Vol. 18, No. 1, 19-23, 2015
Corresponding author: Young Joon Kim, Department of Plastic and Reconstructive Surgery, Sanggye Paik Hospital, Inje University College of Medicine, 1342, Dongil-ro, Nowon-gu, Seoul 139-707, Korea Tel: 82-2-950-1048, Fax: 82-2-932-6373 E-mail: [email protected]
2 mm 두께의 Matriderm 인조진피을 사용한 동시 부분층 식피술의 가능성
이창렬ㆍ김준현
1ㆍ김영준
1고성 보건소, 1인제대학교 의과대학 상계백병원 성형외과
The Capacity of 2 mm Matriderm
Ⓡas a Dermal Substitute in Single Stage Skin Resurfacing
Chang Ryul Yi, M.D., Joon Hyon Kim, M.D.
1and Young Joon Kim, M.D., Ph.D.
1Goseong Community Health Center, Goseong, 1Department of Plastic and Reconstructive Surgery, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea
Purpose: Matriderm
Ⓡ is a highly porous dermal substitute consisting of a collagen matrix (collagen type I, III, and V) cross-linked to an elastin hydrolysate. The 1 mm thickness MatridermⓇ is used in a one-stage procedure. On the other hand, 2 mm thickness MatridermⓇ has been used in two- stage procedures in combination with split thickness skin grafts (STSG) for reconstruction as dermal substitute. To the best our knowledge, there is no case that reports the single stage procedure with 2 mm thickness MatridermⓇ. There are many expected advantages if a two-stage surgery could be performed by one-stage procedure as long as the result is guaranteed. The purpose of this study is to present capacity of 2 mm thickness MatridermⓇ as a dermal substitute in sin- gle stage skin grafting by the successful results of six cases.Methods: We performed this one-stage procedure in five pa-
tients instead of soft tissue reconstruction. Those patients were required soft tissue reconstruction after trauma injuries or radial forearm harvest as a donor site in the period be- tween 2011 and 2012. Five Patients were treated with a com- bination of STSG and 2 mm thickness MatridermⓇ solely.Three out of five patients who were injured by trauma got transplanted splint thickness skin that were range from 4/1000∼8/1000 inches (Table 1). Patients’ data were ana- lyzed retrospectively by chart review and patients interviews.
Each patient’s chart was reviewed for age, gender, type of in- jury, complications, final outcome and successful rates.
Results: The patient group consisted of 4 men and 1 woman
between ages of 5 and 70. The clinical results of these five treated patients concerning skin-quality and coverage of ex- posed soft tissue were very good. Using 2 mm thickness MatridermⓇ the wound could gain more dermal substitute compare to 1 mm thickness MatridermⓇ.
Conclusion: Matriderm
Ⓡ is a single-use three-dimensional matrix composed of native, structurally intact collagen fibrils and elastin for supporting dermal regeneration. In this study five patients with trauma injuries or radial forearm harvest as a donor site were treated with 2 mm thickness MatridermⓇ as a dermal substitute and STSG as a single-stage procedure to cover exposed structures. Compare to 1 mm MatridermⓇ, 2 mm thickness MatridermⓇ provide more dermal collagen and enhance skin-elastisity. Achieving single stage STSG with 2 mm thickness MatridermⓇ, patient’s hospital days were reduced in half and infection chances were also de- creased. In conclusion, single skin grafting with 2 mm thickness MatridermⓇ is feasible and it is time-effient and cost effective procedure. (J Korean Burn Soc 2015;18:19 -23)Key Words: Dermal substitute, Matriderm, Skin graft
INTRODUCTION
Matriderm
Ⓡis a highly porous dermal substitute con-
sisting of a collagen matrix (collagen type I, III, and V)
cross-linked to an elastin hydrolysate
1). Since evaluation
in several trials by Van Zujlen, this collagen-elastin matrix
has been used as dermal substitute and showed sufficient
survival and successful result
1-15). Because of concerning
about take rates and the distance between wound bed
and skin graft, the 1 mm thickness Matriderm
Ⓡis pre-
ferred the 2 mm thickness Matriderm
Ⓡin reconstructive
surgery. When the 2 mm thickness Matriderm
Ⓡwas
needed, it has been applied in two-stage procedure in-
cluding additional skin graft. To the best our knowledge,
