Comparison of Pelvic Phased-Array versus Endorectal Coil Magnetic Resonance Imaging at 3 Tesla for Local Staging
of Prostate Cancer
Bum Soo Kim, Tae-Hwan Kim, Tae Gyun Kwon, and Eun Sang Yoo
Department of Urology, School of Medicine, Kyungpook National University, Daegu, Korea.
Received: May 26, 2011 Revised: August 31, 2011 Accepted: September 8, 2011
Corresponding author: Dr. Eun Sang Yoo, Department of Urology, School of Medicine, Kyungpook National University,
130 Dongdeok-ro, Jung-gu, Daegu 700-721, Korea.
Tel: 82-53-420-5843, Fax: 82-53-421-9618 E-mail: [email protected]
∙ The authors have no financial conflicts of interest.
© Copyright:
Yonsei University College of Medicine 2012 This is an Open Access article distributed under the terms of the Creative Commons Attribution Non- Commercial License (http://creativecommons.org/
licenses/by-nc/3.0) which permits unrestricted non- commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Purpose: Several studies have demonstrated the superiority of endorectal coil magnetic resonance imaging (MRI) over pelvic phased-array coil MRI at 1.5 Tesla for local staging of prostate cancer. However, few have studied which evaluation is more accurate at 3 Tesla MRI. In this study, we compared the accuracy of local staging of prostate cancer using pelvic phased-array coil or endorectal coil MRI at 3 Tesla. Materials and Methods: Between January 2005 and May 2010, 151 pa- tients underwent radical prostatectomy. All patients were evaluated with either pel- vic phased-array coil or endorectal coil prostate MRI prior to surgery (63 endorec- tal coils and 88 pelvic phased-array coils). Tumor stage based on MRI was compared with pathologic stage. We calculated the specificity, sensitivity and ac- curacy of each group in the evaluation of extracapsular extension and seminal ves- icle invasion. Results: Both endorectal coil and pelvic phased-array coil MRI achieved high specificity, low sensitivity and moderate accuracy for the detection of extracapsular extension and seminal vesicle invasion. There were statistically no differences in specificity, sensitivity and accuracy between the two groups.
Conclusion: Overall staging accuracy, sensitivity and specificity were not signifi- cantly different between endorectal coil and pelvic phased-array coil MRI.
Key Words: Prostatic neoplasms, magnetic resonance imaging, neoplasm stag- ing, comparative study
INTRODUCTION
Prostate cancer remains a major health concern among the male population. Cur- rently, a rapid increase in prostate-specific antigen (PSA) screening has resulted in an increased detection rate of small cancers and an increased incidence of this dis- ease. In the evaluation of patients with prostate cancer, the most important factor affecting a patient’s prognosis and choice of management method is the disease stage at the time of diagnosis.1 For several decades, various imaging modalities have been assessed for staging of prostate cancer. Among these imaging modali- ties, magnetic resonance imaging (MRI), with its excellent soft-tissue contrast, provides high-resolution images of the prostate and surrounding structures.2-4
tient had difficulty or was contraindicated for ERC inser- tion (e.g., prior anorectal surgery, inflammatory bowel dis- ease, or high anal sphincter tension), the patient underwent MRI with a PAC.
MR imaging analysis
All patients were randomly scheduled to undergo 3 Tesla MRI (Signa Excite, GE Medical Systems, Waukesha, WI, USA) with either an ERC or a PAC prior to radical prosta- tectomy. In the MRI examination using a PAC (Pelvic Ar- ray, GE Healthcare, Waukesha, WI, USA), a commercially available eight-element standard PAC was placed around the pelvic area with the patient in the supine position. After localizing images were obtained, T2-weighted fast spin- echo image series in the transverse, sagittal, and coronal planes were obtained. Radiofrequency power deposition from the spin-echo train was reduced using hyperechoes.12 The T2-weighted imaging scan parameters were as follows:
TR/TE, 3700/104 ms; slice thickness, 4 mm; interslice gap, 0.4 mm; 320×224 matrix; FOV, 160×160 mm; number of excitations, 3; and scan time, 8 minutes 20 seconds.
