서론
Idiopathic pleuroparenchymal fibroelastosis (이하 IPPFE)는 주로 양측 폐상엽 첨부의 흉막과 흉막하 폐실질에 섬유화를 일 으키는 드문 질환으로 최근에 희귀 간질성 폐렴에 포함되었다 (1). IPPFE는 남성과 여성의 비율이 보고에 따라 차이가 없거나 남성이 2배 정도 많은 것으로 되어 있다(2). 영상의학적으로는 주로 양측성 폐 첨부 흉막 비후, 상부 폐의 흉막하를 따라 존재 하는 폐 실질에 불규칙한 모양의 증가음영, 그리고 폐 용적 감 소 등의 소견을 보인다(1, 3, 4). 병리학적으로는 흉막과 흉막 하에 위치한 폐 실질에 탄력섬유증(elastosis)과 폐엽 내 섬유화 (intraalevolar fibrosis)를 보이는 것이 특징적이다. 원인으로는 정확히 알려진 것이 없으나 반복적인 감염과 자가면역, 유전적 요소가 관련이 있을 것으로 추측되고 있다(2). 저자들은 호흡 곤란을 호소하는 57세 여자에서 수년간 점차 진행하는 양측 폐 상엽 흉막하 병변의 영상소견을 보이고 수술적 생검에서 IPPFE 로 진단된 증례를 경험하였다. IPPFE는 최근 들어 증례 보고가
되고 있는 드문 질환으로, 이 질환의 장기적 진행과정을 잘 보 여주는 예로써 보고하고자 한다.
증례 보고
57세 여자 환자가 8년 전부터 경미한 호흡곤란과 기침을 호소 하다가 최근 2년 전부터 증상이 악화되었다. 흡연력은 없었으며 가족력이나 직업력상 특이 사항은 없었다. 관절통과 입 마름 증 상이 있었고 폐 청진 소견에서 경도의 수포음(crackle)이 있었다.
신체검사에서 finger clubbing 등의 다른 이상소견은 보이지 않았 다. Complete blood cell count, C-reactive protein, erythrocyte sedimentation rate를 포함한 혈액검사에서 이상소견은 보이지 않았고 자가면역질환 항체검사에서도 이상소견은 없었다. 내원 2년 전 시행된 폐기능 검사(pulmonary function test)상 forced vital capacity (이하 FVC, % predicted) 82, forced expiratory volume in one second (이하 FEV1, % predicted) 93, FEV1/ FVC (% predicted) 83으로 제한성 폐질환의 소견을 보였고, 내
J Korean Soc Radiol 2014;70(4):255-259 http://dx.doi.org/10.3348/jksr.2014.70.4.255
Received December 22, 2013; Accepted February 14, 2014 Corresponding author: Eun Jin Chae, MD
Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 138-736, Korea.
Tel. 82-2-3010-5389 Fax. 82-2-476-4719 E-mail: [email protected]
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distri- bution, and reproduction in any medium, provided the original work is properly cited.
Idiopathic pleuroparenchymal fibroelastosis (IPPFE) is a recently described, very rare type of fibrotic interstitial lung disease predominantly involving subpleural areas of both upper lungs. IPPFE has distinctive radiologic and pathologic features: progres- sive subpleural opacity with fibrotic changes, predominantly in upper lungs, and dense elastic component on histology. We experienced one case of surgically con- firmed IPPFE, with progression of radiologic findings on the serial CT examinations.
We herein report the characteristic radiologic features of IPPFE with pathologic and clinical manifestations.
Index terms
Idiopathic Pleuroparenchymal Fibroelastosis Interstitial Lung Disease
Upper Lobe Fibrosis Lung
Idiopathic Pleuroparenchymal Fibroelastosis, a Rare Entity of Interstitial Pneumonia: A Case Report
1드문 간질성 폐렴인 Idiopathic Pleuroparenchymal Fibroelastosis: 증례 보고
1Jong Chun Park, MD
1,2, Eun Jin Chae, MD
1, Joon Seon Song, MD
31Department of Radiology and Research Institute of Radiology, 3Department of Pathology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea
2Department of Radiology, School of Medicine, Catholic University of Daegu, Daegu, Korea
상엽의 흉막하 음영의 증가 및 폐 용적감소가 점차 진행해 왔 다. 그리고 그 정도는 보다 경미하였지만 양측 하엽의 흉막하 망상음영 및 용적감소도 서서히 진행하였다(Fig. 2A-C).
