Vol. 18, No. 4, September, 2006
대퇴 전자하 골절의 수술적 치료
이 상 홍
조선대학교 의과대학 정형외과학교실
서 론
대퇴골 전자하부 골절은 교통사고의 증가와 평균수명의 연장으로 인한 노령 인구의 증가로 점차 발생 빈도가 증가 하는 추세에 있다11,13,17). 전자하 골절은 전체 고관절 골절 의 10-34% 정도를 차지하며 약 1/3은 고 에너지 손상에 의해 젊은층에서 발생하고 나머지는 저에너지손상에 의해 고령의 골다공증이 심한 환자에게 발생한다. 다른 고관절 부 골절에 비해 젊은 연령군에서 높은 빈도를 보이고 있는 데 이는 골절의 원인 중 교통사고나 실족, 추락사고등이 대부분으로 활동력이 가장 높은 층과 밀접한 연관관계가 있다고 보여진다.
해부학적, 생역학적 특징
대퇴골에서 전자하부는 소전자로부터 대퇴골 간부의 상 부 1/3부위를 말한다. 일반적으로 소전자로부터 5 cm 하 방의 근위 대퇴골 부위를 전자하부라고 지칭하며 소전자 상단에서부터 원위 7.5 cm 하방에 이르는 부위를 이르기 도 한다. 이 부위는 두꺼운 피질골로 이루어진 높은 생역 학적 압력을 받는 부위로 Koch 등25)은 소전자 직하부의 내측과 후내측의 피질골에 1200lb/in의 압박력이 가해지 고 외측의 피질골은 1000lb/in 의 장력이 가해진다고 하였 다(Fig. 1). 이러한 생역학적 특징으로 인하여 골절은 내 측으로는 분쇄를 동반하고 골절부는 내반되려고 하는 굽힘 모멘트가 발생한다.
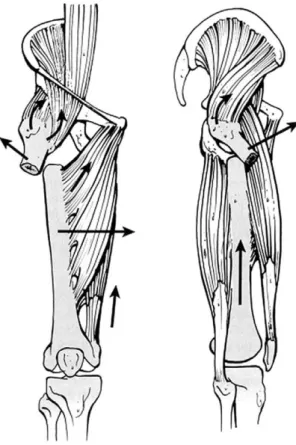
전자하부는 골절시 주위 근육에 의해 골절편이 다양하게 전위되는데 소둔근과 중둔근은 대전자부에 붙어 근위 골편 을 당겨 외전시키고 장요근은 소전자에 붙어 근위골편을 굴곡, 외회전 시킨다. 골절은 특징적으로 원위 골편이 내 반형태를 이루게 되는데 이는 내전근과 슬괵근의 부착으로
발생되며 결과적으로 골절부의 단축을 야기한다. 단외회전 근들(piriformis, superior and inferior gammellus, obturator internus)은 대부분의 전자하 골절에서 근위 골절편을 외회전 시키게 된다(Fig. 2). 이러한 근육들의 작용은 원위 골절편을 근위 골절편에 정복하려고 할 때 패 쇄적 정복술을 어렵게 하며 치료에 사용되는 내고정물도 이러한 해부학적, 생역학적 특징을 고려해야 한다.
분 류
1949년 Boyd and Griffin9)은 전자간 골절의 변형으로 서 전자하 골절에 대해 처음으로 기술하였으며 이 골절은 수술적 치료 결과가 좋지 않다고 하였다. 초기에 Fielding and Magliato17)는 이 골절을 소전자에서부터 골절부위까 지의 거리를 바탕으로 분류하였지만 이는 골절의 연장이나 분쇄정도는 반영하지 못하였다. Zickel67)은 이 골절을 high transverse, low transverse, short oblique, long oblique로 나누어 분류하였으며 oblique 골절은 분 쇄와 비분쇄로 추가 분류하였다. 하지만 이 분류 방법 역 시 골절 양상은 잘 설명할 수 있으나 현재의 내고정장치에 적합한 치료법을 제시하지 못하였다.