In the MRI examination using an ERC (MR Innerva, Medrad, Pittsburgh, PA, USA), a commercially available balloon-covered expandable ERC was inserted with the pa- tient in the left lateral decubitus position. The balloon was then inflated with 40-60 mL of de-mineralized water. The patient was then placed in the supine position, and bowel movements were suppressed with an intramuscular injec- tion of 1 mg of glucagon. An ERC localization image series was obtained, and subsequently, T2-weighted fast spin- echo images were obtained with the use of hyperechoes in the transverse, sagittal, and coronal planes. Sequence pa- rameters were as follows: TR/TE, 3700/104 ms; slice thick- ness, 4 mm; interslice gap, 0.4 mm; 320×224 matrix; FOV, 160×160 mm; number of excitations, 3; and scan time, 8 minutes 20 seconds. Of these 151 patients, 63 patients un- derwent prostate MRI with an ERC, and 88 patients under- went prostate MRI with a PAC. Radiologic interpretations were made by consensus of two radiologists. One radiolo- gist had more than 10 years of experience with prostate MRI with the use of a PAC at 1.5 Tesla and 3 years of ex- perience with the use of an ERC at 1.5 Tesla. The other ra- diologist had 2 years of experience with prostate MRI with the use of both ERC and PAC at 1.5 Tesla. The criteria for the diagnosis of extraprostatic extension included a bulge in the contour of the prostate, obliteration of the rectoprostatic angle, thickening or disruption of the prostatic capsule, an Although there has been much debate regarding whether
MRI should be used routinely for the diagnosis of prostate cancer, for over two decades, MRI has improved our ability to delineate localized versus locally advanced prostate can- cer.5 However, it has poor sensitivity for the detection of microscopic spread. Hence, various MR techniques, such as endorectal coil, higher Tesla and diffusion-weighted MRI, have been proposed to improve the morphological imaging quality of prostate cancers. To date, several studies have suggested that MRI using an endorectal coil (ERC) is the most promising technique for the detection and staging of prostate cancer. Especially, at standard clinical field strengths of 1.5 Tesla, an ERC is necessary to obtain a suf- ficiently high signal-to-noise ratio (SNR) with subsequent spatial resolution, which allows for more reliable cancer de- lineation in a clinically reasonable timeframe.6-8 However, the use of an ERC is more time-consuming, entails higher costs and causes greater discomfort in the patient.9,10 More- over, at higher magnetic field strengths, such as 3 Tesla, SNR increases in standard MRI, and the need for an ERC for the detection or localization of prostate cancer at this magnetic field strength has not yet been resolved.11 There- fore, it is important to determine whether an ERC remains necessary or whether a pelvic phased-array coil (PAC) could suffice for staging of prostate cancer at 3 Tesla MRI.
Thus, we compared the prostate cancer local-staging per- formance of ERC and PAC MRI at 3 Tesla along with his- topathologic findings as a reference standard.
MATERIALS AND METHODS
Patient characteristics
Between January 2005 and May 2010, 151 consecutive pa- tients, who met our inclusion criteria and had biopsy-prov- en prostate cancer, underwent radical prostatectomy at our institution. Of these patients, 33 patients underwent open radical retropubic prostatectomy, while 118 patients under- went robotic-assisted laparoscopic surgery. All surgeries were performed by one oncologic urologist who had expe- rience in more than 100 cases of radical prostatectomies.
