서 론
인구 평균 수명이 늘어나면서 슬관절 퇴행성 관절염 환자는 점차 증가하는 추세이다. 슬관절의 심한 퇴행성 관절염 환자의 치료법 중 전치환술은 이러한 고령의 환자들에게 일차적으로 시도해볼 수 있는 좋은 치료 방법이다.1) 하지만 일차 슬관절 전치환술 환 자에서 수술 후 약 1,518 ml의 평균 혈액 손실이 보고되었으며, 이는 수술 후 동종 수혈의 증가와 직접적인 관련이 있다고 볼 수
Copyright © 2021 by The Korean Orthopaedic Association
“This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.”
The Journal of the Korean Orthopaedic Association Volume 56 Number 2 2021 Received March 5, 2020 Revised April 27, 2020 Accepted April 29, 2020
Correspondence to: Young Woo Chung, M.D.
Department of Orthopedic Surgery, Gwangju Veterans Hospital, 99 Cheomdanwolbong-ro, Gwangsan-gu, Gwangju 62284, Korea
TEL: +82-62-602-6162 FAX: +82-62-602-6936 E-mail: ywchungos@bohun.or.kr ORCID: https://orcid.org/0000-0001-9929-6769
일차 슬관절 전치환술 중 트라넥삼산의 정맥 내 투여와 국소 사용의 효과에 관한 비교 연구
이현주 • 안기용 • 박지연 • 정영우
광주보훈병원 정형외과
Efficacy of Tranexamic Acid during Primary Total Knee Arthroplasty:
Comparative Study between Intravenous Use and Topical Use
Hyun Ju Lee, M.D., Ki Yong An, M.D., Ji Yeon Park, M.D., and Young Woo Chung, M.D.
Department of Orthopedic Surgery, Gwangju Veterans Hospital, Gwangju, Korea
Purpose:
This study examined the effectiveness of tranexamic acid in reducing postoperative blood loss in total knee arthroplasty by comparing the methods of administration between an intravenous group, topical group, and non-tranexamic acid group.Materials and Methods: This was a retrospective case series study of patients who underwent primary total knee arthroplasty from
March 2017 to February 2019 performed by a single surgeon. The study population was divided into three groups according to the method of tranexamic acid administration (Group I: intravenous group, Group II: topical group, Group III: non-tranexamic acid group). To evaluate the effectiveness of tranexamic acids, the total amount of postoperative blood loss, postoperative hemoglobin loss, and volume of red blood cell transfusion in the three groups were compared.Results:
The total amount of postoperative blood loss was lower in the tranexamic acid administered group than in the non-tranexamic acid group (1,366±866 ml). Among the administration methods, the intravenous group (987±449 ml) was significantly lower than the topical group (1,136±339 ml) (p=0.004). Postoperative hemoglobin loss was lower in the tranexamic acid group than the non-tranexamic acid group.Among the administration methods, the intravenous group was lower than the topical group. The transfusion rate was higher in the non- tranexamic acid group (5.7%) than the tranexamic administered group. The transfusion rate of the intravenous group was 1.4%, and no patient required a transfusion postoperatively in the topical group. The number of postoperative thromboembolic events, as a complication of tranexamic acid, was similar in the three groups.
Conclusion: Tranexamic acid was effective in reducing postoperative blood loss after primary total knee arthroplasty compared to the non-
tranexamic acid administered group. No significant difference in the complications induced by tranexamic acid was observed among the three groups.Key words: primary total knee arthroplasty, tranexamic acid, blood loss
있겠다.2-5) 일차 슬관절 전치환술 후 수혈은 감염 및 급성 전신반 응, 사망과 같은 위험과 관련이 있고, 수술 후 수혈을 받은 환자들 은 재활시간과 입원기간을 연장하고 환자의 비용을 증가시키는 단점이 있다.6-9) 따라서 수술 후 출혈량을 줄이기 위한 많은 연구 가 있어 왔고, 여러 가지 방법이 소개되었다.10-14) 그 중에서도 효 과적인 방법 중 하나는 항섬유용해제로 작용하여 출혈량을 줄이 는 트라넥삼산을 사용하는 것이다.15-18) 트라넥삼산의 일차적 슬 관절 전치환술 중 사용은 경구 투여, 국소 투여, 정맥 투여, 혹은 2가지 투여 방법을 혼합해 환자에게 투여되는데, 지금까지 많은 연구에도 불구하고 어느 방법으로 어느 정도의 용량을 사용하였 을 때 수술 후 가장 출혈량을 줄일 수 있는지에 대한 보고는 논문 마다 상이하다.19,20) 이에 저자들은 트라넥삼산의 사용이 출혈량 을 줄이는 데 효과가 있을 것이라 전제하고, 정맥 내 투여 군과 관 절 내 투여 시 투여하지 않은 군과 비교하여 출혈량 및 헤모글로 빈 감소가 트라넥삼산을 사용한 그룹에서 더 낮을 것이라 가정하 였다.