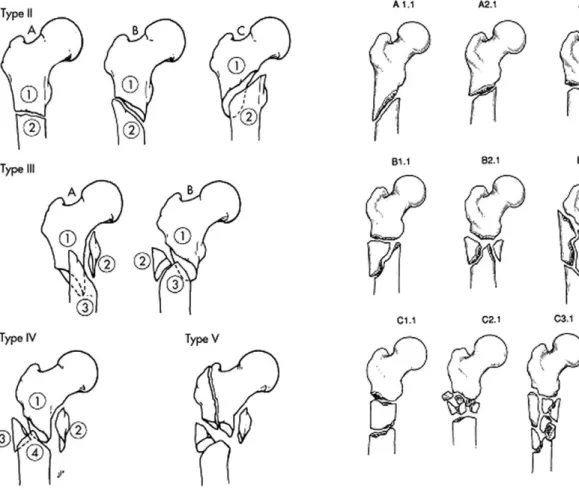
Seinsheimer51) 분류는 큰 골절 편의 수와 골절 선의 위 치 및 모양에 따라 5형으로 분류하였는데 이는 골절로 인 한 내측 피질골의 소실에 따라 고정물 실패가 좌우되기 때 문에 예후평가에 용의하다(Fig. 3). AO 분류는 A,B,C 형의 골절로 분류하는데 A형은 소전자 직하방의 단순골 절, B형은 내측 또는 외측에 쐐기형의 골편이 있는 경우, C형은 분절 골절 또는 심한 분쇄가 있는 경우이다. 각각의 골절은 추가로 spiral, oblique, transverse로 나누어진 다. 이 역시 골절의 심한 정도에 따라 분류하여 예후 예측 에 도움이 된다(Fig. 4).
Russel과 Taylor46) 분류는 소 전자의 골절여부와 골절 선이 뒤로 연장되어 이상 와(piriformis fossa)를 침범하 는 대 전자 골절의 유무를 기준으로 하여 재건 금속정을 사용할 수 있는지에 중점을 두고 분류하였다.
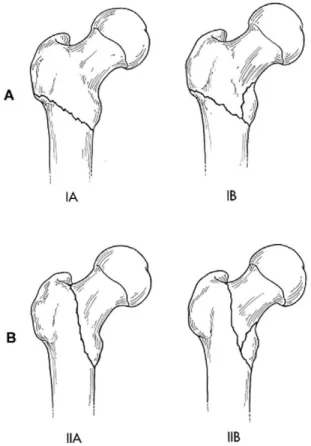
제I형은 이상 와를 침범하지 않은 골절로 IA 형은 분쇄 골절로 골절선이 소 전자 하부부터 대퇴 협부(femoral
※ 통신저자 : 이 상 홍
광주광역시 동구 서석동 558 조선대학교 의과대학 정형외과학교실 Tel: 82-62-220-3147
Fax: 82-62-226-3379 E-mail: [email protected]
isthmus)에 이르는 것, IB 형은 골절선과 분쇄 골절이 소 전자를 침범하여 협부에 이르는 골절, 제II형은 골절선이 근위부로 대 전자를 통과하여 이상 와를 침범하는 골절로 IIA형은 골절선이 소 전자부터 협부에 이르며 소 전자에 골절이 없는 것, IIB형은 골절선이 이상 와를 침범하고 대 퇴골 내측 피질 골에도 분쇄골절이 있어 소 전자를 침범하 는 것이다(Fig. 5). 최근의 금속정은 이상 와가 기시점이 아닌 대전자부인 경우도 있는데 이런 경우 이 분류법의 효 용성이 떨어진다. 하지만 이 분류법과 seinsheimer의 분 류법은 골절을 보다 자세하게 표현할 수 있고 향후 처치의 난이도를 어느정도 예측가능하게 하여 현재 널리 사용되고 있다.
치 료
1. 보존적 치료
내과적으로 수술을 할 수 없는 환자에게 적용되고 일반 적으로는 시행하지 않으며 단축과 변형 때문에 좋지 않은 결과를 보일 가능성이 크다. 즉 전자하 골절의 근위 골편
은 부착된 근육의 수축으로 외전, 굴곡 및 외 회전, 대퇴 골간은 내전 및 단축되어 보존적 요법으로 치료가 어렵다.
