대흉외지 2006;39:795-798 □ 증례보고 □
- 795 - CASE REPORT
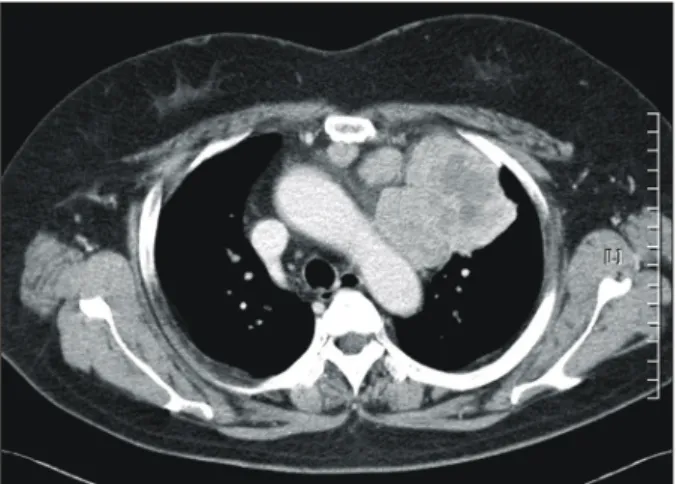
A 58-year-old woman was referred to our hospital for the investigation and treatment of a huge anterior mediastinal mass. Her initial symptoms were right chest pain, dyspnea, and palpitation. Computed tomography of her chest and a chest MRI revealed a 10×9×5.5 cm sized lobulated mass in
her anterior mediastinum (Fig. 1). Moon face appearance was present initially, but was overlooked. A fine needle aspiration biopsy was performed to rule out possibility of lung origin and the biopsy revealed findings suggestive of thymoma. A left thymectomy was then performed.
A median sternotomy incision was done. A well-encapsulated large lobular mass containing dark blood-like fluid was bordered
A Case Report of Thymic Carcinoid Tumor Associated with Cushing’s Syndrome:
Possible Corticotropin-Releasing Hormone Secreting Tumor
Soon-Ho Chon, M.D.*, Chul Burm Lee, M.D.*, Sun Kyun Ro, M.D.**, Young-Ha Oh, M.D.***, Jun Goo Kang, M.D.****, Jong Hoon Yeom, M.D.*****
Thymic carcinoid tumor associated with Cushing's syndrome is a rare disease with a poor prognosis. Thymic carcinoid with Cushing's syndrome caused by CRH (corticotropin-releasing hormone) production is even rarer. We report a 58-year-old woman with a huge anterior mediastinal mass. Five months after thymectomy the patient was readmitted with symptoms of generalized edema and dyspnea. Recurrence and metastases were discovered and Cushing's syndrome diagnosed.
(Korean J Thorac Cardiovasc Surg 2006;39:795-798) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Key words: 1. Thymus
2. Thymectomy 3. Carcinoid tumor 4. Cushing's syndrome
*한양대학교 의과대학 구리병원 흉부외과
Department of Thoracic and Cardiovascular Surgery, Hanyang University Guri Hospital, Hanyang University College of Medicine
**한양대학교 의과대학 서울병원 흉부외과
Department of Thoracic and Cardiovascular Surgery, Hanyang University Hospital, Hanyang University College of Medicine
***한양대학교 의과대학 구리병원 병리과
Department of Pathology, Hanyang University Guri Hospital, Hanyang University College of Medicine
****한림대학교 의과대학 평촌병원 내과
Department of Internal Medicine, Hallym University Pyongchon Hospital, Hanyang University College of Medicine
*****한양대학교 의과대학 구리병원 마취과
Department of Anesthesiology, Hanyang University Guri Hospital, Hanyang University College of Medicine 논문접수일:2006년 3월 6일, 심사통과일:2006년 7월 31일
책임저자:이철범 (471-020) 경기도 구리시 교문동 249-1, 한양대학교 의과대학 구리병원 흉부외과 (Tel) 031-560-2301, (Fax) 031-568-9948, E-mail: [email protected]
본 논문의 저작권 및 전자매체의 지적소유권은 대한흉부외과학회에 있다.
쿠싱 증후군 일으킨 카르시노이드종양의 1예 보고:
코르티코트로핀분비호르몬 분비하는 종양 의증
전순호*․이철범*․노선균**․오영하***․강준구****․염종훈*****
대흉외지 2006;39:795-798
- 796 - superiorly by her left innominate vein, medially by aortic arch, inferiorly by pericardium, laterally by mediastinal pleura and left upper lobe. The mass was relatively well encapsulated and was moderately adhered to her pericardium, surrounding fat tissue, and left innominate vein. There was no adhesion to the lung.