대상 및 방법
1. 연구 대상 및 방법 1) 연구 대상
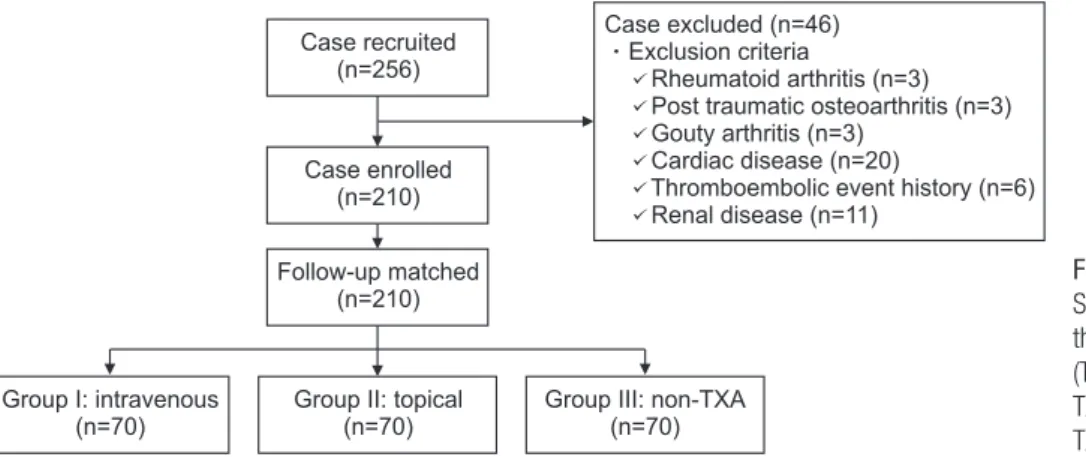
이 연구는 광주보훈병원에서 1명의 정형외과 의사에게 2017년 3월부터 2019년 2월까지 일차 슬관절 전치환술 수술을 시행 받 은 256명의 환자들을 대상으로 이루어졌다. 이들 중 기저질환으 로 류마티스 관절염, 통풍성 관절염, 심혈관질환자(심방세동 및 관상동맥 질환자, 혈전색전의 과거력이 있는자), 신장질환이 있 는 자는 제외 하였다(Fig. 1). 이 기준에 근거하여 총 46명의 환 자를 제외하였으며, 정맥 내 트라넥삼산을 사용한 그룹 70명 (Group I), 관절 내로 트라넥삼산을 사용한 환자 군 70명(Group II), 트라넥삼산을 사용하지 않은 그룹 70명(Group III)에 대해서 후향적 비교 연구를 시행하였다. 본 연구는 광주보훈병원의 연구 윤리 심의 위원회의 승인을 받고 시행되었다(#IRB number: 인
간 2019-18차 3호).
2) 수술 전후 관리, 수술 술기 및 트라넥삼산 투여 방법
모든 환자들은 전신 마취하에 수술을 시행하였으며, 수술 중 지 혈대의 압력은 280 mmHg로 동일하게 진행되었다. 모든 수술은 전방 정중 피부 절개 및 슬개내연 도달법으로 시행하였다. 트라 넥삼산의 정맥 내 투여 군은 지혈대를 승압하기 10–12분 전 트 라넥삼산 500 mg (tranexamic acid; Shin Poong Pharm. Co., Ansan, Korea)을 생리식염수 15 ml와 혼합하여 투여하였고, 수 술 부위 봉합 도중 지혈대를 감압하기 10–12분 전 트라넥삼산 500 mg을 생리 식염수 15 ml와 혼합하여 정맥 내 재투여하였다.
트라넥삼의 관절 내 투여 군은 수술 부위 봉합 직후 배액관을 통 해 지혈대 감압 직전 1,000 mg을 생리 식염수 20 ml와 혼합하여 투여하였으며, 나머지 군은 수술 전후에 트라넥삼산을 사용하지 않았다. 모든 군에서 수술 직후부터 이후 약 3시간 동안은 배액관 의 압력을 음압이 아닌 중립으로 유지하였고, 수술 후 3일째 모든 환자의 배액관은 제거하였다.
