47 REVIEW
DOI 10.4070 / kcj.2009.39.2.47
Print ISSN 1738-5520 / On-line ISSN 1738-5555 Copyright ⓒ 2009 The Korean Society of Cardiology
Transcatheter Closure of Secundum Atrial Septal Defects in the Elderly
Christian Spies, MD1 and Ziyad M. Hijazi, MD2
1The Queen’s Medical Center and Department of Medicine, University of Hawaii, Honolulu, HI,
2Rush Center for Congenital and Structural Heart Disease, Rush University Medical Center, Chicago, IL, USA
ABSTRACT
Background and Objectives: With the exception of bicuspid aortic valves, atrial septal defects (ASDs) are the most common congenital heart lesions found in adults. A mortality and morbidity benefit has clearly been de- monstrated in the treatment of this lesion in younger patients. However, the benefits of ASD closure are less well defined in the elderly. We report our experience with transcatheter ASD closure and detail its impact on functional status and right ventricular remodeling as indicators of right heart failure in patients greater than 60 years of age.
Subjects and Methods: Fifty-five patients (median age 70 years) underwent ASD closure at a single center during an eight-year period. Data were collected and analyzed retrospectively. Results: Transcatheter closure was success- ful in all patients. No major complications occurred during the periprocedural or follow-up periods. Complete defect closure was documented in 97% of patients during follow-up. All patients improved by at least one New York Heart Association (NYHA) functional class. Following ASD closure, no patient was in NYHA III or IV. The median right-ventricular end-diastolic diameter decreased from 39 mm to 26.6 mm (p<0.001). Conclusion:Atrial septal defect closure is safe and effective in elderly patients. Our data and prior published data consistently demon- strate that even patients greater than 60 years of age experience improvement in functional status and right ven- tricular remodeling. Therefore, patient age should not influence the decision of whether an ASD should be closed.
(Korean Circ J 2009;39:47-51)
KEY WORDS: Congenital heart disease; Atrial septal defect; Aged.
Introduction
With the exception of bicuspid aortic valves, atrial septal defects (ASDs) are the most common congenital heart lesions found in adults. Hemodynamically signifi- cant secundum type ASDs are now routinely treated with transcatheter closure, while primum and sinus ve- nosus defects still require surgical closure.1-4) Untreated hemodynamically significant ASDs have the potential to reduce life expectancy, decrease exercise capacity, and cause right heart failure, pulmonary arterial hyperten- sion, and atrial tachyarrhythmias. Long-term follow-up data in younger patients below the age of 25 years sug- gest that surgical ASD repair results in normal life ex- pectancy.5) Furthermore, atrial fibrillation can be pre- vented if patients undergo ASD closure before the age of 40.6) The benefits of ASD closure in elderly patients
(defined as above the age of 60 years) are less well de- fined.7) Some reports suggest that surgical ASD closure in older patients still prevents volume overload-induced heart failure and leads to reduction in pulmonary arte- rial pressure and improvement of symptoms.8) Conversely, ASD closure may be detrimental in elderly patients with advanced pulmonary arterial hypertension or left ven- tricular diastolic or systolic dysfunction who need the ASD as a “pop-off” valve.9)10)
With the advent of transcatheter ASD closure and its lower procedural morbidity compared to surgical closure, it may be reasonable to lower the threshold for ASD clo- sure in the elderly, with the hope of improving morbidity.
We report our experience with transcatheter ASD closure and detail its impact on functional status and right ven- tricular remodeling as indicators of right heart failure in patients greater than 60 years of age.
Methods
Study population
All patients above 60 years of age who underwent at-
Correspondence: Ziyad M. Hijazi, MD, Rush Center for Congenital and Struc- tural Heart Disease, Rush University Medical Center, 1653 W. Congress Parkway, Jones 770, Chicago, IL 60612, USA
Tel: 1-312-942-6800, Fax: 1-312-942-8979 E-mail: [email protected]
48·ASD Closure in the Elderly
tempted transcatheter ASD closure at a single tertiary referral center between September 1999 and March 2008 were included in the present study. Data were collected retrospectively. Indications for defect closure were a he- modynamically significant ASD with a diameter less than 40 mm and sufficient rims (>5 mm, except the anterior margin, which was allowed to be deficient). Patients un- dergoing patent foramen ovale closure and those with ASDs greater than 40 mm in diameter or partial ano- malous pulmonary venous drainage were excluded. Fifty- five patients (35 females; 20 males) with a median age of 70 years (range 61-87 years) underwent attempted device closure of their defects.
