를 잇는다.
19)AR 의 LBD에서 발생하는 점 돌연
변이는 androgen 없이도 AR signaling을 유도한다. Androgen이
아닌 glucocorticoid를 통해 수용체를 활성화시키거나(L702H변
Fig. 1. Scheme of androgen biosynthesis pathway in adrenal cortex cells and regulating factors for persistent androgen receptor activity
in prostate tumor cells.
이),
20)progesterone이나 estrogen 그리고 1세대 항안드로겐(fluta- mide 계)를 통해 수용체를 활성화시킬 수 있으며(T878A 변
이)
16,21)수용체 antagonist를 agonist로 작용하게 하는 변이(F877L
변이)도 연구되고 있다.
22)이러한 변이들은 일반 전립선암의 호 르몬 억제 저항성으로 진행뿐만 아니라 CRPC의 치료제에도 내 성을 나타내는 기전이 된다.
(3) AR splice variants (ARVs)
야생형(wild type)의 온전한 AR은 NTD (exon 1에 의해 암호화 ), DNA binding domain (DBD, exon2-3 에 의해 암호화), hinge 영 역(exon 4에 의해 암호화), LBD (exon 5-8에 의해 암호화)으로 구 성된다. 유전자 스플라이싱 과정에 문제가 생겨 LBD에 결함이 생긴 경우 리간드와 무관하게 지속적인 AR 활성을 유도하여 CRPC 진행에 결정적인 역할을 한다. AR-V1과 AR-V7이 가장 흔 한 변이인데, 일반 전립선암 환자에서보다 CRPC 환자에서 20배 이상 발현률이 높다.
23)특히 AR-V7변이는 많은 CRPC 환자들에 서 치료제 내성을 유발하여 가장 많은 연구가 진행되고 있다.
(4) Ligand independent AR NTD trans-activation
IL-6 나 각종 cytokine들은 AR의 NTD(N-terminal domain)에 결 합하여 androgen 없이도 AR의 전사활동을 자극한다.
24)IL-6 는 특정 유전자들의 발현을 조절하여 종양세포의 apoptosis를 억제 하며,
25)IL-4는 coactivator로서 AR의 신호전달에 영향을 끼쳐 AR 을 활성화 CRPC로의 진행을 촉진한다.
26)IL-8 역시 CRPC 환자에서 과발현 되어있는 사이토카인이고, 이미 진행된 CRPC 의 혈관신생과 전이를 촉진한다.
27)(5) Progesterone, Glucocorticoid receptor activation
CRPC 환자들에게 progesterone receptor (PR)가 상향조절 되어 있고,
28)glucocorticoid receptor (GR) 역시 과발현되어 있다. GR 의 전사과정은 AR 경로와 상당 부분 공유된다.
29)때문에 GR 활 성은 ADT로 인해 androgen이 저하되어 있는 상태의 환자에서 AR 경로를 유지시키는 역할을 할 수 있다.
30)GR 의 활성을 억 제하여 CRPC의 진행을 미루는 연구가 진행 중이며, AR antagonist (Enzalutamide) 에 반응이 없는 CRPC 환자들에게 치료 타겟이 될 수 있다.
31)Progesterone receptor (PR) 또한 AR subset의 전사활 동을 조절하고 종양세포의 증식을 조절하는 역할을 하는데, 이 는 PR이 AR과 구조적인 유사성을 가지기 때문이다. 이로 인 해, 많은 항안드로겐 치료제는 AR의 LBD와 유사한 PR을 충분 히 억제할 수 있다.
(6) Reciprocal regulation of PI3K/AKT/mTOR pathway PI3K/AKT pathway 는 대표적인 종양유발 경로이다. 종양세포 내 종양억제 단백질인 PTEN이 고갈되면 활성화되는데 종양세 포 내 AR signaling 및 MAPK cascade와 협업하며 AR signal- ing 을 촉진한다.
32)전립선암의 거세저항성 진행과 분화기전에 핵 심적인 역할을 하는 것으로 주목되고 있다.