2. 임상적 평가 1) 수혈 기준
수혈 기준은 수술 후 혈색소 수치가 7.0 mg/dl 이하일 때 시행하 였으나 혈색소 수치가 7.0 mg/dl 초과일지라도 저혈압, 어지러 움, 빈맥이나 창백 등의 빈혈 증상을 보이는 환자에서는 수혈을 시행하였다. 수혈을 시행한 환자에 대해서는 농축 적혈구 2팩(총 800 ml)을 투여하였으며, 1회 이상 수혈을 시행한 환자는 없었 다.
2) 실혈량의 평가
본 연구에서는 정확한 실혈량을 평가하기 위해 Nadler 등,21) Sehat 등22)의 공식을 사용하여 환자의 키, 체중 및 성별에 따라 수술 전 총 혈액량을 계산하고 혈색소 수치의 변화에 따른 총 실 혈량을 측정하였다. 공식은 1. Patient blood volume (PBV)=
Case excluded (n=46) Exclusion criteria
Rheumatoid arthritis (n=3) Post traumatic osteoarthritis (n=3) Gouty arthritis (n=3)
Cardiac disease (n=20)
Thromboembolic event history (n=6) Renal disease (n=11)
Follow-up matched (n=210) Case recruited
(n=256)
Case enrolled (n=210)
Group III: non-TXA (n=70) Group I: intravenous
(n=70)
Group II: topical (n=70)
Figure 1. CONSORT (Consolidated Standards of Reporting Trials) diagram for the present trial. Group I, tranexamic acid (TXA) administered intravenously; Group II, TXA administered topically; Group III, non- TXA group.
K1×height (m2)+K2×weight (kg)+K3, 남성: K1=0.3669, K2=0.03219, K3=0.6041/여성: K1=0.3561, K2=0.03308, K3=0.1833); 2. Total red blood cell (RBC) volume loss=PBV
×(수술 전 hematocrit [Hct]-수술 후 Hct); 3. Total blood vol- ume loss=Total RBC volume loss/average Hct 순으로 계산하 였다.
3) 수술 후 발생한 합병증의 평가
수술 후 종아리 통증 호소하는 환자나 오목부종을 보이는 환자 에 한해서 도플러 초음파를 이용하여 심부 정맥 혈전증을 진단하
였으며, 호흡 곤란이나 가슴 불편감을 보이는 환자에 한해서 가 슴 컴퓨터 단층 촬영(조영제 투여)을 시행하여 폐동맥 색전증을 진단하였다. 또한 C-반응 단백질, 백혈구, 적혈구 침강 속도가 술 후 2주가 지나도 정상 범위에 속하지 않으면서 발적 및 종창이 심하여 감염이 의심되는 환자에 한해 핵의학 검사, 무릎 컴퓨터 단층 촬영 및 관절 천자를 시행하여 인공관절 주위 감염을 진단 하였다.
3. 통계분석
모든 자료는 평균±표준편차로 표현하였고, IBM SPSS Statistics
Table 1. Demographic Data and Preoperative Characteristics
Characteristic Group I Group II Group III p-value
Number of patients 70 70 70 -
Age (yr) 73.76±6.15 71.82±6.93 73.53±7.14 0.181
Sex (male/female) 34/36 32/38 39/31 0.512
BMI (kg/m²) 26.50±3.74 26.44±3.45 25.54±3.83 0.227
Preoperative Hb (g/dl) 12.62±1.32 12.41±1.94 12.54±1.41 0.764
Preoperative Hct (%) 38.09±3.56 37.44±5.07 37.91±3.96 0.681
Postoperative Hct (%) 29.46±3.15 28.19±4.05 28.71±3.67 0.12
Preoperative PT (s) 12.10±1.51 11.71±1.05 11.76±0.93 0.194
PT (INR) 1.04±0.10 1.03±0.06 1.06±0.12 0.259
Preoperative aPTT (s) 33.91±5.00 34.33±3.27 33.89±2.52 0.663 Preoperative blood volume (ml) 3,495.17±413.41 3,455.92±387.00 3,380.16±401.48 0.228 Values are presented as number only or mean±standard deviation. Group I, intravenously; Group II, intra-articular; Group III, controlled; BMI, body mass index; Hb, hemoglobin; Hct, hematocrit; PT, prothrombin time; INR, international normalized ratio; aPTT, activated partial thromboplastin time; -, not available.