there is no case that reports the single stage procedure
with the 2 mm thickness Matriderm
Ⓡ. There are many ex-
pected advantages if a two-stage surgery could be per-
20
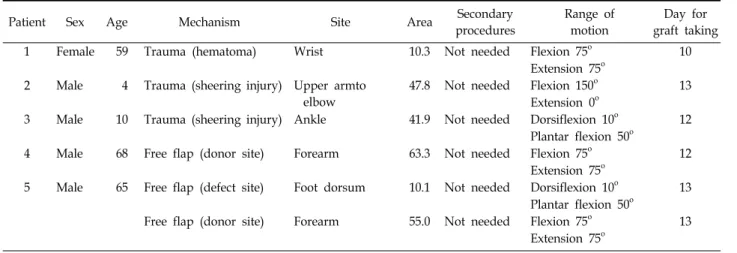
대한화상학회지 Vol. 18, No. 1, 2015Table 1. Data of Patients
Patient Sex Age Mechanism Site Area Secondary
procedures
Range of motion
Day for graft taking
1 Female 59 Trauma (hematoma) Wrist 10.3 Not needed Flexion 75o 10
Extension 75o 2 Male 4 Trauma (sheering injury) Upper armto
elbow
47.8 Not needed Flexion 150o 13
Extension 0o
3 Male 10 Trauma (sheering injury) Ankle 41.9 Not needed Dorsiflexion 10o 12
Plantar flexion 50o
4 Male 68 Free flap (donor site) Forearm 63.3 Not needed Flexion 75o 12
Extension 75o
5 Male 65 Free flap (defect site) Foot dorsum 10.1 Not needed Dorsiflexion 10o 13 Plantar flexion 50o
Free flap (donor site) Forearm 55.0 Not needed Flexion 75o 13
Extension 75o
formed by one-stage procedure as long as the result is
guaranteed. The purpose of this study is to present ca- pacity of 2 mm Matriderm
Ⓡas a dermal substitute in sin- gle stage skin grafting by the successful results of six cases.
PATIENTS AND METHODS
Data of patients admitted to our department were col- lected in the period between 2011 and 2012. Out of all the patients who required soft tissue reconstruction 5 pa- tients of 6 cases were treated with split thickness skin graft (STSG) and dermal substitute. 3 patients out of 5 pa- tients acquired the soft tissue defect after trauma. 2 pa- tients were needed to reconstruct the defect which re- sulted as a donor site or remnant defect site in the re- constructive surgery. Patients’ data were analyzed retro- spectively by chart review. Each patient’s chart was re- viewed for age, gender, mechanism of injury, complica- tions, final outcomes and success rates.
The authors were treated the 6 cases of 5 patients with defects in the combination of autologous STSG and 2 mm thickness Matriderm
Ⓡ(Dr Suwelack Skin and Health Care AG, Billerbeck, Germany) in a one-stage procedure.
The defects that the authors treated could only be re- constructed with local or free flap for coverage of the ex- posed structure like tendon and muscles. The wounds were debrided in full-thickness skin depth. Following de- bridement and hemostasis, the dermal matrices were ap- plied on the wound bed. Autologous STSG without mesh
were put on the dermal substitute and fixed by suture or surgical stapler. Then compressive dressing was per- formed with 0.9% saline soaked gauzes. The first change of the dressing was done 2nd or 3rd postoperative day.
Staples or suture were removed between 7 days and 10 days postoperatively.
The take-rate of STSG was defined as the percentage of the grafts that was considered to be vital and showed good adherence to the wound bed 2 weeks after surgery.
Wounds were considered as healed when more than 95%
of the grafted area was epithelialized. The necessity of re- grafting was regarded as an indicator of the success of the initial transplantation.
RESULTS
The patient group consisted of 1 female and 4 male be- tween the ages of 4 and 68. The mean area of defects was 38.1 cm
2(range 10.1∼63.3 cm
2)(Table 1). All the 6 cases in 5 patients needed only one grafting including dermal substitution with 2 mm thickness Matriderm
Ⓡfor a suc- cessful reconstruction. Thus the success rate was 100%.
The mean follow-up was 10.6 months (range 5∼19 months). The mean period for graft taken was 12.2 days.
All the patients were returned to daily life and work. The clinical photos of case (Patient 2) are presented in Fig. 1.
DISCUSSION
Since 2000 when Van Zuijlen et al. described about it,
Fig. 1. Clinical photos of case (Patient 2). (A) Preoperative photo shows full thickness skin loss and soft tissue defect on right foot and ankle. (B) After meticulous debridement, 2 mm thickness MatridermⓇ is applied over wound bed. (C) Split thickness skin graft with 8/1000 inch is applied over 2 mm thickness MatridermⓇ and fixed. (D) Clinical photo of patient at 6 months postoperatively.
the collagen-elastin matrix, Matriderm
Ⓡ, have been used in reconstructive surgery as dermal substitute.