2. 수술적 치료
골절 자체가 다리의 단축과 내측 각형성을 발생시키기 때문에 부적절한 치료시 외전근의 단축으로 인한 합병증을 야기시킬 수 있으므로 수술적 치료가 원칙이며 치료의 목 표는 정상 길이와 각을 유지하여 외전근에 적당한 장력을 유지시키는 것이다. 또 전자하부의 해부학 및 생역학적인 특징을 고려한 충분한 강도와 적절한 특징을 가진 내고정 물을 사용하여야 하며 사용되는 내고정물은 크게 골수강내 고정과 골수강외 고정으로 구별된다. 현재의 골수강내 고 정은 1세대 교합성 금속정과 2세대 교합성 금속정 (reconstruction nail 및 gamma nail과 같은 nail lag screw device를 포함하는 cephalomedullary nail)이 있 다. 골수강외 고정의 종류에는 95도 condylar or angled blade plate, 95도 dynamic condylar screw, sliding or compression hip screw등이 있으며 Medoff sliding plate나 trochanteric stabilizing plate같은 보조 고정
Fig. 1. Koch’s diagram showing the compression stress on the medial side and the tension stress on the lateral side of the proximal femur.
Fig. 2. Deforming forces about a subtrochanteric femur fracture.
물 등이 있다.
고정물의 생역학을 보면 골수강내 고정장치는 골수강외 고정장치에 비해 두 가지 생역학적 장점이있다. 첫 번째는 골수강내 금속정의 간부 고정은 외측에 대는 금속판에 비 하여 고관절의 회전의 중심에 더 가까이 위치한다는 것이 다. 이는 더 짧은 지렛대 역할을 하게 됨으로써 굽힘모멘 트가 작아져 역학적인 실패의 가능성을 줄인다. 두 번째 장점은 골수강내 금속정이 load sharing device인데 비하 여 골수강외 장치는 load bearing device라는 점이다. 하 지만 이는 안정적인 골절인 경우만 해당된다. 심한 분쇄를 동반한 불안정골절에서는 하중이 결핍부위를 통과하여 골 수강내 고정물과 골수강외 고정물에서 모두 원위부에 하중 을 전달하게 되며34,46), 다른 생역학적인 것을 비교하자면 모두 비슷한 굴곡강도를 가지고 있으며 골수강내정이 골수 강외 장치 보다 염전력에 약하다58). 골수강내정은 더 높은 정도의 굴곡, 압박력을 견딜 수 있어 불안정 전자하 골절 에서 135도 또는 95도 screw or plate에 비하여 더 견고 한 고정이 가능하게 한다15,34). 그 밖에 골수강내 장치의 다 른 장점들로는 원위골편이 내측으로 이용하는 것을 막아주 는 것과 골두와 경부의 골편이 단축되는 것을 막아주는 것 등이 있다40).
1) 골수강내 고정물
전자하 골절을 치료하는데 있어 골수강내 금속정의 사용 은 생역학적인 발전과 골절에 대한 비개방성 접근법 때문 에 정형외과 의사들이 점차 선호하는 방법이 되고 있다.
1967년에 최초로 Zickel68)이 전자하 골절에 골수강내 금속 정을 사용하여 성공적으로 보고하였고 Brien 등11)은 교합 성 금속정을 Zickel nail 과 95도 condylar blade plate 와 비교하여 교합성 금속정이 전자하 골절을 치료하는데 있어 가장 이상적인 고정물로 소개하였다. 하지만 금속정 이 생역학적으로 비교적 이상적인 고정물임에도 불구하고 여러 합병증들(malrotation, 부정유합, 불유합, 재골절) 등이 보고되고 있고 그 세심한 술기가 필요하므로 이를 복 잡한 골절에 쉽게 사용할 수 있다고 간과해서는 안된다.
① 제 1세대 교합성 골수강내 금속정
소전자의 골절이 없을 때 사용할 수 있으므로 자주 사용 되는 고정물은 아니다. 제 1세대 금속정은 근위부의 interlocking screw를 근위부에서 원위부를 향해 고정하 게 되어 있으며 나사못은 소전자 부위의 피질골에 고정되 므로 만약 소전자가 골절되어 있다면 근위부의 고정이 어
Fig. 3. Seinsheimer classification Fig. 4. AO-ASIF classification
렵다. 그러므로 이상 와와 소전자가 골절되지 않은 Russell-Taylor IA형의 골절에서 사용할 수 있다46).