Device implantation
The Amplatzer Septal Occluder (ASO) (AGA Medical Corp., Plymouth, Minnesota, USA) was used in all pa- tients except for one. The ASO and the implantation procedure have been described previously.11)12) Between September 1999 and August 2000, all procedures were performed under general anesthesia and simultaneous fluoroscopic and transesophageal echocardiographic (TEE) guidance. After August 2000, all procedures were performed with conscious sedation and simultaneous fluoroscopy and intracardiac echocardiography (ICE).
Baseline hemodynamics were evaluated in all patients prior to closure. If the mean left atrial pressure was greater than 18 mmHg, temporary balloon occlusion of the ASD was performed for 15 minutes. During balloon occlusion, the left atrial pressure was recorded using the distal tip of the balloon catheter, after removal of the guide wire. If the mean left atrial pressure increased by more than 5 mmHg from baseline, the procedure was abandoned, and the patient received several days of an afterload-reducing agent and diuretic therapy. The pa- tient was then re-evaluated using the same balloon-oc- clusion technique. If the mean left atrial pressure did not change by more than 5 mmHg, the ASD was com- pletely closed. However, if the pressure increased by more than 5 mmHg, a fenestration was created in the device, which was then deployed according to a protocol described previously.11)13)
Three doses of cephalexin were administered in the periprocedural period. Acetylsalicylic acid (81 mg daily) was started 48 hours prior to the procedure and conti- nued for six months. Furthermore, during the last three years of our practice, clopidogrel 75 mg per day was given for the first two months following closure. Pro- phylaxis for bacterial endocarditis was recommended for six months after the procedure.
Follow-up
Physical examination, electrocardiography, and trans- thoracic echocardiography (TTE) were performed on the day following the procedure, at six months after the
procedure, and yearly thereafter to assess symptoms and to evaluate for the possibility of complications or residu- al shunt. Symptom status was classified according to the New York Heart Association (NYHA) system. Right ven- tricular end-diastolic diameter (RVEDD), defined as the largest diameter of the mid-right ventricular cavity during diastole in the short axis view, was evaluated using TTE.
Residual shunt was defined as a leak traversing the occlu- der or passing between the two discs of the ASO detected by two-dimensional color-flow Doppler. Residual shun- ting was classified according to the color-jet width descri- bed by Boutin et al.,14) trace <1 mm, small >1 mm and <2 mm, moderate >2 mm and <4 mm, and large >4 mm.
Statistics
Data are presented as medians and ranges. Differ- ences in RVEDD were compared using the Student’s t- test. The alpha level was set at 0.05. In patients with mul- tiple ASDs, the largest defect size was used for analysis.
Results
Patient characteristics
Transcatheter closure was successful in all patients.
Procedural and hemodynamic data are summarized in Table 1. Three of the 55 patients had multiple ASDs re- quiring two devices for complete closure. An ASO was used for closure in all but one patient, who was closed with a Helex occluder (W. L. Gore & Associates, Flagstaff, Arizona, USA). A fenestrated ASO was placed in two patients who had a fixed increased left atrial pressure.
The 6 mm diameter fenestration served as a protective interatrial communication, reducing left ventricular pre- load by allowing left-to-right shunting and preventing the development of pulmonary edema. Pulmonary ar- terial hypertension (defined as a mean pressure greater than 20 mmHg) was present in 23 patients (42%).
Six patients had significant pulmonary hypertension (defined as a mean pressure greater than 40 mmHg);
of these, five had complete ASD closure without any events. In one patient, a small defect was left open due to concurrent evidence of left ventricular diastolic dys- function.
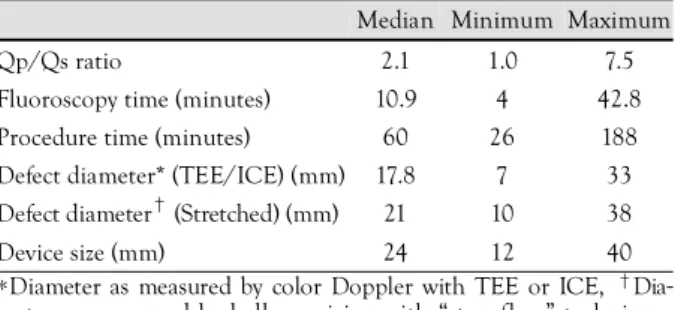
Table 1. Procedural characteristics
Median Minimum Maximum
Qp/Qs ratio 2.1 1.0 7.5
Fluoroscopy time (minutes) 10.9 4 42.8 Procedure time (minutes) 60 26 188 Defect diameter* (TEE/ICE) (mm) 17.8 7 33 Defect diameter† (Stretched) (mm) 21 10 38
Device size (mm) 24 12 40
*Diameter as measured by color Doppler with TEE or ICE, †Dia- meter as measured by balloon sizing with “stop-flow” technique.