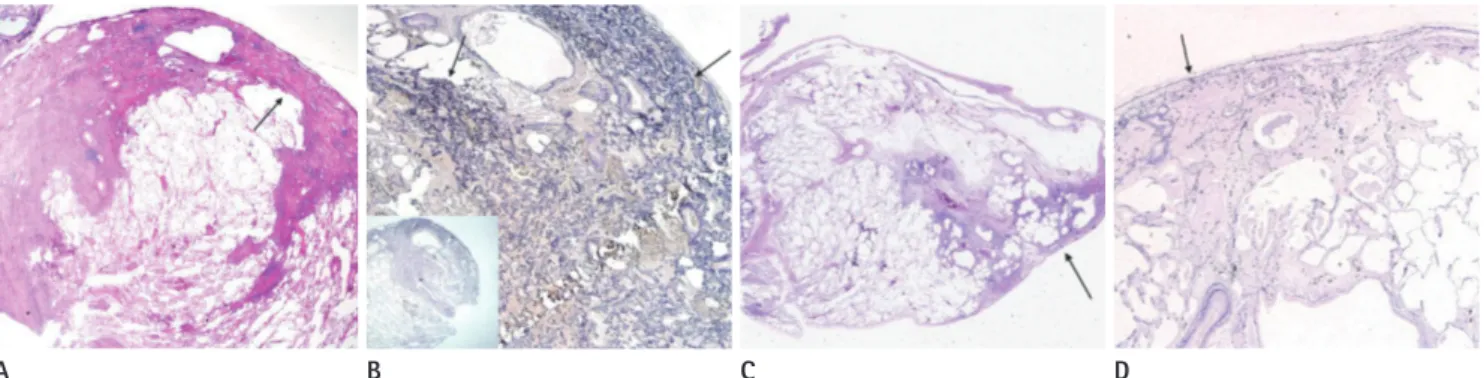
비디오 보조 흉강경(video-assisted thoracoscopy)을 이용하 여 우상엽과 우하엽의 흉막하 병변에 대해 수술적 생검을 시행 하였다. 병리소견상 우상엽의 병변은 흉막하를 따라 치밀한 섬 유화를 보였으며(Fig. 3A) Elastic Van Geison 염색에서 흉막 하에 치밀하고 불규칙하게 분포하는 탄력 섬유(elastic fiber)가 관찰되었다(Fig. 3B). 우하엽은 일시적 다양성(temporal het- erogeneity)을 보이는 흉막하 섬유화가 군데군데 분포하였고 섬유아세포 병소(fibroblastic foci)가 보였다(Fig. 3C). Elastic Van Geison 염색에서는 정상 폐 조직에서 보이는 정도의 탄력 섬유(elastic fiber)가 흉막하에서 관찰되었다(Fig. 3D). 최종적 으로 우상엽의 병변은 IPPFE로 우하엽의 병변은 초기 상용 간 질성 폐렴[early usual interstitial pneumonia (이하 UIP)]으로 기관지 폐포세척검사(bronchoalveolarlavage)상 백혈구(white
blood cell) 100 × 104 cells/mL, 호산구(eosinophil) 1%, 호중 구(neutrophil) 6%, 대식세포(macrophage) 84%로 경도의 호 중구(neutrophil) 증가 소견을 보였다. 과거력상 2년 전 타원에 서 시행한 객담검사 중 중합효소연쇄반응(polymerase chain reaction) 검사에서 비항산성 결핵균(nontuberculous mycobac- teria)인 Mycobacterium avium 양성 소견이 나온 적이 있었다.
당시의 CT에서 우중엽에 중심 소엽성 결절이 국소적으로 있었 으나 추적 CT에서 우중엽의 병변은 소실되었고 이후 객담검사 에서도 음성 소견을 보였다.