Frozen sections revealed suspected lymphocytic thymoma. Partial thymectomy was performed because of the seemingly benign nature, being well encapsulated and cystic.
Gross examination presented a lobular and encapsulated mass and the cut surface revealed a partly solid and a partly cystic region showing areas of hemorrhage and necrosis. On histologic examination, there was residual thymic tissue with Hassall's corpuscles and small lymphocytes adjacent to the tumor. The tumor was highly cellular and revealed solid nests and trabecular pattern compartmentalized by delicate fibrovascular stroma (Fig. 2A). In the periphery of the mass, the tumor cells also formed ribbon-like or Indian file appearance. Lymphatic tumor emboli were frequently seen.
The tumor cells were uniform and had granular eosinophilic cytoplasm. The nuclei were round with stippled powdery chr- omatin and inconspicuous nucleoli. Mitotic figures were occa- sionally seen. The tumor cells were positive for cytokeratin, neuron specific enolase, synaptophysin, and chromogranin, but negative for ACTH (Fig. 2B). Histopathologically, the tumor was diagnosed as atypical carcinoid tumor of the thymus.
The patient was discharged on her postoperative 16th day
and received postoperative radiotherapy at 5,000 rads one month later.
Five months later the patient developed symptoms of genera- lized edema and dyspnea. A chest CT revealed progression of tumor invading her pericardium and involvement of her right paratracheal lymph nodes. She also had shown direct invasion of her left phrenic nerve, presenting left hemidiaphragmatic el- evation. She was readmitted and found with high ACTH levels and a positive dexamethasone suppression test (high dose). Her free serum cortisol and plasma ACTH levels were 829μg/day and 103 pg/mL. The patient's T3, free T4, and TSH levels were within the normal range. The patient's urinary 17-OHCS levels were surprisingly suppressed by 8 mg of dexamethasone from 103 to 73 pg/mL. Following administration of 100μg ovine CRH intraveneously, blood ACTH actually decreased from 158 to 137 pmol/L (45 min). The response of cortisol levels to CRH was blunted (did not increase) from 23.6 to 21.6 nmol/L (45 min). Brain MRI had shown no signs of a pituitary lesion.
The patient had then refused all treatment, except for sim- ple pain control, and had expired 18 months after her initial operation.
DISCUSSION
Thymic carcinoid was first described in 1972 by Rosai and Higa[1] and since then over 150 cases have been reported.
There have been reports of carcinoid tumor in Korea, but, none associated with Cushing syndrome[2,3]. Thymic carcin- oid associated with Cushing's syndrome is a rare event and only 25 cases have been reported in the English literature.
Neuroendocrine carcinomas in the thymus account for 2 to 4% of all anterior mediastinal tumors[4]. There is only one other case in the English literature of a thymic carcinoid with Cushing's syndrome caused by CRH production[5]. Clinically, adrenocorticotropin hormone (ACTH) production in thymic carcinoid is not uncommon. Our case caused much confusion and we believe a thorough study including studies for pro- duction of CRH in patients with thymic carcinoid and Cu- shing's syndrome should be pursued. Such studies may prove to be an extremely important marker for recurrence or meta- stases.
Fig. 1. Chest CT reveals 10×9×5.5 cm sized solid and hetero- geneous mass with multiple lymphadenopathy. The mass is located in the anterior mediastinum and is attached to the aortic arch, pericardium, and anterior chest wall.
전순호 외 Thymic Carcinoid Tumor Associated with Cushing's Syndrome
- 797 - Thymic carcinoid tumors associated with Cushing's syndrome occur from 4 to 64 years of age and peak between the second and fourth decades. There is no gender preference when associated with Cushing's syndrome[4]. Elevated cortisol serum levels or 24-hour urine levels confirm the diagnosis of Cushing's syndrome. A drop in the 24-hour urine and plasma steroids of more than 50% of base line after 8 mg of an oral dexamethasone suppression test indicates a pituitary origin of ACTH[4]. Our case had a negative dexamethasone suppression test and negative findings on her brain MRI; this would suggest an origin other than the pituitary. An intravenous CRH test revealed a blunted increase in blood ACTH concentration, suggesting ectopic secretion of CRH. Unfortunately, antisera for CRH within the removed thymic carcinoid itself was not available, but clinically, such results would suggest a thymic carcinoid tumor with ectopic CRH production.