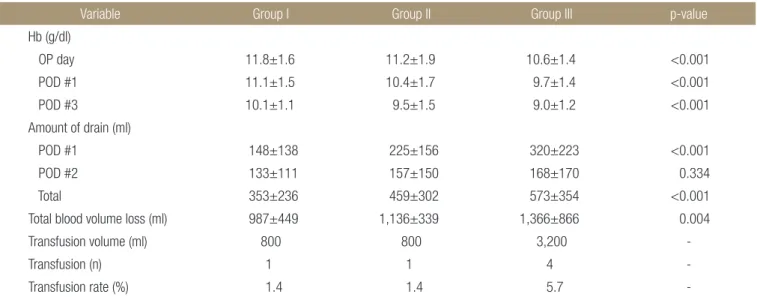
Table 2. Comparison of Blood Loss Volume and Transfusion among the Groups
Variable Group I Group II Group III p-value
Hb (g/dl)
OP day 11.8±1.6 11.2±1.9 10.6±1.4 <0.001
POD #1 11.1±1.5 10.4±1.7 9.7±1.4 <0.001
POD #3 10.1±1.1 9.5±1.5 9.0±1.2 <0.001
Amount of drain (ml)
POD #1 148±138 225±156 320±223 <0.001
POD #2 133±111 157±150 168±170 0.334
Total 353±236 459±302 573±354 <0.001
Total blood volume loss (ml) 987±449 1,136±339 1,366±866 0.004
Transfusion volume (ml) 800 800 3,200 -
Transfusion (n) 1 1 4 -
Transfusion rate (%) 1.4 1.4 5.7 -
Values are presented as mean±standard deviation, number only, or percent only. Group I, intravenously; Group II, intra-articular; Group III, controlled;
Hb, hemoglobin; OP, operation; POD, postoperative day; -, not available.
ver. 23.0 (IBM Corp., Armonk, NY, USA) 소프트웨어를 이용 하여 p-value 값이 0.05 미만인 경우를 통계적으로 유의하다고 간주하였다. 결과 값을 도출하기 위해 통계적으로 등분산성을 만 족하는 경우에는 analysis of variance (ANOVA)를 사용하였으 며, 등분산성을 만족하지 않은 경우에는 Welch’s t-test를 통해 검정하였다. 또한 p-value가 0.05보다 작은 경우 사후분석을 하 였으며, 등분산성을 만족하는 경우에는 turkey’s HSD (honest significant difference) test를 사용하였으며, 등분산성을 만족 하지 않은 경우에는 Dunnett-T3 test를 통해 검정하였다. 각 그 룹 간의 합병증 발생률에 대해 통계적으로 유의한 차이가 있는지 확인하기 위해 Fisher exact test를 시행하였다.
결 과
이들 환자 군들의 수술 전 차이는 ANOVA test를 이용하여 검정 하였으며, 통계적으로 유의한 차이는 없었다(Table 1). 일차 슬 관절 전치환술 후 총 실혈량은 관절 내 투여 군(Group II 1,136
±339 ml) 및 트라넥삼산을 사용하지 않은 군(Group III 1,366
±866 ml)보다 정맥 내 투여 군(Group I 987±449 ml)에서 더 낮았다(p=0.004). 수술 전 헤모글로빈(Group I 12.62±1.32 g/
dl, Group II 12.41±1.94 g/dl, Group III 12.54±1.41 g/dl) 은 그룹 간 차이가 없었으나(p=0.764), 수술 후 당일 헤모글로빈 (Group I 11.9±1.6 g/dl, Group II 11.2±1.9 g/dl, Group III 10.6±1.4 g/dl)과 수술 3일 후 헤모글로빈(Group I 10.1±1.1 g/dl, Group II 9.5±1.5 g/dl, Group III 9.0±1.2 g/dl)은 유의 한 차이를 보였다(p<0.001) (Table 2). 수혈 빈도는 트라넥삼산 을 사용하지 않은 군(Group III)에서 4예(5.7%)로 트라넥삼산을 혈관 내로 사용한 군(Group I)에서의 1예(1.4%)보다 더 높았으나 사용 방법에 따른 큰 차이는 없었다. 수술 후 합병증의 빈도는 트 라넥삼산을 관절 내 투여한 군(Group II)에서 심부 정맥 혈전증 1예(Fig. 2) 및 트라넥삼산을 사용한 각각의 군(Group I, Group II)에서 폐 색전증이 1예(Fig. 3)씩 진단되었으나, 그룹 간 통계적 으로 유의한 결과는 없었다(Table 3).