33)(7) Coactivator overexpressoion
Coactivator 는 AR과 직접 결합하여 전사활동을 촉진하기에, Steroid Receptor Coactivators (SRC) 을 비롯한 coactivator들의 비 정상적인 상향조절은 CRPC에서 두드러지는 특징 중 하나이 다.
34)SRC-1 의 과발현은 종양의 공격성(aggressiveness)과 관련이 있고,
35)SRC-2의 과발현은 PI3K 경로와 연관되어 전이성 종양 과 CRPC에서 많이 발견된다.
36)SRC-3 의 과발현은 종양억제 단 백질인 PTEN을 억제하여 종양유발경로를 활성화, CRPC에서 수 치상승이 관찰되는 형태이다.
37)(8) Neuro-endocrine trans-differentiation
약 25%의 CRPC 환자에게서 종양은 neuroendocrine prostate cancer (NEPC, 신경내분비종양) 형태로 관찰되며 그 빈도는 점 점 늘어나는 추세이다.
38)AR 의 소실 그리고 synaptophysin, chro- mogranin A 와 같은 신경내분비지표들의 증가로 특징될 수 있고 ADT 요법 및 항안드로겐 요법에 불응한다.
39)2. 전립선암 및 CRPC 치료제 개발 동향
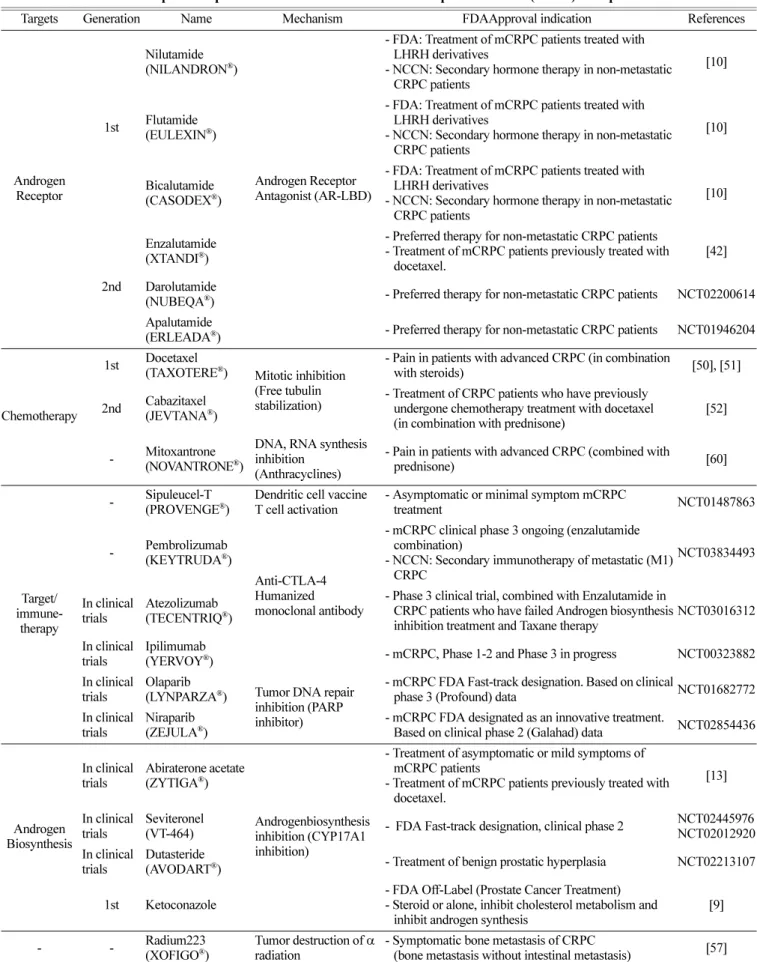
NCCN Guideline (ver1. 2020)과 국내 거세저항성 전립선암 (CRPC) 치료지침을 기반으로 현재 CRPC 치료에 사용되는 약 물을 종합하여 정리하였다(Table 1). 또한 CRPC를 추가 적응증 으로 승인취득을 위해 임상시험평가 중인 표적항암제, 면역제제 도 함께 정리하였다.