Surgery is the treatment of choice and aggressive local resection, including the entire thymus and perithymic fat, is necessary[4]. Due to the aggressive nature and frequent metastases, postoperative radiotherapy is usually indicated to prevent local recurrence. Glucocorticoids during the surgical procedure and postoperatively are indicated due to the pro- longed high cortisol levels, to prevent adrenal insufficiency during and after surgery[6]. In our case, the diagnosis of Cu- shing's syndrome was overlooked and thus, perioperative and postoperative doses of steroids were not given. Only after re-
currence, was Cushing's syndrome diagnosed and ectopic sec- retion of CRH discovered.
Immunohistochemical analysis of thymic carcinoid usually stains positive with chromogranin A and synaptophysin. The diagnosis of a carcinoid tumor is further supported by the pre- sence of neuron-specific enolase found in neuroendocrine cells of the amine precursor uptake and decarboxylation series[7].
ACTH usually is positive in those associated with Cushing's syndrome[4]. In our case, immunohistochemical studies for ne- uron specific enolase, chromogranin, and synoaptophysin were positive, but ACTH was negative. As mentioned above, unfor- tunately, antisera for CRH could not be obtained in our cou- ntry and ectopic secretion of CRH from a thymic carcinoid could only be suggested clinically.
The prognosis of thymic carcinoid is very poor and most patients will have local recurrence or metastasis within 5 years of surgery and expire within 10 years[4]. The five-year survival rate of thymic carcinoid has been reported to be 13% and the average survival at 3 years[8]. We believe a to- tal thymectomy and postoperative adjuvant therapy may have prolonged her survival. It was unfortunate that there was a discrepancy between preoperative, intraoperative and postoper- ative pathologic reports. Again, when Cushing's Rosai J, Hig syndrome associated with thymic carcinoid is encountered, a thorough study of not only ACTH, but also studies for CRH should be performed, especially in cases where a negative Fig. 2. Histologic and immunohisto- chemical findings. (A) The tumor is highly cellular and is arranged in solid nests and trabecular patterns divided by delicate fibrovascular st- roma (H&E, ×200). (B) The tumor cells are immunoreactive for chromo- granin (×200).
A B
대흉외지 2006;39:795-798
- 798 - study for ACTH is found.
REFERENCES
1. Rosai J, Higa E. Mediastinal endocrine neoplasm, of probable thymic origin, related to carcinoid tumor: clinicopathologic study of 8 cases. Cancer 1972;29:1061-74.
2. Lee JY, Kim MC, Yoo SY, Cho HL, Kang HM, Yang MH.
Thymic carcinoid tumor. Korean J Thorac Cardiovasc Surg 1998;31:319-23.
3. Kim SH, Lee JC, Han SS. Thymic carcinoid tumor. Korean J Thorac Cardiovasc Surg 1992;25:1236-9.
4. de Perrot M, Spiliopoulos A, Fischer S, Totsch M, Keshavjee
S. Neuroendocrine carcinoma (carcionoid) of the thymus as- sociated with Cushing's syndrome. Ann Thorac Surg 2002;73:
675-81.
5. Ozawa Y, Tomoyasu H, Takeshita A, et al. Shift from CRH to ACTH production in a thymic carcinoid with Cushing's syndrome. Horm Res 1996;45:264-8.
6. Byyny RL. Preventing adrenal insufficiency during surgery.
Postgrad Med 1980;67:2465-70.
7. Huntrakoon M, Lin F, Heitz PU, Tomita T. Thymic carci- noid tumor with Cushing's syndrome. Arch Pathol Lab Med 1984;108:551-4.
8. Wick MR, Bernatz PE, Carney JA, Brown LR. Primary me- diastinal carcinoid tumors. Am J Surg Pathol 1982;6:195-205.
=국문 초록=
쿠싱 증후군과 연관된 흉선 carcinoid 종양은 드문 질병으로 그 예후가 나쁜 것으로 알려져 있다. 그 중 부신피질자극 호르몬 분비 촉진 호르몬을 생산하는 흉선 carcinoid 종양은 훨씬 더 드물다. 우리는 거대한 전방 종격동 종양을 갖고 있는 58세 여자 환자에 대해 보고하려고 한다. 환자는 흉선제거술 5개월 후 전반적인 부종과 호흡곤란으로 다시 입원하였다. 환자는 재발과 전이가 발견되었고 쿠싱 증후군으로 진단 받았다.
중심 단어:1. 흉선 2. 흉선제거술 3. Carcinoid 종양 4. 쿠싱 증후군