Exclusion criteria were contraindications for MRI (e.g., pacemaker and metal cerebral clips) as well as severe claus- trophobia. Additionally, patients who received neoadjuvant hormonal therapy or radiotherapy after MRI examination and patients who had undergone a prostate biopsy and MRI within 3 weeks of each other were also excluded. If a pa-
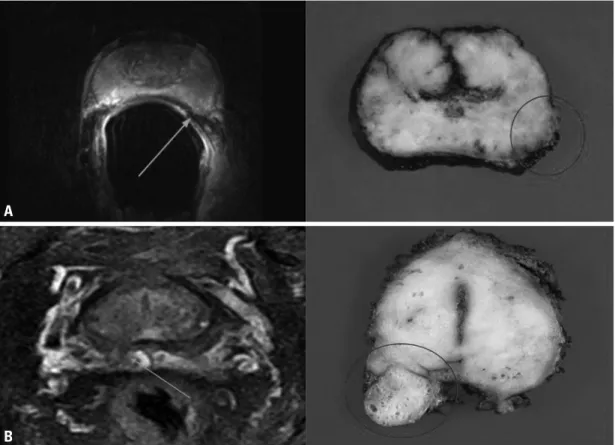
extent of each cancer focus, and radical distance of each ex- tracapsular penetration were determined by a genitourinary histopathologist with 13 years of experience who was blind- ed to the MRI results. The MRI findings were compared with the histopathologic findings of the radical prostatecto- my specimen in each patient (Fig. 1).
Statistical analysis
Sensitivity, specificity, positive prediction values, negative prediction values, and overall accuracy in prediction of ex- tracapsular extension and seminal vesicle invasion were calculated by dichotomizing the readings. Calculated SNR values of each sequence were expressed as the mean±SD and compared using Student’s t-test. Statistical significance differences in sensitivity, specificity, positive prediction val- ue, negative prediction value, and accuracy between the ERC MRI group and PAC MRI group were determined us- ing the Chi square test. All statistical analyses were con- ducted using SPSS 12.0 for Windows, and statistical signif- icance was accepted at a p-value less than 0.05.
infiltrative strand in the periprostatic fat, or asymmetry of the neurovascular bundle. Seminal vesicle invasion was de- fined by the presence of abnormal tissue with low signal in- tensity within the seminal vesicle or dilatation of the semi- nal vesicle with asymmetry on T2-weighted images. T1- weighted images were used to rule out false-positive findings caused by post-biopsy hemorrhage; if a low signal intensity lesion on a T2-weighted image matched a high signal inten- sity, then this area was considered a biopsy hematoma. Fur- thermore, SNRs of the entire prostate region for ERC and PAC MRI groups were calculated.
Histopathologic examination
After excision, prostatectomy specimens were fixed over- night in 10% neutral buffered formaldehyde and coated with India ink. Four-millimeter-interval whole-mount sec- tions were cut at a plane likewise to the transverse MRI plane. All sections were routinely embedded in paraffin. Tis- sue sections of 5 μm were prepared and stained with hema- toxylin-eosin. The exact localization, volume, Gleason score,
Fig. 1. Comparison of a T2-weighted fast spin-echo magnetic resonance image at 3 Tesla and a corresponding axial whole-mount-sec- tion histopathologic slice (A) example of a tumor with a 2-mm radial distance of extracapsular extension (arrow) (prostate-specific anti- gen level, 7.8 ng/mL; final Gleason score, 3+4; stage, pT3a) that was detected with ERC MRI in a 61-year-old man, and histopathologic ex- amination confirmed the presence of extracapsular entension at the left lateral side (circle) (B) example of a tumor with a 8-mm radial distance of extracapsular extension (arrow) (prostate-specific antigen level, 10.6 ng/mL; final Gleason score, 4+3; stage, pT3a) that was detected with PAC MRI in a 64-year-old man, and histopathologic examination confirmed the presence of extracapsular entension at the right dorsal side (circle). ERC, endorectal coil; PAC, phased-array coil; MRI, magnetic resonance imaging.