② 제 2세대 교합성 골수강내 금속정
제2세대 또는 cephalomedullary nail은 제 1세대 금 속정과 비교하여 근위부의 interlocking screw의 위치와 방향에 차이가 있다. 이 나사못은 원위부에서 근위부를 향 하게 되며 대퇴골 근위부의 외측 피질에서 대퇴 경부 및 골두를 향하여 고정된다. 이는 소전자가 골절되었다 하더 라도 사용가능하기 때문에 제 1세대 금속정에 비하여 전자 하 골절을 치료하는데 더 광범위하게 사용되고 있다. 이 금속정은 Russell과Taylor IB형의 골절에서 사용할 수 있 다. Russell과 Taylor 등46)은 제 2형의 골절에서는 이상 와(piriformis fossa)가 손상되기 때문에 골수강내 금속정 을 사용할 수 없다고 하였으나 현재는 대전자에서 삽입이
가능한 금속정으로 제 2형 골절 같이 이상 와가 손상되어 있는 경우에도 사용이 가능하다.
Cephalomedullary nail의 사용은 기술적으로 어렵고 금속정의 삽입 위치가 정확히 위치해야 근위부의 interlocking screw가 대퇴 골두 및 경부에 안정적으로 삽 입될 수 있기 때문에 정확한 술자의 숙련도가 요구된다23).
③ Nail-Lag Screw Devices
Cephalomedullary nail의 한 종류로 제 2세대 금속정 의 interlocking 개념과 closed nailing의 개념 그리고 sliding hip screw 의 lag screw 개념을 혼합하여 제작 되었다. 가장 초기에 제작된 nail-lag screw 기구는 Gamma nail로 초기에 디자인의 문제로 금속정의 끝부분 에 발생하는 대퇴간부 골절 및 외측 피질의 골절등의 합병 증1,4,10,12,42,44,60)
이 발생되었으나 이러한 디자인의 보완으로 여러 형태의 고정물이 소개되고 있으며 합병증의 빈도도 감소되고 있다50).
2) 골수강외 고정물
① 활강 압박고 나사(Sliding Hip Screw)
전자하 골절을 포함하여 고관절 골절에서 135도 활강 압 박고 나사는 자주 사용되어지는 기구로 장점은 친숙하다는 것이지만 전자하 골절에 쓰일 경우 단점이 있다. 저에너지 손상 환자에서는 적당한 고정을 할 수 있고 결과도 비교적 좋지만 고에너지 또는 불안정한 전자하 골절에서는 실패율 이 5~20%로 나사못의 골두내 돌출, 원위 간부의 내측 이 동, 단축, 내측 각형성등 합병증이 보고되었다51).
그 외 근위 전자하 골절의 경우 골절 부위가 lag screw 의 삽입위치와 비슷하기 때문에 견고함을 더하기 위해 side plate를 통해 근위 골편에 추가로 나사를 박는 것이 어려워 안정성에 문제가 될 수 있으며 심한 분쇄를 동반한 원위 전자하 골절에서는 side plate를 통과하는 나사가 골 절부의 원위부와 근위부에 위치하여 압박을 막기 때문에 불유합을 발생시킬 수 있다47,48,67). 또한 더 원위부의 골절 에서는 더 긴 side plate를 사용하기위해 절개부가 더 넓 어질 수 있어 연부조직 손상이 많아진다. 하지만 안정적 골절에서 활강 압박고 나사의 사용은 비교적 만족할 만한 결과를 보였으며 전자하 골절에서 제한된 적응증을 가지고 사용한다면 합병증을 줄일 수 있다.
Table 1. Treatment recommendations based on Russell-Taylor classification of subtrochanteric fractures.