고 찰
수술 시 위험도의 증가와 관련 있는 동반 질환은 피할 수 없기 때 문에 수술 중이나 수술 후에 발생하는 출혈량의 감소시키는 것은 일차 슬관절 전치환술의 성공적인 결과와 관련이 있다.3) 술 후 빈 혈은 수혈의 가장 많은 이유 중 하나이다.6) 미국 혈액은행협회에 서는 체내 혈액이 부족할 경우 합병증의 발생이 높아 이를 막기 위해 혈색소가 7 g/dl 이하이거나 심혈관 질환이 있는 환자에서 는 8 g/dl 이하일 경우 수혈을 권고하고 있다.8) Lotke 등2)의 연구 에서 일차 슬관절 전치환술 환자에서 1,518 ml의 평균 혈액 손실 이 보고되었으며, 이는 슬관절 전치환술 후 수혈의 필요성 증가
3
4
5 M3 M3
+9.6
9.6 cm/s 1
2 0
X3
Figure 2. Deep vein thrombosis was diagnosed using Doppler sonography.
Figure 3. Pulmonary thromboembolism was diagnosed using chest computed tomography (enhanced).
Table 3. Comparison of the Postoperative Complications among the Groups
Variable Group I Group II Group III
DVT - 1 -
PTE 1 1 -
Infection - - -
Mortality - - -
Cerebral infarction - - -
Group I, intravenously; Group II, intra-articular; Group III, controlled; DVT, deep vein thrombosis; PTE, pulmonary thromboembolism; -, not available.
와 관련이 있다. 이에 일차 슬관절 전치환술 후 대규모 혈액 손실 과 관련된 합병증을 줄이기 위해 노력하고 있으며, 출혈을 줄이 기 위한 다양한 방법들 중에서 트라넥삼산의 사용이 효과적인 방 법 중 하나로 성공적인 결과를 보여준다.1,4,5) 하지만 지금까지 많 은 연구에도 불구하고 어느 방법으로 어느 정도의 용량을 사용하 였을 때 수술 후 가장 효과적이었냐는 부분에 대해서는 논문마다 의견이 상이하다.23) Wei 등24)은 일차 슬관절 전치환술 시 지혈대 감압 전 트라넥삼산을 10 mg/kg을 정맥 내 투여 시와 수술 부위 에 국소적으로 1.0 g 트라넥삼산을 생리식염수 50 ml와 혼합하 여 사용하였을 경우 혈액 손실에서 유의한 차이를 보이지는 않 았으나 혈색소 감소가 정맥 내 투여 시 2.8±0.7 mg/dl이며, 국 소 투여 시 2.7±0.6 mg/dl로 보고하였다. 저자들의 경우 혈관 내 투여가 실혈량이 적었으며, 이는 수술 전, 후 각각 주사를 투여 한 점이 출혈을 줄이는 데 도움이 되었을 것으로 생각된다. Pitta 등25)은 정맥 내로 트라넥삼산을 투여할 시 투여하지 않았던 군에 비해 9.4%의 혈액 손실이 감소되었다고 발표하였다. 다른 방법으 로 Ishida 등26)은 트라넥삼산을 국소 투여했을 때 혈색소 수치 감 소 및 슬관절 종창을 줄일 수 있다고 발표하였다.
본 연구의 결과로는 정맥으로 사용한 군의 평균 혈액 손실 감 소는 수술 후 약 987±449 ml, 관절 내 투여 군의 평균 혈액 감 소는 수술 후 1,136±339 ml을 보여 주었으며, 트라넥삼산을 사 용하지 않는 군에 대해서는 수술 후 약 1,366±866 ml의 혈액 손실을 보여주었다. 따라서 본 연구의 가장 중요한 발견은 일차 슬관절 전치환술 시 트라넥삼산을 사용하지 않는 군에 비해 정맥 내 투여 군, 관절 내 투여 군에서의 출혈량이 유의하게 감소되는 것이며, 그 중에서도 정맥 내 투여 군이 관절 내 투여 군보다 출혈 량을 줄이는 데 더 효과적임을 보여주었다.