A
B
with extraprostatic extension and 13 patients with seminal vesicle invasion. Of 88 patients, PAC MRI discovered sus- pected extraprostatic extension in 15 patients and suspected seminal vesicle invasion in 9 patients, while histopatholog- ic analysis revealed 48 patients with extraprostatic exten- sion and 21 patients with seminal vesicle invasion. The sen- sitivity, specificity, and overall accuracy for the detection of extraprostatic extension were 33.3%, 96.6%, and 63.5% for ERC MRI and 31.3%, 97.5%, and 61.4% for PAC MRI, re- spectively (Table 2). Additionally, the sensitivity, specifici- ty, and overall accuracy for the detection of seminal vesicle invasion were 46.2%, 92.0%, and 82.5% for ERC MRI and
RESULTS
Table 1 summarizes the clinicopathologic data of the ERC MRI and PAC MRI groups. The mean age, mean preopera- tive PSA level, average time interval between prostate bi- opsy and MRI examination, ratio of open/robotic surgery, Gleason score at biopsy, and prostatectomy were not signif- icantly different between the two groups. Of 63 patients, ERC MRI discovered suspected extraprostatic extension in 11 patients and suspected seminal vesicle invasion in 6 pa- tients, while histopathologic analysis revealed 33 patients Table 1. Clinicopathologic Characteristics of the Patients
Endorectal coil MRI Pelvic phased-array coil MRI p value
No. of patients 63 88
Mean age (yrs)* 64.8 (47-76) 66.8 (55-76) 0.127
Mean preoperative PSA level (ng/mL)* 11.69 (3.0-37.0) 12.36 (4.0-38.0) 0.386
Interval between biopsy and MRI (days)* 28.18 (22-45) 27.65 (24-45) 0.707
Operation method (ORRP/RARP) 13/50 20/68 0.759
Gleason score at biopsy† 0.757
6 35 (55.5) 50 (56.8)
7 18 (28.6) 22 (25.0)
8 9 (14.3) 12 (13.6)
9 1 (1.6) 4 (4.5)
Gleason score at prostatectomy† 0.544
6 19 (30.2) 23 (26.1)
7 28 (44.4) 42 (47.7)
8 13 (20.6) 14 (15.9)
9 3 (4.8) 9 (10.2)
MRI, magnetic resonance imaging; PSA, prostate specific antigen; ORRP, open retropubic radical prostatectomy; RARP, robotic-assisted laparoscopic radi- cal prostatectomy.
*Data in parentheses are ranges.
†Data in parentheses are percentages.
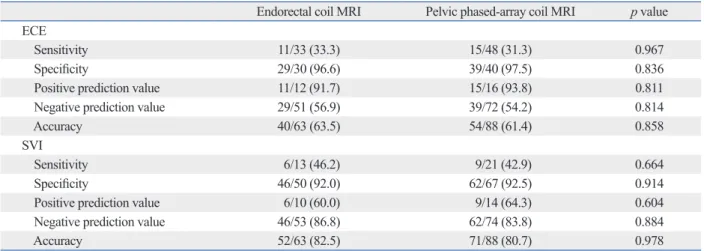
Table 2. Comparison of Local Staging Performance between Endorectal Coil and External Surface Coil MRI for Detecting Ex- traprostatic Extension and Seminal Vesicle Invasion of Prostate Cancer
Endorectal coil MRI Pelvic phased-array coil MRI p value ECE
Sensitivity 11/33 (33.3) 15/48 (31.3) 0.967
Specificity 29/30 (96.6) 39/40 (97.5) 0.836
Positive prediction value 11/12 (91.7) 15/16 (93.8) 0.811
Negative prediction value 29/51 (56.9) 39/72 (54.2) 0.814
Accuracy 40/63 (63.5) 54/88 (61.4) 0.858
SVI
Sensitivity 6/13 (46.2) 9/21 (42.9) 0.664
Specificity 46/50 (92.0) 62/67 (92.5) 0.914
Positive prediction value 6/10 (60.0) 9/14 (64.3) 0.604
Negative prediction value 46/53 (86.8) 62/74 (83.8) 0.884
Accuracy 52/63 (82.5) 71/88 (80.7) 0.978
MRI, magnetic resonance imaging; ECE, extracapsular extension; SVI, seminal vesicle invasion.