ⅠA Piriformis fossa and lesser trochanter intact Standard interlocking IM nail
ⅠB Piriformis fossa intact, lesser trochanter fractured Reconstruction IM nail
ⅡA Piriformis fossa fractured, lesser trochanter intact Sliding hip screw or reconstruction IM nail
ⅡB Piriformis fossa and lesser trochanter both fractured Sliding hip screw with bone graft or reconstruction IM nail Fig. 5. Russell-Taylor classification
전자하 골절을 활강 압박고 나사를 이용하여 치료하는 방법은 Medoff sliding plate13,32,35,63)
나 Trochanteric stabilizing plate (TSP)32,33)를 이용하여 더 견고하게 고 정할 수 있다. Medoff sliding plate는 간부의 축을 따라 활강이 가능하게 만든 기구로 이차적으로는 대퇴 경부를 따라 활강이 이뤄져 load sharing이 가능하며 비교적 좋 은 결과를 보였다32,63). 하지만 골절부가 소전자로부터 5 cm이하까지 연장된 골절의 경우 나사가 근위 골편에 위치 하여 금속판의 활강이 불가능하게 되므로 사용의 제약이 있다. Trochanteric stabilizing plate는 side plate에 더하여 대전자의 buttress plate로 작용함으로써 과도한 골절부 감입이나 간부가 내측 이동하는 것을 억제한다33). 이 두가지의 간단한 방법을 추가로 사용하므로서 활강 압 박고 나사의 적응증이 더 다양해질 수 있겠다.
② Condylar Blade Plate
High angled hip screw의 초기 실패로 condylar blade plate가 전자하 골절의 치료를 위해 소개되었다.
Blade plate의 장점은 금속판의 강도가 높다는 점과 뼈에 더 견고히 부착이 가능하여 비교적 단단한 고정이 가능하 다는 것이다24,52,65). 하지만 blade plate를 이용한 고정은 상당한 연부조직의 절개를 필요로 하고 blade가 대퇴 골두 를 통하여 정확하게 삽입되어야 하는 기술적인 어려움이 있다는 단점이 있다11,51,35). 합병증으로는 대퇴경부 골절, malreduction, implant failure 등이 있으며 이러한 문 제점과 절개시 발생하는 상당량의 출혈로 인해 현재 고령 에서의 condylar blade plate의 사용은 거의 추천되고 있 지 않다24).
③ Dynamic Condylar Screw
blade plate의 대용으로 대퇴골의 전자하 골절이나 과 상골절을 치료하기 위해 개발되었다47,49). DCS의 장점은 3 차원적으로 고정이 필요한 condylar blade plate보다 기 술적으로 시술하기가 편하며 나사의 삽입 부분이 보다 근 위부에 위치하여 2개 이상의 나사고정이 가능하고 특히 calcar의 강한 부위에 고정이 가능하다는 것이다47,66). 그리 고 경피적으로 삽입이 가능하여 비침습적인 수술이 가능하 다. 하지만 금속판의 강도와 나사의 고정력등이 문제시 되 어 실패율이 20~25%정도 보고되고 있으며 현재는 제한 되어 사용되고 있다30).
술후 처치
수술 후에 환자에게 체중부하를 억제하는 것은 결국 환 자의 보행 능력을 감소시키고 하지의 근력약화와 골절부의 혈행 감소를 야기하여 좋지 않은 결과를 나타낼 수 있다.
그러므로 수술의 목적은 충분히 견고한 고정물을 사용하여
가능한 체중부하를 최대한 빨리 하게끔 하는 것이다. 심한 분쇄가 있거나 불안정한 전자하 골절에서 골수강외 고정장 치를 사용하는 것은 Medoff sliding plate를 제외하고는 조기 보행이 어려워 골수강내 고정장치를 이용 후 빠른 전 체중 부하를 추천하고 있다8,16,22,32,39,43,54,60,63)
.
요 약
고에너지 외력에 의해 발생한 대퇴골 전자하부 골절은 비교적 드문 골절로 생역학적, 해부학적 특징으로 인해 분 쇄와 전위가 심하며 적절히 치료하기 위해서는 특징을 잘 이해하고 적절한 고정물의 선택과 세심한 수술술기를 사용 하는 것이 필요하다. 고정물의 선택에 있어 서 이상 와 (piriformis fossa)의 침범 여부에 따른 Russell과 Taylor의 분류에 기초를 둔 치료방법이 추천되는데 (Table 1), 보다 좋은 결과를 얻기 위해서는 술 전 골절에 대한 정확한 분석과 숙련된 술자의 능력이 필수적이다.
REFERENCES
11) Albareda J, Laderiga A, Palanca D, et al : Complications and technical problems with the Gamma nail. Int Orthop, 20:47-50, 1996.