유사하게 Tanaka 등27)도 트라넥삼산을 사용하지 않은 그룹에 비해 트라넥삼산을 1–2회 정맥 내 투여한 환자에서 혈액 손실 및 수혈 빈도를 현저하게 감소시키는 것으로 보고하였고, Orpen 등28)의 연구에서도 지혈대를 적용하기 10분 전 트라넥삼산을 정 맥 주사하면 수술 후 초기 혈액 손실을 줄이는 데 효과적이었다 고 보고하였다.
하지만 트라넥삼산 사용의 합병증으로 대두되는 혈전 색전증 위험성 때문에 사용을 주저하는 경우가 많으나 최근 보고에서는 일차 슬관절 및 고관절 전치환술 시 트라넥삼산 사용의 상대 위 험도(relative risk)는 심부 정맥 혈전증이 0.98, 폐색전증이 1.01, 뇌졸증이 0.86으로 발표하였다.29) 수술 시행 시 그러나 바늘 흡입 및 약물 희석 동안 박테리아 오염으로 인한 인공 삽입물 감염의 이론적 위험이 증가하는 것은 불가피하였으며, Kłak 등30)은 트라 넥삼산이 포도상구균 패혈증 관절염 발생 및 패혈증을 악화시킬 수 있는 방법이 될 수 있다고 보고하였다.
본 연구의 결과에 따르면, 감염률은 모두 0명이었으나 이는 표 재성 감염을 제외한 결과이며 트라넥삼산의 관절 내 투여 군에서
총 3명의 표재성 감염이 일어났다. 이 3명의 환자에서는 수술적 처치 없이 정맥 항생제 6주 사용 후 모두 완치되었다. 또한 트라 넥삼산의 정맥 내 투여의 전신 합병증으로 우려되는 혈전 색전증 은 오히려 관절 내 투여 군에서 더 많았으며, 이는 표본이 작아 유 의하지 않더라도 정맥 내 투여 군과 국소 투여 군의 합병증 발생 률은 크게 차이가 없음을 보여준 것이다.
본 연구가 갖는 제한점은 전체적인 표본수가 적으며, 환자 퇴 원 후에 발생했던 합병증에 대한 추시는 전 환자에서 이루어지지 않았다는 점이다. 또한 표재성 감염은 수술 후 감염률에 포함하 지 않았다.
결 론
일차 슬관절 전치환술 시행 시 트라넥삼산을 사용한 환자 군에서 사용한지 않은 군에 비해 총 실혈량을 유의하게 감소시켰고, 관 절 내 투여보다는 정맥 내로 투여하는 것이 실혈량의 감소 면에 서 더 효과적이었다. 정맥 내 투여로 인한 합병증은 관절 내 투여 및 트라넥삼산을 사용하지 않은 군과 비교해 유의한 차이는 없었 으나 표본 수의 부족 및 연구 계획에 편견이 작용할 수 있었다는 점을 감안하면 향후 추가적인 연구가 필요할 것으로 생각한다.
CONFLICTS OF INTEREST
The authors have nothing to disclose.
ORCID
Hyun Ju Lee, https://orcid.org/0000-0002-1696-0976 Ki Yong An, https://orcid.org/0000-0003-3583-6425 Ji Yeon Park, https://orcid.org/0000-0001-5639-7877 Young Woo Chung, https://orcid.org/0000-0001-9929-6769
REFERENCES
1. Huang ZY, Pei FX, Ma J, et al. Comparison of three different tourniquet application strategies for minimally invasive total knee arthroplasty: a prospective non-randomized clinical tri- al. Arch Orthop Trauma Surg. 2014;134:561-70.
2. Lotke PA, Faralli VJ, Orenstein EM, Ecker ML. Blood loss after total knee replacement. Effects of tourniquet release and continuous passive motion. J Bone Joint Surg Am.
1991;73:1037-40.
3. Su EP, Su S. Strategies for reducing peri-operative blood loss in total knee arthroplasty. Bone Joint J. 2016;98(1 Suppl
A):98-100.
4. Ishii Y, Noguchi H, Sato J, Tsuchiya C, Toyabe S. Effect of a single injection of tranexamic acid on blood loss after prima- ry hybrid TKA. Knee. 2015;22:197-200.
5. Xie J, Ma J, Yao H, Yue C, Pei F. Multiple boluses of intrave- nous tranexamic acid to reduce hidden blood loss after pri- mary total knee arthroplasty without tourniquet: a random- ized clinical trial. J Arthroplasty. 2016;31:2458-64.