Qp: pulmonic flow, Qs: systemic flow, TEE: transesophageal echo- cardiography, ICE: intracardiac echocardiography
Christian Spies, et al.·49
Follow-up
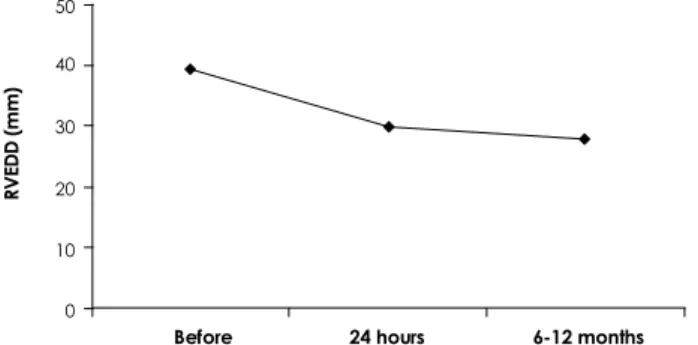
Clinical and echocardiographic follow-up information were available in 31 patients. The median follow-up du- ration was 28 months (range 6-79 months). Device clo- sure was associated with a significant decrease in the RVEDD. The median RVEDD decreased from 39 mm (range 20-55 mm) before ASD closure to 26.6 mm (range 14-38 mm) at a median interval of 6 months (p<0.001) (Fig. 1).
The majority of patients showed improvement in symptoms during follow-up (Table 2). One NYHA class III patient with a moderately large ASD and reduced left ventricular diastolic elasticity underwent successful ASD closure with a fenestrated ASO and subsequently improved by one functional class during follow-up.
However, he was admitted with acute decompensated heart failure six years after his ASD closure, secondary to severe diastolic dysfunction from his chronic hyper- tension.
Thirteen patients (24%) had atrial fibrillation or flut- ter prior to ASD closure. Three patients underwent ra- diofrequency ablation prior to ASD closure, and the other ten remained in atrial fibrillation. Only one pa- tient had new onset persistent atrial fibrillation 4 years after ASD closure.
Immediate closure was accomplished in 87% of pa- tients (46 of 53 patients). Trivial shunts were seen in three patients, and small shunts were seen in three pa- tients. A moderate shunt was seen in one patient. The two patients who received a fenestrated ASO were exclud- ed. During follow-up, complete closure was documented
in 97% of patients (32 of 33 patients). One patient had a persistent small residual shunt.
Complications
Minor periprocedural complications occurred in ten patients. Four patients developed hematomas at their venous puncture sites. A small pericardial effusion was noted in five patients. All patients were followed clini- cally without any need for drainage. During the implan- tation procedure, a pacemaker lead dislodged in one patient and required re-implantation. All periprocedural complications resolved without long-term sequelae. Dur- ing follow-up, one patient was noted to have a femoral pseudoaneurysm one year after her procedure, which required surgical repair. However, this patient under- went another cardiac catheterization two weeks prior to the closure procedure. Four patients died during follow- up, and all expired for reasons unrelated to ASD closure (one due to chronic liver disease, one due to ischemic heart disease, and two due to other severe cardiovascu- lar comorbidities).
Discussion
Our data support prior published data suggesting that ASD closure is safe and effective, even in patients over 60 years of age.3)7) This finding is consistent with the recently published recommendations issued by the Ame- rican College of Cardiology and the American Heart As- sociation addressing the care of adults with congenital heart disease. These guidelines state that any hemody- namically significant ASD should be considered for clo- sure, irrespective of age.15) There are, however, several differences in the treatment strategies and potential benefits of ASD closure in adult and pediatric patients.
First, although the indications for transcatheter clo- sure are the same as for surgical closure, the former mo- dality has lower periprocedural morbidity in all age groups. Presumably due to the higher incidence of co- morbidities in elderly patients, age may have a significant impact on periprocedural mortality in surgically treated adult patients. Ghosh et al.,16) demonstrated that patients below 51 years of age carried a periprocedural surgical mortality of 0%, while patients above 51 years of age carried a periprocedural surgical mortality of 3.3%. This makes transcatheter ASD closure even more appealing in the elderly.