12) Alcivar E: A new method of external fixation for proximal fractures of the femur. Injury, 32(suppl 4):SD107-114, 2001.
13) Alvarez JR, Gonzolez RC, Aranda RL, et al : Indications for use of the long Gamma nail. Clin Orthop, 350:62-66, 1998.
14) Aune AK, Ekeland A, Odegaard B, et al: Gamma nail vs compression screw for trochanteric femoral fractures.
15 reoperations in a prospective, randomized study of 378 patients. Acta Orthop Scand, 65:127-130, 1994.
15) Barquet A, Francescoli L, Rienzi D, et al : Intertrochanteric-subtrochanteric fractures: Treatment with the long Gamma nail. J Orthop Trauma, 14:324-328, 2000.
16) Bartucci EJ, Gonzalez MH, Cooperman DR, et al: The effect of adjunctive methylmethacrylate on failures of fixation and function in patients with intertrochanteric fractures and osteoporosis. J Bone Joint Surg, 67-A:
1094-1107, 1985.
17) Baumgaertner MR, Curtin SL, Lindskog DM, et al:
The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg, 77-A:1058-1064, 1995.
18) Bellabarba C, Herscovici D Jr and Ricci WM : Percutaneous treatment of peritrochanteric fractures using the Gamma nail. Clin Orthop, 375:30-42, 2000.
19) Boyd HB and Griffin LL: Classification and treatment of trochanteric fractures. Arch Surg, 58:853-866, 1949.
10) Bridle SH, Patel AD, Bircher M, et al: Fixation of
intertrochanteric fractures of the femur. A randomised prospective comparison of the Gamma nail and the dynamic hip screw. J Bone Joint Surg, 73-B:330-334, 1991.
11) Brien WW, Wiss DA, Becker V Jr, et al : Subtrochanteric femur fractures: a comparison of the Zickel nail, 95 degrees blade plate, and interlocking nail.
J Orthop Trauma, 5:458-464, 1991.
12) Butt MS, Krikler SJ, Nafie S, et al: Comparison of dynamic hip screw and gamma nail: a prospective, randomized, controlled trial. Injury, 26:615-618, 1995.
13) Ceder L, Lunsjo K, Olsson O, et al: Different ways to treat subtrochanteric fractures with the Medoff sliding plate. Clin Orthop, 348: 101-106, 1998.
14) Choueka J, Koval KJ, Kummer FJ, et al: Cement augmentation of intertrochanteric fracture fixation: a cadaver comparison of 2 techniques. Acta Orthop Scand, 67:153-157, 1996.
15) Curtis MJ, Jinnah RH, Wilson V, et al: Proximal femoral fractures: a biomechanical study to compare intramedullary and extramedullary fixation. Injury, 25:
99-104, 1994.
16) Edwards SA, Pandit HG and Clarke HJ: The long Gamma nail: a DGH experience. Injury, 31:701-709, 2000.
17) Fielding JW and Magliato HJ: Subtrochanteric fractures. Surg Gynecol Obstet, 122: 555-560, 1966.
18) Orthopaedic Trauma Association Committee for Coding and Classification Fracture and dislocation compendium.
J Orthop Trauma, 10(suppl 1):36-40, 1996.
19) Goldhagen PR, O’Connor DR, Schwarze D, et al: A prospective comparative study of the compression hip screw and the Gamma nail. J Orthop Trauma, 8:367-372, 1994.
20) Harrington KD: The use of methylmethacrylate as an adjunct in the internal fixation of unstable comminuted intertrochanteric fractures in osteoporotic patients. J Bone Joint Surg, 57-A:744-750, 1975.
21) Haynes RC, Poll RG, Miles AW, et al: Failure of femoral head fixation: a cadaveric analysis of lag screw cut-out with the Gamma locking nail and AO dynamic hip screw. Injury, 28:337-341, 1997.
22) Hotz TK, Zellweger R and Kach KP: Minimal invasive treatment of proximal femur fractures with the long Gamma nail: indication, technique, results. J Trauma, 47:
942-945, 1999.
23) Kang S, McAndrew MP and Johnson KD : The reconstruction locked nail for complex fractures of the proximal femur. J Orthop Trauma, 9:453-463, 1995.