1) Chemotherapy for CRPC: androgen 억제요법에사용되는 치료제 Enzalutamide (XTANDI
®) 는 2세대 항안드로겐 제제이자 경구 AR antagonist 로서 전이성 및 비전이성 CRPC에 모두 적응증이 있는 치료제이다. AR의 LBD에 높은 친화력으로 결합하여 AR 과 androgen의 결합을 저해할 뿐만 아니라, androgen과 AR 복 합체의 핵 내 이동을 막고 복합체의 DNA 부착을 억제하며 coactivator 의 결집을 저해한다.
40)1 세대 항안드로겐 제제와 다르 게 AR agonist 작용이 없기 때문에 anti-androgen withdrawal syndrome 이 나타나지 않으며,
41)주요 부작용으로는 피로, 안면홍 조, 설사, 요통 등이 있고 고 함량 요법에서의 발작이 관찰되기 도 한다.
42)Apalutamide (ERLEADA
®)는 2018년 전이성 CRPC에 적응증 승인을 받은 2세대 항안드로겐 제제이다. Apalutamide 역시 AR 의 LBD에 결합하여 androgen-AR 복합체의 핵 내 유입과 DNA 부착을 억제한다. AR에 높은 친화성을 가질 뿐만 아니라, CRPC 종양세포에 과발현된 AR에도 온전한 길항제 효과를 유지하며 전사억제 및 세포성장을 억제한다.
43)Enzalutamide와 마찬가지로 피로, 안면홍조, 설사 등의 부작용이 있다. 다만 AR 특이성이 높아 다른 steroid receptor (ex. PR)에 영향이 적고, enzalutamide 보다 4배정도 낮은 혈액뇌장벽(blood-brain barrier) 투과율로 발 작 위험이 낮은 것은 장점으로 꼽힌다.
43)Darolutamide (NUBEQA
®) 는 가장 최근에 비전이성 CRPC 적
응증으로 승인된 신약으로, Enzalutamide와 Apalutmide보다 AR
Table 1. Trends in the development of prostate cancer and castration-resistant prostate cancer (CRPC) therapeutics
Targets Generation Name Mechanism FDAApproval indication References
Androgen Receptor
1st
Nilutamide (NILANDRON
®)
Androgen Receptor Antagonist (AR-LBD)
- FDA: Treatment of mCRPC patients treated with LHRH derivatives
- NCCN: Secondary hormone therapy in non-metastatic CRPC patients
[10]
Flutamide (EULEXIN
®)
- FDA: Treatment of mCRPC patients treated with LHRH derivatives
- NCCN: Secondary hormone therapy in non-metastatic CRPC patients
[10]
Bicalutamide (CASODEX
®)
- FDA: Treatment of mCRPC patients treated with LHRH derivatives
- NCCN: Secondary hormone therapy in non-metastatic CRPC patients
[10]
2nd
Enzalutamide (XTANDI
®)
- Preferred therapy for non-metastatic CRPC patients - Treatment of mCRPC patients previously treated with
docetaxel.
