大짧放射짧짧學 f캉응훈‘ 第 22 卷 第5 號 pp. 832 - 835, 1986 Journal of Korean Radiological Society, Vo1. 22, No.5, 1986
後題體의 훌훌性 빼모管睡 1 例
천북대 학교 의 과대학 방사선과학교실 -“‘-ι 며ζ그
희 • 최
기 철전북대학교 의과대학외과학교살
김 재 천
국군논산영원 내과 임 창 。ε크걱
- Abstract-
A Case of Retroperitoneal Cystic Lymphangioma
Myung Hee Sohn
,
M.D. and Ki Chul Choi,
M.D.Oepartment of Radiologκ Col!ege of Medicine, Chonbuk National University
Jae Chun Kim
,
M.DOepartment of Ceneral Surgery, Col!ege of Medicine, Chonbuk National University
Chang Yeol Yim
,
M.D.Oepartment of Intemal Medicine, Nonsan Military Hospital
Retroperitoneal cystic Iymphangiomas are uncommon tumors usually found incidentally at surgery, autop' sy, or Iymphography. When clinically significant, they usually present early in lile as a palpable abdominal mass We discribe an unusual case 01 a six-year old boy who was operated lor a cystic Iymphangioma 01 the right axilla at the age 01 live months, and, six years later, was lound to have a retroperitoneal cystic Iymphangioma accompanied with motor weakness 01 the lower extremities
서 론
후복악의 낭성 임파판종은 임파계의 양성 냥종으로})
이 논운응 1986 년 8 월 30 일에 접수하여 1986년 9 월.JO 일에 채택되었음.
주요 발생원인이 태생기 이상으후 생각되는 회귀한 질
환이마 2 , 3)
저자들은 냥성 임파판종이 출생시부터 액와부에 존재 한 환자를 생후 5 개월째 수술치료하였는데 6 년후 다시 하지운동장애를 동반한 후복악의 낭성 임파판종이 발견 된 환자를 경험하였기에 문헌고찰과함께 보고하고자한
- 832 -
손영 회 외 • 後股陳의 꿇↑生 i#巴管6파 1例 다.
드E
=
환자 검 O곤 .6 세, 남자.
려|
주소 . 하지운동장애와 하복부 종울
과거력 : 6 년전 액와부의 냥성 임파판종 (Fig.1) 으 로수술치료 받았음.
헌병력 : 6 년천 액와부의 낭성 업파판종 수술 치료후 계속 건강하였으냐 내원 1 개월천부터 하지운동%배로 잘 얼어서지 옷하고 하복부어| 종물이 있어서 업원하였다.
이학적 소견 : 영양상태와 말육상태는비교적 양호하였 고 혈압은
120/80 mmHg .
체온은36.5 t. 맥박은 90 회/분, 호흡수는 25 회/분이었다. 두경부와 흉부소견은 특이사항 없었으며 북부소견상 좌하복부에 달갈 크기의 종물이 촉지되었는데 압통은 없었 A며 파옹은 있었다.
사지소견£로는 양하지의 운동능력이 약호벼어 기립이불 펀하였다.
검사소견 : 말초혈액 검사는 정상이었고 일반적 생화 학 검사와 소변검사소견도 모두 정상이었다.
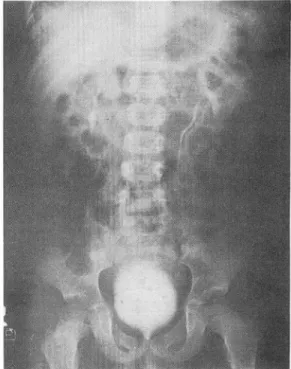
방사선학적 소견 : 흉부 X 선 사진상 특。l소견 없었으 며 북부단순촬영 사진상 조l측의 요근음영 이 불분영하게 냐타나 있어서 후복악캉의 영변을 의심할 수 있었다.경 정액신우촬영 사진에서는 죠}측 신장과 죠}측 요판의 상
Fig.
1.Chest P.A view shows a large soft tissue mass over the lateral chest wall and the right axilla.
부가 외측으로 전위돼 있었다. 우측 신장과 요판은 정 상이었마 (Fig.2). 복부전산화 단층촬영상 후복막강내 에 좌측 신장의 앞쪽에 낮은 밀도
(low density)( HU
Fig. 2. 25.minute film of urogram shows lateral displace.
ment of left kidney and the proximal portion of the left ureter
‘- 833-
- 大韓放射없醫學장誌 : 第 22卷 第5 號 1986 -
Fig. 3. Transverse computed tomography with contrast enhancement through the level of th
e kidneysshows a low-density mass (HU
=21)anterior to the laterally displaced left kidney
‘The left
‘ureter is displaced laterally.
= 21) 의 낭성 종물이 있었£며 그 종울에 의해 조넉산 장과 상부요판。l 외측으로 전위되어 있었다 (Fig.
3).
세 로재 쿠성
(sagittal reform
ation) 결파 이 종물은 조녁 신장의 상단에서 골반강까지 냐타냐 보였다(Fig.
4 ).
수술소견 및 조직소견 : 후복막강내에 18X6X7
cm
익 대 형 낭종。1 좌측 신장의 상부와 죠}측 부신에 유착 되어 있었고 닝L종은 다방성(multiloculated)
형태로- 834
표연은 배끄러웠으며 닝μ종내에 약황색의 액체가 약
100 ml
들어 있었다.조직검사상 낭성 임파판종으로확인되었다.