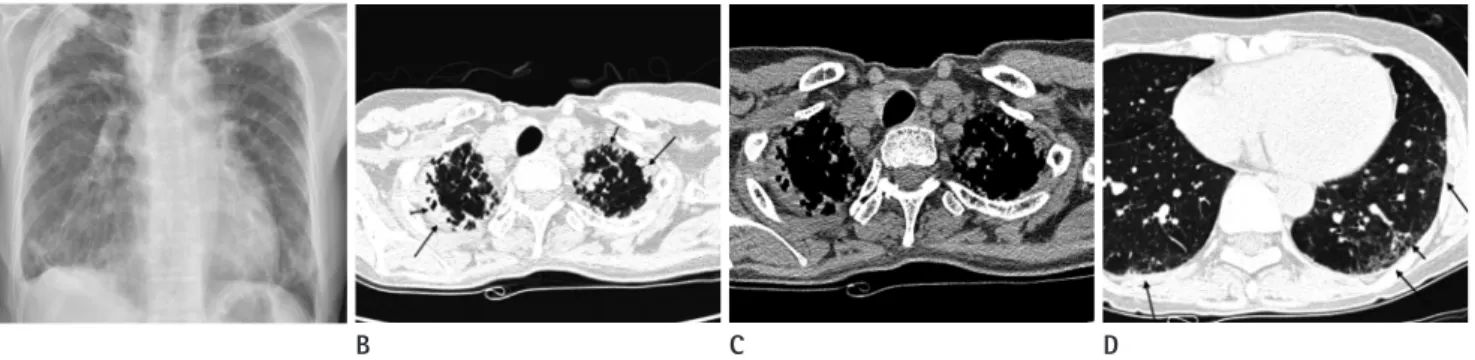
내원시 실시한 흉부 후전 영상에서 양측 폐의 상부에 불규칙 한 모양의 흉막하 경화소견과 함께 폐 용적이 감소되어 있었다 (Fig. 1A). CT 영상에서는 주로 양측 폐 상부에 흉막하 불규칙 음영증가, 흉막 비후, 그리고 견인성 기관지 확장증이 나타났다 (Fig. 1B, C). 폐 하부에는 흉막하 망상음영과 견인성 기관지
Fig. 2. Coronal reformation CT images shows progressive subpleural irregular opacities and traction bronchiectasis with volume loss in both up- per lungs, and less progressive subpleural reticular opacities with volume loss in both lower lungs than upper lungs; 8 years ago (A), 2 years ago (B), present (C).
B
A C
Fig. 1. A 57-year-old female who showed fibrotic interstitial disease predominantly involves both apical lungs.
A. Chest radiograph shows bilateral irregular opacities with volume loss and hilar elevation in the subpleural area of both upper lungs.
B, C. CT shows bilateral subpleural irregular opacities, pleural thickening (long arrows) and traction bronchiolectasis (short arrows) in both upper lobes on lung window setting (B) and mediastinal setting (C).
D. CT shows subpleural reticular opacities (long arrows) with mild traction bronchiectasis (short arrow) in both lower lobes.
A B C D
반한다. CT 영상에서 폐 상엽에 위치하는 진행하는 흉막하 불 규칙 음영으로 나타나고 견인성 기관지확장증과 폐 용적감소가 보이며 망상음영과 벌집모양 음영, 중심 소엽성 결절성 병변도 보고되고 있다(2-5). 보고된 문헌의 증례들 중 많은 수에서 폐 하엽에서도 간질성 음영이 동반되었는데, 상엽의 병변보다는 범 위와 정도가 경미하였으며, 상엽의 병변이 진행되면서 같이 진 행하는 양상이었다. 병리 소견에서 폐하엽에서는 탄력섬유증 (fibroelastosis)이 없거나 일부에서 관찰되었고 상엽의 병변보다 경미한 수준이었다(2, 4). 이러한 폐하엽의 병변들은 IPPFE와 공존하는 다른 형태의 간질성 폐렴을 시사하고 있다(2).
IPPFE 진단을 위해서는 폐 상엽의 섬유화를 초래할 수 있는 다른 원인들, 즉 흡입손상에 의한 섬유화, 석면폐증, 방사선손 상, 항암제부작용, 만성 과민성 폐렴, 교원질-혈관성 질환(col- lagen vascular disease), 골수 이식과 폐 이식의 부작용 등이 배 제되어야 한다(2, 5, 6). 흡입손상, 방사선손상, 항암제 부작용 등은 자세한 직업력과 과거력 조사를 통해 배제할 수 있어야 하 며 만성 과민성 폐렴의 경우 환자의 과거력과 임상경과, 세기관 지 중심성 병변, 호기(expiratory) CT 영상에서 공기가둠 등이 감 별에 도움을 줄 수 있다. 반복적인 감염과 폐첨부의 상대적인 허 혈상태로 인한 폐첨부 덮개(apical cap)의 경우와는 증상이 없고 진행하지 않는다는 점에서 감별점이 될 수 있다(2, 5).