[42]
Darolutamide
(NUBEQA
®) - Preferred therapy for non-metastatic CRPC patients NCT02200614 Apalutamide
(ERLEADA
®) - Preferred therapy for non-metastatic CRPC patients NCT01946204
Chemotherapy
1st Docetaxel
(TAXOTERE
®) Mitotic inhibition (Free tubulin stabilization)
- Pain in patients with advanced CRPC (in combination
with steroids) [50], [51]
2nd Cabazitaxel (JEVTANA
®)
- Treatment of CRPC patients who have previously undergone chemotherapy treatment with docetaxel (in combination with prednisone)
[52]
- Mitoxantrone (NOVANTRONE
®)
DNA, RNA synthesis inhibition
(Anthracyclines)
- Pain in patients with advanced CRPC (combined with
prednisone) [60]
Target/
immune- therapy
- Sipuleucel-T (PROVENGE
®)
Dendritic cell vaccine T cell activation
- Asymptomatic or minimal symptom mCRPC
treatment NCT01487863
- Pembrolizumab (KEYTRUDA
®)
Anti-CTLA-4 Humanized monoclonal antibody
- mCRPC clinical phase 3 ongoing (enzalutamide combination)
- NCCN: Secondary immunotherapy of metastatic (M1) CRPC
NCT03834493
In clinical trials
Atezolizumab (TECENTRIQ
®)
- Phase 3 clinical trial, combined with Enzalutamide in CRPC patients who have failed Androgen biosynthesis inhibition treatment and Taxane therapy
NCT03016312
In clinical trials
Ipilimumab
(YERVOY
®) - mCRPC, Phase 1-2 and Phase 3 in progress NCT00323882 In clinical
trials
Olaparib
(LYNPARZA
®) Tumor DNA repair inhibition (PARP inhibitor)
- mCRPC FDA Fast-track designation. Based on clinical
phase 3 (Profound) data NCT01682772 In clinical
trials
Niraparib (ZEJULA
®)
- mCRPC FDA designated as an innovative treatment.
Based on clinical phase 2 (Galahad) data NCT02854436
Androgen Biosynthesis
In clinical trials
Abiraterone acetate (ZYTIGA
®)
Androgenbiosynthesis inhibition (CYP17A1 inhibition)
- Treatment of asymptomatic or mild symptoms of mCRPC patients
- Treatment of mCRPC patients previously treated with docetaxel.
[13]
In clinical trials
Seviteronel
(VT-464) - FDA Fast-track designation, clinical phase 2 NCT02445976 NCT02012920 In clinical
trials
Dutasteride
(AVODART
®) - Treatment of benign prostatic hyperplasia NCT02213107
1st Ketoconazole
- FDA Off-Label (Prostate Cancer Treatment) - Steroid or alone, inhibit cholesterol metabolism and
inhibit androgen synthesis
[9]
- - Radium223
(XOFIGO
®)
Tumor destruction of α radiation
- Symptomatic bone metastasis of CRPC
(bone metastasis without intestinal metastasis) [57]
에 높은 친화도를 나타내 우수한 효능 보인다.
44)야생형의 AR 과 변이된 AR모두 억제하는 것을 특장점으로 갖는데, 수용체 antagonist를 agonist로 전환하는 AR F876L 변이에도 작용할 수 있어 CRPC 치료제 내성에도 적용될 것으로 기대된다.
45)Enza- lutamide, apalutamide 와 유사한 부작용을 나타내지만, BBB를 통 과하지 않아 발작의 위험이 없다.
2) Chemotherapy for CRPC: Free tubulin 을 안정화하는 Tax- ane계 치료제
Taxane 계 약물의 주요 기전은 microtubule 안정화를 통해 이 에 영향을 받는 AR의 hinge 영역을 저해하여 AR의 핵 내 이동 (Nuclear translocation) 및 전사활동을 하향 조절하여 암의 진행 을 억제하는 것이다.
46)Docetaxel은 전립선암뿐만 아니라 위암, 유방암, 비소세포폐암 등 다양한 암 치료에 사용되는 유사분열 억제제이다. 지난 2004년, Docetaxel이 전이성 거세저항성 전립 선암 환자의 생존율을 높이는 것이 입증되며,
47,48)10여 년 동안 거세저항성 전립선암의 가장 효과적인 치료제로 사용되어 왔고 현재까지도 1차 요법으로 선호되고 있다.
Cabazitaxel (JEVTANA
®)은 docetaxel의 7,10-dimethoxy 유 사체로 지난 2011년 FDA승인을 받은 전이성 CRPC (metastatic CRPC, mCRPC) 치료제이다. Docetaxel 치료경험이 있는 mCRPC 환자에 2차 요법으로 사용되며, docetaxel과 enzalutamide 또는 abiraterone의 치료 실패 후에도 효과를 볼 수 있어 주목받고 있다.