고 찰
임파판종은 수많은 확장된 업파판으로 쿠성된 익양성종 양인데 조직학적£혹 단순성, 해연상성, 낭포성의 3 종 으로 분류된다. 낭성 엄파판종응 단방성
(unilocular )
혹은 다방성 (multilocular) 하게 출현하며 보통 장액성 혹은 유미성의 액체가 들어 있다‘ .5)이 질환의 원인은 확실하지는 않지만 일반적으호 종 양이라기 보다 태생기 이%벼| 의해 생기는 파오종£로 간주되고 있다6) 그 외에도 임파판의 폐쇄냐 외상등에 의해 서도 생긴다고 한다7)
호발부위 를 보면 경부에 75 %(수활액 낭종). 액와부 에
20 %
정 도가 발생 하고 종격 동, 후복악, 장칸막(장간 막 낭종). 망(망낭종). 골반강, 서혜부, 바장, 뼈, 펴부 등에 나머지 5% 가 발생 한다고 한다3 , 8)증상이 있는 경우에는 보통 생후 2 년 이내에 복부의 종물로 인해서 뱅원을 찾게 되는데 3 , 5 , 8-10) 이 질환에 의해서 주위 쿠조물。 l 압박되어 요판폐쇄 8.11) 냐 조백l 쇄 4 , 12> 가 드물게 알어냐기도 한다. 본 증례에서는 출생 직후 액와부에 낭성 엄파판종이 출현하여 5 개월째 수
Fig. 4. A sagittal reformation
demonstrates a low-density mass
extending from the upper pole of
the left kidiley to the pelvic
cavíty.
- 손명 회 외 : 後JlMß흉의 캘률1生 ìM;巴짤]重 lWIJ-
술치료하여 그 후 건강하였으나 6 년후에 복부 종울파 하지의 운동장애가 발생하여 내원한 것이 특이했다.
수술전 이 질환의 진단을 위한 최근의 방법으로는 복 부초음파단층촬영, 하지 엄파판조영술, 복부전산화단층촬 영 및 경피낭종천자술 둥이 있는데 복부초음파단층촬영 소견을 보연 종물이 보이연서 내부 echo 가 냐타냐지 않A므로 낭성명변임을 알 수 있고 7 , 9 , 13) 하지임파판조 영출 소견을 보연 조영제가 낭종내로 들어가서 눔lobu-
les로 뭉쳐지는 소견을 보이기도 하며1) 대동맥 주위 임파판이냐 업파절의 전위를 보이기도 한다시 또한 낭 종과 엄파계와의 교통을 확인할 수도 있다 5) 복부전산 화단충촬영 소견은 후복막강내에 주변부가 잘 경계되며 낮응 밀도를 갖는 종물이 수위 구조물의 전위를 일으컨 다9 , 14 , 15) 경과l 낭종천자 소견을 보연 천지액내에 임파 구양 세포들이 발견되는 반면 종양세포는 보이지 않는 것이 특정이며 14) 이 방볍으로 유 0] 의 존재를확인할 수 있다.
이 질환의 치료법으로는 종전에는 수슬적 요법만을권 장했으나 3 , 16) 보촌치료도 고려해 볼 펼요가 있다고 한 다l 시
걷 로
낭성 임파판종。 l 출생시부터 액와부에 존재한 환자를 생후 5 개월째 수술치료하였는데 6 년후 다시 하지운동 징L애 를 동반한 후복악의 낭성 임파판종。l 발견된 환자
1 예를 보고하였다.
78:45-50
,
19593. Rekhi BM, Esselstyn CB jr, Levy 1, et al: Retroperitoneal cystic Iymphangioma. Report of two cases and review of the literature. C1eve C1in Q39:125-128, 1972
4. Henzel jH, Pories Wj, Burget DE, et al’ Intra-abdominal Iymphangiomata. Arch surg 93:304-308, 1966 5. Harrow BR: Retroperitoneal Iymphatic cyst (cystic Iym-
phangioma). j Urol 77:82-89, 1957
6. Willis RA: The borderland of embryology and pathology.
2nd Ed 358, Butterworth, Londoπ 1962
7. Rossi L, Mandrioli R, Rossi A, et al: Retroperitoneal cystic Iymphangioma. Br j Radiol 55:676-678, 1982
8. Singh 5, Baboo ML, Pathak IC: Cystic Iymphangioma in children. Report of 32 cases inc/uding lesions at rate sites.
Surgery 69:947-951, 1971
9‘ Leonidas jC, Brill PW, Bhan 1, et al: Cystic retroperitoneal Iymphangioma in infants and children. Radiology 127:203-208, 1978
10. Wayne ER, Burrington jD, Bailey W
c,
et al: Retroperitoneal Iymphangioma: An unusual case of the acute surgical ab- domen. j Pediatr Surg 8:831-832, 197311. Norfleet CM, Fitzsimmons LE, Smith LC, et al: Ureteral
obstruction due to retroperitoneallymphatic cyst (cystic Iymphangioma). j Urol 81:737-739, 1959
12. Barnett LA: Retroperitoneal cystic Iymphangioma. jAMA
173:1‘η 1-1116, 1960
13. Hamilton 5, M디 nerney D: Retroperitoneal angiomatous Iymphoid hamartoma demonstrated by ultrasound. Br j RadioI54:813-815, 1981
14. Sarno Rζ Carter BL, Bankoff MS: Cystic Iymphangiomas:
REFERENCES CT diagnosis and thin needle aspiration. Br j Radiol 57:424-426, 1984
1. Castellino RA, Finkelstein 5: Lymphographic demonstra- 15. Radin R, Weiner 5, Koenigsberg M, et al: Retroperitoneal tion of a retroperitoneal Iymphangioma. Radiology cystic Iymphangioma. AjR 140:733-734, 1983
115:355-356, 1975 16. Kalish M, Dorr R, Hoskins P: Retroperitoneal cystic Iym- ,2. Rauch RF: Retroperitoneal Iymphangioma. Arch Surg phangioma. Urology 6:503-506, 1975