24) Kinast C, Bolhofner BR, Mast JW, et al : Subtrochanteric fractures of the femur. Results of treatment with the 95 degrees condylar blade-plate. Clin Orthop 238:122-130, 1989.
25) Koch JC: The laws of bone architecture. Am J Anat, 21:
243, 1917.
26) Kourtzis N, Pafilas D and Kasimatis G: Management of pertrochanteric fractures in the elderly patients with an external fixation. Injury, 32(suppl 4): SD115-128, 2001.
27) Koval KJ, Sala DA, Kummer FJ, et al: Postoperative weightbearing after a fracture of the femoral neck or an intertrochanteric fracture. J Bone Joint Surg, 80-A:352- 356, 1998.
28) Krettek C, Schandelmaier P, Miclau T, et al: Minimally invasive percutaneous plate osteosynthesis (MIPPO) using the DCS in proximal and distal femoral fractures. Injury, 28(suppl 1):A20-30, 1997.
29) Kukla C, Heinz T, Gaebler C, et al: The standard Gamma nail: a critical analysis of 1,000 cases. J Trauma, 51: 77-83, 2001.
30) Kulkarni SS and Moran CG: Results of dynamic condylar screw for subtrochanteric fractures. Injury, 34:
117-122, 2003.
31) Kyle RF, Cabanela ME, Russell TA, et al: Fractures of the proximal part of the femur. Instr Course Lect, 44:227- 253, 1995.
32) Lunsjo K, Ceder L, Tidermark J, et al: Extramedullary fixation of 107 subtrochanteric fractures: a randomized multicenter trial of the Medoff sliding plate versus 3 other screw-plate systems. Acta Orthop Scand, 70:459-466, 1999.
33) Madsen JE, Naess L, Aune AK, et al: Dynamic hip screw with trochanteric stabilizing plate in the treatment of unstable proximal femoral fractures: a comparative study with the Gamma nail and compression hip screw. J Orthop Trauma, 12:241-248, 1998.
34) Mahomed N, Harrington I, Kellam J, et al : Biomechanical analysis of the Gamma nail and sliding hip screw. Clin Orthop, 304:280-288, 1994.
35) Medoff RJ and Maes K: A new device for the fixation of unstable pertrochanteric fractures of the hip. J Bone Joint Surg, 73-A:1192-1199, 1991.
36) Michelson JD, Myers A, Jinnah R, et al: Epidemiology of hip fractures among the elderly. Risk factors for fracture type. Clin Orthop, 311:129-135, 1995.
37) Ozdemir H, Dabak TK, Urguden M, et al: A different treatment modality for trochanteric fractures of the femur in surgical highrisk patients: a clinical study of 44 patients with 21-month followup. Arch Orthop Trauma Surg, 123:538-543, 2003.
38) Pai CH: Dynamic condylar screw for subtrochanteric femur fractures with greater trochanteric extension. J Orthop Trauma, 10:317-322, 1996.
39) Pakuts AJ: Unstable subtrochanteric fractures-Gamma nail versus dynamic condylar screw. Int Orthop, 28:21-24, 2004.
40) Parker M and Handoll H: Gamma and other cephalocondylic intramedullary nails versus extramedullary implants for extracapsular hip fractures. Cochrane Database Syst Rev, 1:CD000093, 2004.
41) Parker MJ, Dutta BK, Sivaji C, et al: Subtrochanteric
fractures of the femur. Injury, 28:91-95, 1997.
42) Parker MJ and Pryor GA: Gamma versus DHS nailing for extracapsular femoral fractures. Meta-analysis of ten randomised trials. Int Orthop, 20:163-168, 1996.
43) Pervez H and Parker MJ: Results of the long Gamma nail for complex proximal femoral fractures. Injury, 32:
704-707, 2001.
44) Radford PJ, Needoff M and Webb JK: A prospective randomised comparison of the dynamic hip screw and the Gamma locking nail. J Bone Joint Surg, 75-B:789-793, 1993.
45) Rantanen J and Aro HT: Intramedullary fixation of high subtrochanteric femoral fractures: a study comparing two implant designs, the Gamma nail and the intramedullary hip screw. J Orthop Trauma, 12:249-252, 1998.