IPPFE의 병리학적 소견은 보고된 증례마다 조금씩 차이가 있 지만 여러 증례 보고 문헌들을 모아서 분석한 Watanabe 등(4) 의 연구에서 폐엽내 콜라겐 침착(intraalveolar collagen deposi- tion)과 흉막하 탄력섬유증(subpleural elastosis) 소견이 공통적 으로 존재하였다. 그리고 폐상엽의 병변과 동반되어 보일 수 있 는 양측 하엽에 간질성 음영은 생검에서 상용 간질성 폐렴 진단되었다. 환자는 이후 IPPFE에 대한 특별한 치료는 받지 않
았으며 외래를 통하여 경과 관찰하기로 하고 퇴원하였다.
고찰
IPPFE는 Frankel 등(3)이 5명의 환자의 영상의학적, 임상적, 병리학적 소견을 통해 처음으로 기술하였으며, 주로 양측 폐 상 엽을 침범하는 특발성 간질성 폐렴의 새로운 질병으로 보고하였 다. 아직까지 명확한 병리적 영상학적 진단기준은 확립되어 있지 않다(2, 4-6). 다른 특발성 간질성 폐렴의 아형들과는 달리 폐 상엽을 주로 침범하고 만성적으로 진행하는 원인 불명의 간질성 폐렴은, 이전부터 idiopathic pulmonary upper lobe fibrosis (7), pulmonary apical fibrocystic change (8), 그리고 marked pul- monary fibrosis in the upper lung field (9) 등의 여러 질병명 으로 보고되어 왔고 대상 환자들의 조건에는 차이가 있었지만 임상적, 병리적 공통점이 많이 존재하였다(4). 그 중에서 Fran- kel 등(3)과 Amitani 등(7)에 의한 연구에서 임상적, 병리적 성 격이 잘 정리되었다. IPPFE는 만성적이고 진행성의 경과를 보이 는 점에서 기존의 다른 특발성 간질성 폐렴과 유사하나, 상엽 흉 막하에 주로 분포하고 두드러진 탄력섬유증(fibroelastosis)이 있 다는 점에서 구별된다(3, 5). 그러나 병리학적으로 국소적인 pleuroparenchymal fibroelastosis는 첨부를 포함한 폐에서 시행 되는 수술적 생검에서 흔히 볼 수 있는 비특이적 소견이므로, 주 로 상엽의 흉막하에 분포하는 콜라겐과 탄력섬유(elastic tissue) 침착을 특징으로 하는 IPPFE와는 구별되어져야 한다(10).
IPPFE의 영상의학적 소견은 단순흉부촬영상 주로 양측 폐 상부를 침범하는 흉막하 음영으로 나타나고 용적의 감소를 동
Fig. 3. Histopathologic features suggesting idiopathic pleuroparenchymal fibroelastosis, which revealed by surgical lung resection.
A. Right upper lobe lung shows dense fibrosis along the subpleura (arrow). The fibrosis extends into away from the pleura and shows perilobular distribution with alveolar septum (haematoxylin and eosin, × 2).
B. Dense elastic fibers (arrows) are irregularly scattered throughout the fibrosis on Elastic Van Geison stain (elastic Van Gieson staining, × 20).
C. Right lower lobe lung parenchyma shows typical microscopic features of idiopathic pulmonary fibrosis including subplerual fibrosis, patchy distribution, temporal heterogeneity and interstitial fibroblastic foci with microscopic honeycomb change (arrow) (haematoxylin and eosin, × 2).
D. The fibrotic area of subpleura shows small amount of deposition of elastic fiber (arrow) which is as same as normal lung pleura and parenchyma (elastic Van Gieson staining, × 20).
A B C D
Rassl D, Parfrey H, et al. Pleuroparenchymal fibroelastosis:
a spectrum of histopathological and imaging phenotypes.
Eur Respir J 2012;40:377-385
3. Frankel SK, Cool CD, Lynch DA, Brown KK. Idiopathic pleu- roparenchymal fibroelastosis: description of a novel clini- copathologic entity. Chest 2004;126:2007-2013
4. Watanabe K, Nagata N, Kitasato Y, Wakamatsu K, Na- beshima K, Harada T, et al. Rapid decrease in forced vital capacity in patients with idiopathic pulmonary upper lobe fibrosis. Respir Investig 2012;50:88-97
5. Piciucchi S, Tomassetti S, Casoni G, Sverzellati N, Carloni A, Dubini A, et al. High resolution CT and histological find- ings in idiopathic pleuroparenchymal fibroelastosis: fea- tures and differential diagnosis. Respir Res 2011;12:111 6. Becker CD, Gil J, Padilla ML. Idiopathic pleuroparenchymal
fibroelastosis: an unrecognized or misdiagnosed entity?