6. McEvoy MT, Shander A. Anemia, bleeding, and blood trans- fusion in the intensive care unit: causes, risks, costs, and new strategies. Am J Crit Care. 2013;22(6 Suppl):eS1-13; quiz eS14.
7. Benoni G, Fredin H. Fibrinolytic inhibition with tranexamic acid reduces blood loss and blood transfusion after knee ar- throplasty: a prospective, randomised, double-blind study of 86 patients. J Bone Joint Surg Br. 1996;78:434-40.
8. Carson JL, Guyatt G, Heddle NM, et al. Clinical practice guidelines from the AABB: red blood cell transfusion thresh- olds and storage. JAMA. 2016;316:2025-35.
9. Hiippala S, Strid L, Wennerstrand M, et al. Tranexamic acid (Cyklokapron) reduces perioperative blood loss associated with total knee arthroplasty. Br J Anaesth. 1995;74:534-7.
10. Karam JA, Bloomfield MR, DiIorio TM, Irizarry AM, Shar- key PF. Evaluation of the efficacy and safety of tranexamic acid for reducing blood loss in bilateral total knee arthroplas- ty. J Arthroplasty. 2014;29:501-3.
11. Chen S, Li J, Peng H, Zhou J, Fang H, Zheng H. The influ- ence of a half-course tourniquet strategy on peri-operative blood loss and early functional recovery in primary total knee arthroplasty. Int Orthop. 2014;38:355-9.
12. Aggarwal AK, Shashikanth VS, Marwaha N. Platelet-rich plasma prevents blood loss and pain and enhances early functional outcome after total knee arthroplasty: a prospec- tive randomised controlled study. Int Orthop. 2014;38:387- 95.
13. Dong Z, Han L, Song Y, Qi J, Wang F. Hemostatic techniques to reduce blood transfusion after primary TKA: a meta-anal- ysis and systematic review. Arch Orthop Trauma Surg.
2019;139:1785-96.
14. Panni AS, Cerciello S, Vasso M, Del Regno C. Knee flexion after total knee arthroplasty reduces blood loss. Knee Surg Sports Traumatol Arthrosc. 2014;22:1859-64.
15. Park JH, Rasouli MR, Mortazavi SM, Tokarski AT, Maltenfort MG, Parvizi J. Predictors of perioperative blood loss in total
joint arthroplasty. J Bone Joint Surg Am. 2013;95:1777-83.
16. Zhao-Yu C, Yan G, Wei C, Yuejv L, Ying-Ze Z. Reduced blood loss after intra-articular tranexamic acid injection during total knee arthroplasty: a meta-analysis of the litera- ture. Knee Surg Sports Traumatol Arthrosc. 2014;22:3181-90.
17. Lee GC, Kim DH, Lee JW, Kang SW, Cho SW. Comparison of blood loss between intra-articular and intravenous tranexam- ic acid following primary total knee arthroplasty. J Korean Orthop Assoc. 2018;53:152-8.
18. Bezwada HR, Nazarian DG, Henry DH, Booth RE Jr, Mont MA. Blood management in total joint arthroplasty. Am J Or- thop. 2006;35:458-64.
19. Lee SY, Chong S, Balasubramanian D, Na YG, Kim TK. What is the ideal route of administration of tranexamic acid in TKA? A randomized controlled trial. Clin Orthop Relat Res.
2017;475:1987-96.
20. Dai WL, Zhou AG, Zhang H, Zhang J. Most effective regimen of tranexamic acid for reducing bleeding and transfusions in primary total knee arthroplasty: a meta-analysis of random- ized controlled trials. J Knee Surg. 2018;31:654-63.
21. Nadler SB, Hidalgo JH, Bloch T. Prediction of blood volume in normal human adults. Surgery. 1962;51:224-32.
22. Sehat KR, Evans R, Newman JH. How much blood is really lost in total knee arthroplasty? Correct blood loss manage- ment should take hidden loss into account. Knee. 2000;7:151- 5.
23. White CC 4th, Eichinger JK, Friedman RJ. Minimizing blood loss and transfusions in total knee arthroplasty. J Knee Surg.
2018;31:594-9.
24. Wei W, Dang S, Duan D, Wei L. Comparison of intravenous and topical tranexamic acid in total knee arthroplasty. BMC Musculoskelet Disord. 2018;19:191.
25. Pitta M, Zawadsky M, Verstraete R, Rubinstein A. Intrave- nous administration of tranexamic acid effectively reduces blood loss in primary total knee arthroplasty in a 610-patient consecutive case series. Transfusion. 2016;56:466-71.