46) Russell TA and Taylor JC: Subtrochanteric fractures of the femur. In: Browner BD, Jupiter JB, Levine AM, et al., eds. Skeletal Trauma Philadelphia: WB Saunders Co:
1485-1524, 1992.
47) Sanders R and Regazzoni P: Treatment of subtrochanteric femur fractures using the dynamic condylar screw. J Orthop Trauma, 3:206-213, 1989.
48) Schatzker J: Subtrochanteric fractures of the femur. In:
Schatzker J, Tile M, eds. The Rationale of Operative Fracture Care. New York, Springer-Verlag:349-366, 1996.
49) Schatzker J, Mahomed N, Schiffman K, et al: Dynamic condylar screw: a new device. A preliminary report. J Orthop Trauma, 3:124-132, 1989.
50) Schipper IB, Steyerberg EW, Castelein RM, et al:
Treatment of unstable trochanteric fractures. Randomised comparison of the Gamma nail and the proximal femoral nail. J Bone Joint Surg, 86-B:86-94, 2004.
51) Seinsheimer F: Subtrochanteric fractures of the femur. J Bone Joint Surg, 60-A:300-306, 1978.
52) Senter B, Kendig R and Savoie F : Operative stabilization of subtrochanteric fractures of the femur. J Orthop Trauma, 4: 399-405, 1990.
53) Siebenrock KA, Muller U and Ganz R: Indirect reduction with a condylar blade plate for osteosynthesis of subtrochanteric femoral fractures. Injury, 29(suppl 3):
C7-15, 1998.
54) Stapert JW, Geesing CL, Jacobs PB, et al: First experience and complications with the long Gamma nail. J Trauma, 34:394-400, 1993.
55) Szpalski M, Descamps PY, Hayez JP, et al: Prevention of hip lag screw cut-out by cement augmentation:
description of a new technique and preliminary clinical results. J Orthop Trauma, 18:34-40, 2004.
56) Szpalski M and Gunzburg R: Prevention of hip lag screw cut-out in osteoporotic patients: rationale and review of the literature. Bull Hosp Jt Dis, 60:84-88, 2001.
57) Taglang G, Grosse A, Halder SC, et al : The Trochanteric Gamma Locking Nail (Technique Manual).
Rutherford, NJ: Stryker Corp, 2003.
58) Tencer AF, Johnson KD, Johnston DW, et al : A biomechanical comparison of various methods of stabilization of subtrochanteric fractures of the femur. J Orthop Res, 2:297-305, 1984.
59) Vaidya SV, Dholakia DB and Chatterjee A: The use of a dynamic condylar screw and biological reduction techniques for subtrochanteric femur fracture. Injury, 34:
123-128, 2003.
60) Valverde JA, Alonso MG, Porro JG, et al: Use of the Gamma nail in the treatment of fractures of the proximal femur. Clin Orthop, 350:56-61, 1998.
61) Velasco RU and Comfort TH: Analysis of treatment problems in subtrochanteric fractures of the femur. J Trauma, 18:513-523, 1978.
62) Vossinakis IC and Badras LS: The external fixator compared with the sliding hip screw for pertrochanteric fractures of the femur. J Bone Joint Surg, 84-B:23-29, 2002.
63) Wachtl SW, Gautier E and Jakob RP: Low reoperation rate with the Medoff sliding plate: 1 technical failure in 63 trochanteric hip fractures. Acta Orthop Scand, 72:141- 145, 2001.
64) Waddell JP: Alternatives in the management of subtrochanteric fractures. Instr Course Lect, 33: 222-229, 1984.
65) Waddell JP: Subtrochanteric fractures of the femur: a review of 130 patients. J Trauma, 19:582-592, 1979.
66) Warwick DJ, Crichlow TP, Langkamer VG, et al: The dynamic condylar screw in the management of subtrochanteric fractures of the femur. Injury, 26:241- 244, 1995.
67) Zickel RE: An intramedullary fixation device for the proximal part of the femur. Nine years’ experience. J Bone Joint Surg, 58-A:866-872, 1976.
68) Zickel RE: A new fixation device for subtrochanteric fractures of the femur: a preliminary report. Clin Orthop, 54:115-123, 1967.
69) Zickel RE: Subtrochanteric femoral fractures. Orthop Clin North Am, 11:555-568, 1980.