Mod Pathol 2008;21:784-787
7. Amitani R, Niimi A, Kuse F. [Idiopathic pulmonary upper lobe fibrosis (IPUF)]. Kokyu 1992;11:693-699
8. Repo UK, Kentala E, Koistinen J, Lehtipuu AL, Miettinen A, Pyrhönen S, et al. Pulmonary apical fibrocystic disease. A serologic study. Eur J Respir Dis 1981;62:46-55
9. Shiota S, Shimizu K, Suzuki M, Nakaya Y, Sakamoto K, Iwase A, et al. [Seven cases of marked pulmonary fibrosis in the upper lobe]. Nihon Kokyuki Gakkai Zasshi 1999;37:87-96 10. Ryerson CJ, Collard HR. Update on the diagnosis and clas-
sification of ILD. Curr Opin Pulm Med 2013;19:453-459 절반의 환자에서 동반된 감염이 있었던 점에서 감염에 의한 염
증과 섬유화가 연관성이 있을 수 있다(2, 4). 그리고 일부의 환 자들에서 자가면역항체가 발견되어 자가면역질환에 의한 가능 성을 생각해 볼 수 있고 가족력을 보이는 보고에서 유전적 소인 도 역할을 하는 것으로 추측된다(2). 환자의 60%에서 진행성 경과를 보이며, 영상의학적으로 이상을 보이지만 증상이 없는 무증상기(subclinical period)가 있을 수 있지만, 증상이 시작되 면 급격히 호흡기능이 떨어진다는 보고도 있다(2, 4, 6). 스테 로이드와 면역억제제, 항섬유화 제재, 성장전환인자 알파 억제 제(transforming growth factor-αinhibitor) 등이 치료에 이용 되고 있으나 아직 효과적인 치료법은 없으며 폐이식도 고려될 수 있다(2, 6).
IPPFE는 현재까지 드물게 증례들이 보고되어 있는 정도이고 따라서 이 질병에 대한 전반적인 이해가 낮은 상태로 진단에서 간과되었거나 가능성이 있다(6). 특발성 간질성 폐렴은 여러 전 문분야적 접근(multidisciplinary approach)이 중요한 영역으로 특히 영상의학적 진단이 결정적 역할을 하는 질환이다(1, 2, 4).
최근에 소개되어지는 매우 드문 형태의 특발성 간질성 폐렴인 IPPFE의 진단에 있어 영상의학적 소견의 이해 및 다른 간질성 폐렴과의 특징적인 차이에 대한 이해와 적용이 필요하겠다.
참고문헌
1. Travis WD, Costabel U, Hansell DM, King TE Jr, Lynch DA, Nicholson AG, et al. An official American Thoracic Society/
European Respiratory Society statement: update of the international multidisciplinary classification of the idio- pathic interstitial pneumonias. Am J Respir Crit Care Med
드문 간질성 폐렴인 Idiopathic Pleuroparenchymal Fibroelastosis: 증례 보고
1박종천
1,2· 채은진
1· 송준선
3Idiopathic pleuroparenchymal fibroelastosis (이하 IPPFE)는 최근 기술되기 시작한 상부 폐의 흉막 하에 주로 발생하는, 매우 드문 특발성 간질성 폐 질환이다. IPPFE는 다른 특발성 간질성 폐 질환들과 달리 상엽, 그 중에서도 주로 흉막 하에 병변이 위치하며 병리학적으로는 탄력섬유증(fibroelastosis)을 보인다는 점이 특징적이다. 저자들은 수술적 생검을 통해 IPPFE로 확진된 환자에서 컴퓨터 단층촬영(computed tomography)을 통한 8년간의 장기적 추적관찰로 질병의 형태학적 진행을 잘 보여주는 증례를 경험하여, 이 환자의 임상적, 영상 의학적, 병리학적 소견을 보고하고자 한다.
울산대학교 의과대학 서울아산병원 1영상의학과 영상의학연구소, 3병리과, 2대구가톨릭대학교 의과대학 영상의학교실