Data in parentheses are percentages.
extension, the sensitivity, specificity, and accuracy of en- dorectal coil MRI has been reported to range from 13-71%, 47-97%, and 58-91%, respectively, whereas for the detec- tion of seminal vesicle invasion, the sensitivity, specificity, and accuracy of endorectal MRI has been reported to range from 33-71%, 83-99%, and 80-95%, respectively.21-23 In our study, the sensitivity, specificity, and accuracy of endorectal coil MRI for the detection of extraprostatic extension was 33.3%, 96.6%, and 63.5%, respectively, and the sensitivity, specificity, and accuracy of the detection of seminal vesicle invasion was 46.2%, 92.0%, and 82.5%, respectively.
This wide range of specificities and sensitivities of MRI in the assessment of extraprostatic extension and seminal vesicle invasion is due to a combination of factors includ- ing considerable interobserver variability14,24 as well as the lack of standardized diagnostic criteria.25,26 In addition, the oncologic characteristics of preoperative patients are also important factors. Recent studies demonstrated that sensi- tivity was higher in poorly differentiated prostate cancer and/or intermediate and high-risk groups.7,27 Low-risk groups and well-differentiated cancer groups may not usually have extraprostatic extension. However, they have a greater chance of microscopic invasion rather than gross invasion, if they indeed do have extraprostatic invasion. Further, MRI still has a limitation in the detection of microscopic spread.
A large population in the low-risk group (Gleason score 6 and less than 10 of preoperative serum PSA level) and a high upgrading rate in Gleason scores after radical prosta- tectomy may be one of the main factors of low sensitivity in our study. In addition, low sensitivity may be attributable to post-biopsy changes. While the amount of hemorrhaging often varies, it can be profound and involve large segments 42.9%, 92.5%, and 80.7% for PAC MRI, respectively (Ta-
ble 2). Statistically, there were no significant differences in sensitivity, specificity, and accuracy between the two groups.
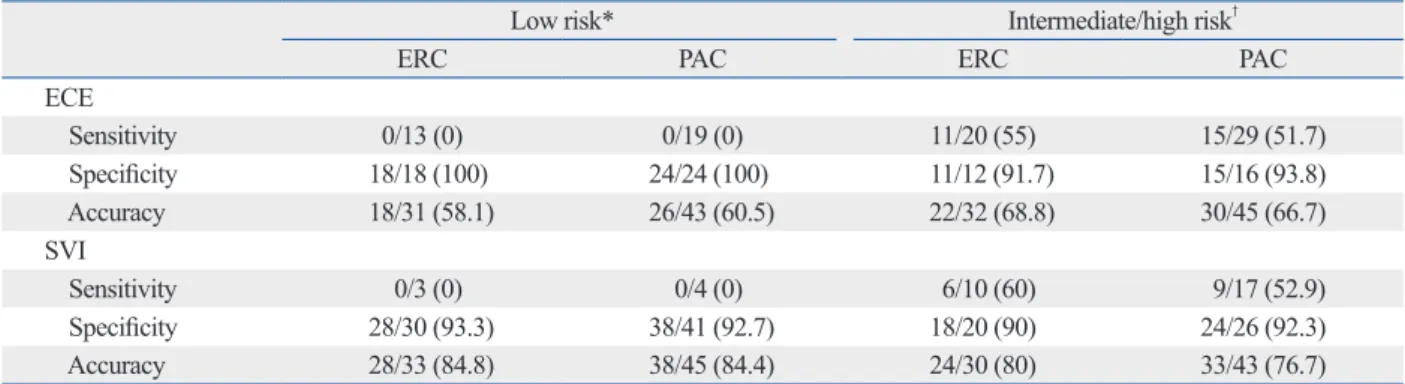
The sensitivity of both ERC and PAC MRI for the detec- tion of extraprostatic extension and seminal vesicle inva- sion tended to increase in the intermediate/high risk group (Table 3).