49)3) Target, immunotherapy for CRPC: 다양한 신약들의 적응증 확대를 위한 시도
Sipuluecel-T (PROVENGE
®)는 CRPC를 적응증으로 하는 치료백신이다. 환자의 수지상세포(CD54
+cells)을 수집, 전립 선암세포 유래 단백질과 조합한 후 체내로 다시 주입하여 전 립선 종양세포를 죽이는 자가면역을 유도한다.
50)생존율 개선 에 유의미한 효과가 입증되어 mCRPC 면역요법에 선호약제 로 사용된다.
Pembrolizumab (KEYTRUDA
®)과 Atezolizumab (TECEN- TRIQ
®) 은 각각 항PD-1, PD-L1 인간화 단 클론항체로 T세포의 표적에 결합하여 항종양 면역반응을 유도한다. 두 약제 모두 현 재 mCRPC에 enzalutamide와 병용요법으로 FDA 승인을 얻기 위해 임상시험이 진행 중이다.
51)Ipilimumab (YERVOY
®) 은 흑색 종 치료에 사용되는 항 CTLA-4 (Cytotoxic T-Lymphocyte asso- ciated Antigen 4) 제제이다. T 세포 활성화를 통해 항암 면역반 응을 유도할 수 있다. 방사선요법과 병용하여 mCRPC 치료에 효과를 나타내며
52)활발한 임상이 진행 중이다.
표적항암제의 CRPC 적응증 획득을 위한 연구도 진행 중이 다. 전립선암의 진행단계에서 DNA-손상회복기전(DNA-damage repair) 의 결핍이 중요한 원인이 될 수 있다. 특히 상동재조합 (double-strand DNA) 에 의해 이중 가닥 DNA 파괴를 복구하는 능력이 손상되는 종양은 폴리(ADP) 리보스 폴리머라제(PARP)
의 억제를 통한 DNA 단일 가닥 파괴의 복구 차단에 매우 민 감하다.
53)Olaparib 과 niraparib은 PARP 억제제로서 BRCA 변이 종양세포에 합성치사(synthetic lethality)를 유도하는 약물이다. 그 중 Olaparib은 mCRPC에 단독요법으로도 효과를 보이지만,
54)기 존 항안드로겐 요법과 병용하여 mCRPC의 무진행 생존기간을 유의미하게 연장시키는 결과를 나타내 주목받고 있다.
55)4) Radiopharmaceutical Therapy For CRPC: Treatment for bone metastasis
많은 거세저항성 전립선암 환자들이 전이로 인한 합병증을 겪 게 되는데, 그 중 종양이 뼈로 전이하게 되어 척추를 압박하는 골절이 발생하거나 척수압박 증상이 나타나는 것이 가장 흔하 다.
56)Radium 223 dichloride (XOFIGO
®) 은 내장전이는 없고 골 전이로 인한 증상이 있는 CRPC 환자에게 투여한다. Radium 223 은 종양세포를 파괴하는 입자이며,
57)종양세포 DNA의 비가역적 인 손상을 유발한다.
58)다른 고식적 방사선 치료와 달리 생존율 에 유의미한 개선을 보이지만, 부작용으로는 호중구감소증, 혈 소판 감소증이 있어 혈액학적 수치검사 확인 후 치료를 진행한다.
59)결 론(Conclusion)
Androgen receptor signaling pathway와 intratumoralsteroidgen- esis 기전은 거세저항성 전립선암의 진행과 CRPC 치료 과정 중 내성에 중요한 역할을 한다. 현재효과가 높은 치료제가 임상에 쓰이는 중이고 새로운 치료제 또한 개발되고 있지만, CRPC로 의 진행이 완벽하게 억제하지 못하기 때문에 전립선 암의 확실 한 정복을 위해 획기적인 약물의 등장은 여전히 절실하다. 치료 제 내성에 대한 연구를 기반으로 종양의 약물내성에 대비책이 있는 치료제가 필요하고, 유전자적 관점에서의 정밀의학 연구 또한 활발해져서 CRPC 환자들에게 다양한 치료 선택권이 주어 지기를 기대해본다.
Conflict of Interest
모든 저자는 이해 상충을 가지고 있지 않음을 선언한다.
References