Second, except for some extraordinary circumstances, it is unlikely that ASD closure will provide a mortality benefit in the elderly age group.5)17)18) Nevertheless, our data, as well as data from other investigators, demon- strate that symptomatic patients improve following ASD closure, resulting in an improved quality of life.8)12)19)20)
But, even in asymptomatic patients, ASD closure can provide benefits such as favorable cardiac remodeling of
Table 2. Assessment of symptoms according to NYHA classifi- cation before and after closure of atrial septal defects
NYHA functional class Before, n (%) After, n (%)
I 05 (12) 24 (58)
II 19 (46) 11 (27)
III 15 (37) 0
IV 02 (5)0 0
Baseline functional status data was available for 41 patients, while follow-up data was available for 35 patients. NYHA: New York Heart Association
RVEDD (mm)
50 40 30 20 10
0
Before 24 hours 6-12 months Fig. 1. Serial changes in right ventricular end-diastolic diameter before and after atrial septal defect closure. RVEDD: right ventri- cular end-diastolic diameter.
50·ASD Closure in the Elderly
a dilated right ventricle. This may prevent development of frank right heart failure.19)20) Further, the functional capacity of patients with ASDs is substantially impa- ired.21) The subjective impression of functional capacity may be overestimated by patients with congenital heart disease, and it has been documented that functional ca- pacity improves even in patients who consider themse- lves asymptomatic.22)23)
Another important difference between pediatric and elderly patients is coexisting pulmonary arterial hyper- tension or left ventricular diastolic dysfunction caused by long standing hypertension in the latter group. Thus, it is important to carefully assess the feasibility of com- pletely closing the defect. As shown in the present study, the right ventricular size decreases soon after ASD clo- sure in elderly patients. The loss of a decompressive ASD can result in serious acute effects on left heart hemody- namics, which have been reported after surgical repair of ASDs.9)10) A possible explanation for this pathophysi- ologic mechanism in elderly patients is restrictive left ventricular diastolic dysfunction leading to left atrial hy- pertension and subsequent pulmonary edema.10) The ASD serves as a protective interatrial communication, reducing the left ventricular preload through left-to- right shunting. Therefore, we placed a fenestrated ASO in two patients and left a small defect open in two other patients who had multiple ASDs. This outlines the im- portance of careful hemodynamic assessment of poten- tial left ventricular dysfunction in elderly patients with moderate-to-large ASDs. We recommend evaluation of this hemodynamic phenomenon by temporary balloon occlusion of the defect in any patient with a baseline left atrial pressure of ≥18 mmHg for 15-20 minutes, as de- scribed in the methods section of this paper and detailed in a more extensive manner in an earlier publication.24)
Finally, atrial fibrillation is part of the natural course of an untreated ASD. It is more likely for an adult pa- tient presenting with an ASD to be in atrial fibrillation at the time of diagnosis than it is for a child or adoles- cent. This is simply due to the hemodynamic effects of the ASD on right and left atrial size, which lead to myo- cardial stretch and atrial fibrillation over time. A land- mark study evaluating the effect of surgical ASD closure has documented that ASD closure beyond the age of 40 has no effect on the future development of atrial fib- rillation.6) In our study, patients in atrial fibrillation at baseline remained in this rhythm, except for those un- dergoing radiofrequency ablation. A temporary increase in atrial fibrillation was documented following occluder placement in a different patient population in a previ- ous study.25) We were not able to reproduce this finding in the present study.
Our study has several limitations, including a retro- spective design, incomplete follow-up data, and a lack of a control group. Nevertheless, the present study con-
firms the positive impact of ASD closure on right ven- tricular remodeling and functional status.
In conclusion, ASD closure is safe and effective in elderly patients. Our data and prior published data con- sistently demonstrate that even patients above 60 years of age experience improvement in functional status and right ventricular remodeling. Patient age should not in- fluence the decision of whether an ASD should be closed.
However, careful assessment of hemodynamic status is warranted prior to complete closure of the defect.
REFERENCES
1) Du ZD, Hijazi ZM, Kleinman CS, Silverman NH, Larntz K. Com- parison between transcatheter and surgical closure of secundum atrial septal defect in children and adults: results of a multicen- ter nonrandomized trial. J Am Coll Cardiol 2002;39: 1836-44.
2) Fischer G, Stieh J, Uebing A, Hoffmann U, Morf G, Kramer HH.
Experience with transcatheter closure of secundum atrial septal defects using the Amplatzer septal occluder: a single centre study in 236 consecutive patients. Heart 2003;89:199-204.
3) Spies C, Timmermanns I, Schrader R. Transcatheter closure of secundum atrial septal defects in adults with the Amplatzer sep- tal occluder: intermediate and long-term results. Clin Res Cardiol 2007;96:340-6.
4) Masura J, Gavora P, Podnar T. Long-term outcome of transcathe- ter secundum-type atrial septal defect closure using Amplatzer septal occluders. J Am Coll Cardiol 2005;45:505-7.