The SNR of ERC MRI was 14.75±3.92 and 11.53±3.44 for PAC MRI. Although the SNR was slightly higher in the ERC MRI group, there was no statistically significant dif- ference (p=0.081).
DISCUSSION
In the past, the use of computed tomography and MRI to evaluate the local extent of prostate cancer was not routine- ly recommended because of low sensitivity and accompa- nying low cost-effectiveness.13-15 However, with continuous developments in better technology, MRI has become in- creasingly implemented for the diagnosis and staging of prostate cancer. Recent studies reported that dynamic con- trast-enhanced MRI are useful for the staging work-up of prostate cancer.16-18 In addition, proton MR spectroscopic imaging and functional MRI can further improve the detec- tion rate of cancer while enhancing the assessment of tu- mors’ aggressiveness, volume, and extent.16-19 Especially, endorectal coil MRI seems to be the most accurate imaging modality available for the evaluation of extensiveness of prostate cancer, replacing pelvic phased-array MRI of the prostate due to higher spatial and contrast resolution, im- proving image quality.8,20 For the detection of extraprostatic
Table 3. Local Staging Performance of the Patients Stratified in the Low and Intermediate/high Risk Groups for Preoperative Endorectal Coil and External Surface Coil MRI
Low risk* Intermediate/high risk†
ERC PAC ERC PAC
ECE
Sensitivity 0/13 (0) 0/19 (0) 11/20 (55) 15/29 (51.7)
Specificity 18/18 (100) 24/24 (100) 11/12 (91.7) 15/16 (93.8)
Accuracy 18/31 (58.1) 26/43 (60.5) 22/32 (68.8) 30/45 (66.7)
SVI
Sensitivity 0/3 (0) 0/4 (0) 6/10 (60) 9/17 (52.9)
Specificity 28/30 (93.3) 38/41 (92.7) 18/20 (90) 24/26 (92.3)
Accuracy 28/33 (84.8) 38/45 (84.4) 24/30 (80) 33/43 (76.7)
ERC, endorectal coil; PAC, pelvic phased-array coil; ECE, extracapsular extension; SVI, seminal vesicle invasion; PSA, prostate-specific antigen.
Data in parentheses are percentages.
*Low risk: clinical stage T1c to T2a and PSA ≤10 and Gleason score 6.
†Intermediate/high risk: clinical stage ≥T2b or PSA >10 or Gleason score ≥7.
the local staging of prostate cancer.
REFERENCES
1. Epstein JI, Partin AW, Sauvageot J, Walsh PC. Prediction of pro- gression following radical prostatectomy. A multivariate analysis of 721 men with long-term follow-up. Am J Surg Pathol 1996;20:
286-92.
2. Hricak H, Williams RD, Spring DB, Moon KL Jr, Hedgcock MW, Watson RA, et al. Anatomy and pathology of the male pelvis by magnetic resonance imaging. AJR Am J Roentgenol 1983;141:
1101-10.
3. Bryan PJ, Butler HE, LiPuma JP, Haaga JR, El Yousef SJ, Resnick MI, et al. NMR scanning of the pelvis: initial experience with a 0.3 T system. AJR Am J Roentgenol 1983;141:1111-8.
4. Phillips ME, Kressel HY, Spritzer CE, Arger PH, Wein AJ, Mari- nelli D, et al. Prostatic disorders: MR imaging at 1.5 T. Radiology 1987;164:386-92.
5. Nishimoto K, Nakashima J, Hashiguchi A, Kikuchi E, Miyajima A, Nakagawa K, et al. Prediction of extraprostatic extension by prostate specific antigen velocity, endorectal MRI, and biopsy Gleason score in clinically localized prostate cancer. Int J Urol 2008;15:520-3.
6. Engelbrecht MR, Jager GJ, Laheij RJ, Verbeek AL, van Lier HJ, Barentsz JO. Local staging of prostate cancer using magnetic reso- nance imaging: a meta-analysis. Eur Radiol 2002;12:2294-302.