26. Ishida K, Tsumura N, Kitagawa A, et al. Intra-articular injec- tion of tranexamic acid reduces not only blood loss but also knee joint swelling after total knee arthroplasty. Int Orthop.
2011;35:1639-45.
27. Tanaka N, Sakahashi H, Sato E, Hirose K, Ishima T, Ishii S.
Timing of the administration of tranexamic acid for maxi- mum reduction in blood loss in arthroplasty of the knee. J Bone Joint Surg Br. 2001;83:702-5.
28. Orpen NM, Little C, Walker G, Crawfurd EJ. Tranexamic acid reduces early post-operative blood loss after total knee arthroplasty: a prospective randomised controlled trial of 29 patients. Knee. 2006;13:106-10.
29. Goldstein M, Feldmann C, Wulf H, Wiesmann T. Tranexam-
ic acid prophylaxis in hip and knee joint replacement. Dtsch Arztebl Int. 2017;114:824-30.
30. Kłak M, Anäkkälä N, Wang W, et al. Tranexamic acid, an in- hibitor of plasminogen activation, aggravates staphylococcal septic arthritis and sepsis. Scand J Infect Dis. 2010;42:351-8.
일차 슬관절 전치환술 중 트라넥삼산의 정맥 내 투여와 국소 사용의 효과에 관한 비교 연구
이현주 • 안기용 • 박지연 • 정영우
광주보훈병원 정형외과
목적:
일차 슬관절 전치환술을 받은 환자들에게서 트라넥삼산의 효능을 확인하고, 트라넥삼산의 정맥 내 사용 방법과 관절 내 투 여 군을 비교하여 어떤 방법이 혈액 손실 감소 효과가 더 있는지 알아보고자 하였다.대상 및 방법:
이 연구는 광주보훈병원에서 2017년 3월부터 2019년 2월까지 일차 슬관절 전치환술을 받은 환자들에 대한 후향적 연구이다. 단측 일차 슬관절 전치환술을 시행 받은 총 210명의 환자가 연구에 포함되었다. 트라넥삼산 사용 방법에 따라 각각 70 명의 환자들에 대해 3개의 그룹으로 나누었다(Group I: 정맥 내 투여 군, Group II: 관절 내 투여 군, Group III: 트라넥삼산을 사 용하지 않은 군). 그룹 간 수술 후 총 실혈량, 헤모글로빈 감소치, 수혈 단위를 비교하였다.결과:
총 실혈량은 관절 내 투여 군(1,136±339 ml) 및 트라넥삼산을 사용하지 않은 군(1,366±866 ml)보다 정맥 내 사용 군(987±449 ml)에서 더 낮았다(p=0.004). 수술 후 헤모글로빈의 손실 또한 정맥 내 사용 군(1.8 g/dl)에서 관절 내 투여 군(2.9 g/dl)이나 투여하지 않은 군(3.5 g/dl)보다 현저히 낮았다(p<0.01). 수혈 빈도는 트라넥삼산을 사용하지 않은 그룹(5.7%)에서 더 높았으며 정맥 내 사용 시 1.4%를 보이고, 관절 내 투여한 군에서 수혈을 받은 환자는 없었다. 혈전색전증의 발생 빈도는 그룹 간 통계적으 로 유의하지 않았다.
결론:
일차 슬관절 전치환술 시행 시 트라넥삼산을 사용한 환자 군에서 사용한지 않은 군에 비해 총 실혈량을 유의하게 감소시켰 고, 관절 내 투여보다는 정맥 내로 투여하는 것이 더 효과적이었다. 정맥 내 투여로 인한 합병증은 관절 내 투여 및 트라넥삼산을 사용하지 않은 군과 비교해 유의한 차이는 없었다.색인단어: 일차 슬관절 전치환술, 트라넥삼산, 혈액 손실
접수일 2020년 3월 5일 수정일 2020년 4월 27일 게재확정일 2020년 4월 29일 책임저자 정영우
62284, 광주시 광산구 첨단월봉로 99, 광주보훈병원 정형외과
TEL 062-602-6162, FAX 062-602-6936, E-mail ywchungos@bohun.or.kr, ORCID https://orcid.org/0000-0001-9929-6769
Copyright © 2021 by The Korean Orthopaedic Association
“This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.”
대한정형외과학회지:제 56권 제 2호 2021