5) Murphy JG, Gersh BJ, McGoon MD, et al. Long-term outcome after surgical repair of isolated atrial septal defect: follow-up at 27 to 32 years. N Engl J Med 1990;323:1645-50.
6) Gatzoulis MA, Freeman MA, Siu SC, Webb GD, Harris L. Atrial arrhythmia after surgical closure of atrial septal defects in adults.
N Engl J Med 1999;340:839-46.
7) Elshershari H, Cao QL, Hijazi ZM. Transcatheter device closure of atrial septal defects in patients older than 60 years of age: im- mediate and follow-up results. J Invasive Cardiol 2008;20:173-6.
8) Jemielity M, Dyszkiewicz W, Paluszkiewicz L, Perek B, Bucz- kowski P, Ponizynski A. Do patients over 40 years of age benefit from surgical closure of atrial septal defects? Heart 2001;85:300-3.
9) Beyer J. Atrial septal defect: acute left heart failure after surgical closure. Ann Thorac Surg 1978;25:36-43.
10) Ewert P, Berger F, Nagdyman N, et al. Masked left ventricular restriction in elderly patients with atrial septal defects: a con- traindication for closure? Catheter Cardiovasc Interv 2001;52:
177-80.
11) Hijazi ZM. Catheter closure of atrial septal and ventricular septal defects using the Amplatzer devices. Heart Lung Circ 2003;12 (Suppl 2):S63-72.
12) Hijazi ZM, Cao Q, Patel HT, Rhodes J, Hanlon KM. Transeso- phageal echocardiographic results of catheter closure of atrial septal defect in children and adults using the Amplatzer device.
Am J Cardiol 2000;85:1387-90.
13) Harper RW, Mottram PM, McGaw DJ. Closure of secundum atrial septal defects with the Amplatzer septal occluder device: techni- ques and problems. Catheter Cardiovasc Interv 2002;57:508-24.
14) Boutin C, Musewe NN, Smallhorn JF, Dyck JD, Kobayashi T, Benson LN. Echocardiographic follow-up of atrial septal defect after catheter closure by double-umbrella device. Circulation 1993;
88:621-7.
15) Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 Guidelines for the Management of Adults With Congenital Heart
Christian Spies, et al.·51
Disease: a report of the American College of Cardiology/Ameri- can Heart Association Task Force on Practice Guidelines (writing committee to develop guidelines on the management of adults with congenital heart disease). Circulation 2008;118:e714-833.
16) Ghosh S, Chatterjee S, Black E, Firmin RK. Surgical closure of atrial septal defects in adults: effect of age at operation on out- come. Heart 2002;88:485-7.
17) Konstantinides S, Geibel A, Olschewski M, et al. A comparison of surgical and medical therapy for atrial septal defect in adults.
N Engl J Med 1995;333:469-73.
18) Attie F, Rosas M, Granados N, Zabal C, Buendia A, Calderon J.
Surgical treatment for secundum atrial septal defects in patients
>40 years old: a randomized clinical trial. J Am Coll Cardiol 2001;38:2035-42.
19) Kort HW, Balzer DT, Johnson MC. Resolution of right heart enlargement after closure of secundum atrial septal defect with transcatheter technique. J Am Coll Cardiol 2001;38:1528-32.
20) Du ZD, Cao QL, Koenig P, Heitschmidt M, Hijazi ZM. Speed of normalization of right ventricular volume overload after trans-
catheter closure of atrial septal defect in children and adults. Am J Cardiol 2001;88:1450-3, A9.
21) Fredriksen PM, Veldtman G, Hechter S, et al. Aerobic capacity in adults with various congenital heart diseases. Am J Cardiol 2001;
87:310-4.
22) Diller GP, Dimopoulos K, Okonko D, et al. Exercise intolerance in adult congenital heart disease: comparative severity, correlates, and prognostic implication. Circulation 2005;112:828-35.
23) Veldtman GR, Razack V, Siu S, et al. Right ventricular form and function after percutaneous atrial septal defect device closure. J Am Coll Cardiol 2001;37:2108-13.
24) Holzer R, Cao QL, Hijazi ZM. Closure of a moderately large atrial septal defect with a self-fabricated fenestrated Amplatzer septal occluder in an 85-year-old patient with reduced diastolic elasticity of the left ventricle. Catheter Cardiovasc Interv 2005;
64:513-8.
25) Spies C, Khandelwal A, Timmermanns I, Schrader R. Incidence of atrial fibrillation following transcatheter closure of atrial sep- tal defects in adults. Am J Cardiol 2008;102:902-6.