7. Park SY, Kim JJ, Kim TH, Lim SH, Han DH, Park BK, et al. The role of endorectal magnetic resonance imaging in predicting extra- prostatic extension and seminal vesicle invasion in clinically local- ized prostate cancer. Korean J Urol 2010;51:308-12.
8. Hricak H, White S, Vigneron D, Kurhanewicz J, Kosco A, Levin D, et al. Carcinoma of the prostate gland: MR imaging with pelvic phased-array coils versus integrated endorectal--pelvic phased-ar- ray coils. Radiology 1994;193:703-9.
9. Lee SH, Park KK, Choi KH, Lim BJ, Kim JH, Lee SW, et al. Is endorectal coil necessary for the staging of clinically localized prostate cancer? Comparison of non-endorectal versus endorectal MR imaging. World J Urol 2010;28:667-72.
10. Heijmink SW, Fütterer JJ, Hambrock T, Takahashi S, Scheenen TW, Huisman HJ, et al. Prostate cancer: body-array versus en- dorectal coil MR imaging at 3 T--comparison of image quality, lo- calization, and staging performance. Radiology 2007;244:184-95.
11. Rouvière O, Hartman RP, Lyonnet D. Prostate MR imaging at high-field strength: evolution or revolution? Eur Radiol 2006;16:
276-84.
12. Hennig J, Scheffler K. Hyperechoes. Magn Reson Med 2001;46:
6-12.
13. Rifkin MD, Zerhouni EA, Gatsonis CA, Quint LE, Paushter DM, Epstein JI, et al. Comparison of magnetic resonance imaging and ultrasonography in staging early prostate cancer. Results of a multi- institutional cooperative trial. N Engl J Med 1990;323:621-6.
14. Tempany CM, Zhou X, Zerhouni EA, Rifkin MD, Quint LE, Pic- coli CW, et al. Staging of prostate cancer: results of Radiology Di- agnostic Oncology Group project comparison of three MR imag- ing techniques. Radiology 1994;192:47-54.
15. Levran Z, Gonzalez JA, Diokno AC, Jafri SZ, Steinert BW. Are pelvic computed tomography, bone scan and pelvic lymphadenec- tomy necessary in the staging of prostatic cancer? Br J Urol 1995;
of the peripheral zone. Hematoma and edema can mimic not only tumor and capsular penetration but also seminal vesicle invasion as well.
High diagnostic specificity indicates less chance of false- positives and thus helps to ensure that few patients will be deprived of potentially curative surgery. It is accepted that tests with high specificity, even if accompanied by low sen- sitivity, offer a more cost-effective approach for patients be- ing considered for surgery in the management of prostate cancer.28 Moreover, most errors in assessing extracapsular extension by MRI lie with false-negative results, as MRI even at 3 Tesla has difficulty detecting microscopic inva- sion of the capsule, which is noted in pathologic examina- tions. However, microscopic invasion of the capsule with- out seminal vesicle invasion or a positive surgical margin may not change the disease-free survival rate from that as- sociated with pathologically organ-confined disease treated with radical prostatectomy.29
Although several studies demonstrated significant im- provements in the quality of MR imaging of the prostate with the use of an ERC, ERC MRI requires more time, in- volves higher costs, and can causes greater discomfort in the patient; even further, it cannot be performed in patients with prior anorectal surgery, inflammatory bowel disease, and high anal sphincter tone. In contrast, the use of a PAC alone for signal reception can save time and costs as well as cause less discomfort in the patient. In addition, higher magnetic field strengths of 3 Tesla can increase the SNR and can improve the image quality of PAC MRI. In our study, there were no significant differences in sensitivity, specificity, positive prediction value, negative prediction value, and overall accuracy as well as SNR for the detec- tion of extracapsular extension and seminal vesicle inva- sion between ERC and PAC MRI.
The present study has some limitations. This study was retrospectively designed and performed at single center. In addition, study method of comparing two modalities was limited to comparing two groups of patients rather than two distinct diagnostic methods in the same patient. This meth- odological flaw might have biased the results, affecting their validity.
In conclusion, both ERC and PAC prostate MRI at 3 Tes- la have high specificity and low sensitivity for the detection of extracapsular extension and seminal vesicle invasion.
Overall staging accuracy, sensitivity, and specificity were not significantly different between the two groups. There- fore, 3 Tesla PAC MRI can be an effective alternative for
calised prostate cancer prior to radical prostatectomy. Eur Radiol 1999;9:29-34.
24. Mullerad M, Hricak H, Wang L, Chen HN, Kattan MW, Scardino PT. Prostate cancer: detection of extracapsular extension by geni- tourinary and general body radiologists at MR imaging. Radiology 2004;232:140-6.
25. Yu KK, Hricak H, Alagappan R, Chernoff DM, Bacchetti P, Za- loudek CJ. Detection of extracapsular extension of prostate carci- noma with endorectal and phased-array coil MR imaging: multi- variate feature analysis. Radiology 1997;202:697-702.
26. Outwater EK, Petersen RO, Siegelman ES, Gomella LG, Chernesky CE, Mitchell DG. Prostate carcinoma: assessment of diagnostic criteria for capsular penetration on endorectal coil MR images.
Radiology 1994;193:333-9.
27. Fütterer JJ, Engelbrecht MR, Jager GJ, Hartman RP, King BF, Hulsbergen-Van de Kaa CA, et al. Prostate cancer: comparison of local staging accuracy of pelvic phased-array coil alone versus in- tegrated endorectal-pelvic phased-array coils. Local staging accu- racy of prostate cancer using endorectal coil MR imaging. Eur Radiol 2007;17:1055-65.
28. Coakley FV, Qayyum A, Kurhanewicz J. Magnetic resonance im- aging and spectroscopic imaging of prostate cancer. J Urol 2003;
170(6 Pt 2):S69-75.
29. Wieder JA, Soloway MS. Incidence, etiology, location, prevention and treatment of positive surgical margins after radical prostatec- tomy for prostate cancer. J Urol 1998;160:299-315.
75:778-81.
16. Kayhan A, Fan X, Oto A. Dynamic contrast-enhanced magnetic resonance imaging in prostate cancer. Top Magn Reson Imaging 2009;20:105-12.
17. Engelbrecht MR, Huisman HJ, Laheij RJ, Jager GJ, van Leenders GJ, Hulsbergen-Van De Kaa CA, et al. Discrimination of prostate cancer from normal peripheral zone and central gland tissue by using dynamic contrast-enhanced MR imaging. Radiology 2003;229:248-54.
18. Buckley DL, Roberts C, Parker GJ, Logue JP, Hutchinson CE.
Prostate cancer: evaluation of vascular characteristics with dy- namic contrast-enhanced T1-weighted MR imaging--initial expe- rience. Radiology 2004;233:709-15.
19. Claus FG, Hricak H, Hattery RR. Pretreatment evaluation of pros- tate cancer: role of MR imaging and 1H MR spectroscopy. Radio- graphics 2004;24 Suppl 1:S167-80.
20. Schnall MD, Imai Y, Tomaszewski J, Pollack HM, Lenkinski RE, Kressel HY. Prostate cancer: local staging with endorectal surface coil MR imaging. Radiology 1991;178:797-802.
21. Ikonen S, Kärkkäinen P, Kivisaari L, Salo JO, Taari K, Vehmas T, et al. Magnetic resonance imaging of clinically localized prostatic cancer. J Urol 1998;159:915-9.
22. Nakashima J, Tanimoto A, Imai Y, Mukai M, Horiguchi Y, Nakaga- wa K, et al. Endorectal MRI for prediction of tumor site, tumor size, and local extension of prostate cancer. Urology 2004;64:101-5.
23. Rørvik J, Halvorsen OJ, Albrektsen G, Ersland L, Daehlin L, Hau- kaas S. MRI with an endorectal coil for staging of clinically lo-