2,3). This is a highly porous biodegradable three dimensional com- posed of native bovine collagen fiber I, II and V and coat- ed with elastin hydrolysate derived from bovine liga- mentum nuchae
3). Matriderm
Ⓡacts as a scaffold in the skin reconstitution and regulates scar formation
4). The question of whether to prefer a one-stage or a two- stage procedure in skin grafting with dermal substitute is subject of many discussions
5). A one-stage approach has to accept the disadvantage of the increased distance be- tween wound bed and the skin graft caused by the inter- posed dermal substitute for superior result
3,5,6). Otherwise the two-stage procedure can avoid diminished take rates but result poor outcome. Some prefer a one-stage proce- dure to prevent an additional surgery. In the case with lack of donor site a two-stage approach was able to delay grafting for several weeks
5,7). But the risk of wound in-
fection is always present and even increasing day by day when the wound coverage with skin graft is delayed for the infiltration of fibroblasts and capillaries from the wound bed to the scaffold
5). Great effort and care are needed for a long time to prevent the artificial dermis from infection and to keep it available. Though several methods have been known to prevent infection and in- crease the take rate of dermal substitutes, the cost remains as problem
5,8). Moreover the necessity of the loss of time for 2 or 3 weeks and an additional anesthesia was not acceptable when the alternatives with other applicable dermal substitutes for a one-stage procedure are availa- ble. In conclusion, whenever possible, use of dermal sub- stitute and coverage with skin graft should be performed in a one-stage.
Since several literatures by Van Zujlen, this colla-
gen-elestin matrix has been applied as one-stage dermal
substitute showing sufficient survival of skin graft on top
22
대한화상학회지 Vol. 18, No. 1, 2015of it
1-15). To the best of our knowledge, Matriderm
Ⓡis the only synthetic dermal substitute which can be applied with skin graft at one-stage procedure. Unlike allogenic dermal substitute, there is no concern about transmitted disease in use of synthetic material. And it may be easier to be supplied the raw materials.
But survival of the overlying skin graft could be at risk after dermal substitution
3,6). Dermal substitute may hinder vascular ingrowth and diffusion of nutrients by increas- ing the distance between wound bed and the graft
2,3,6). That is why the thickness of dermal substitute is impor- tant.
At the best our knowledge, this is the first trial that the 2-mm-thickness Matriderm
Ⓡis applied as dermal sub- stitute in a one-stage procedure of the skin grafting. There are many studies about Matriderm
Ⓡto evaluate the possi- bility and utility as dermal substitute in various types of wound
1-15). However there has not been any literature that mentioned the 2 mm thickness Matriderm
Ⓡas applicable and useful dermal substitute in skin grafting even in one-stage procedure. The authors recognized that 2 mm thickness Matriderm
Ⓡmay act as reliable dermal sub- stitute through the 6 cases of reconstructive surgery.
Moreover 2 mm thickness Matriderm
Ⓡshowed successful take rate and sufficient elasticity in joint movement. The regrafting was not required and no complication was ob- served in any cases.
This literature proves that the 2 mm thickness Matri- derm
Ⓡmay be applied in one-stage approach skin grafting. The thicker dermal substitute is expected to pro- vide superior skin elasticity, lower wound contracture rate and better aesthetic outcomes. But the absence of ob- jective evaluation including contracture rate, elasticity and pliability is the limitation of this article. Further eval- uation and long term follow up in large patient group must be needed.
CONCLUSION
Matriderm
Ⓡis a single-use three-dimensional matrix composed of native, structurally intact collagen fibrils and elastin for supporting dermal regeneration. In this study, 6 cases of soft tissue defect by traumas or flap harvest were successfully treated with 2-mm-thickness Matriderm
Ⓡand STSG in a single-stage procedure. Compared to the 1 mm thickness Matriderm
Ⓡ, the 2 mm thickness Matri- derm
Ⓡcan provide more dermal collagen and enhance skin-elasticity. Achieving single stage procedure, patient’s hospital days were reduced and infection chances were also decreased. In conclusion, single skin grafting with the 2 mm thickness Matriderm
Ⓡis feasible and it is time- efficient and cost effective procedure.
DISCLOSURE
This work was presented as a poster at the 2013 Con- gress of The Korean Burn Society on June 13∼14, 2013.
REFERENCES
1) Ryssel H, Radu CA, Germann G, et al. Single-stage MatridermⓇ and skin grafting as an alternative reconstruction in high- voltage injuries. Int Wound J. 2010;7:385-392.
2) Van Zuijlen PPM, van Trier AJM, Vloemans JFPM, et al. Graft survival and effectiveness of dermal substitution in burns and reconstructive surgery in a one-stage grafting model. Plast Reconstr Surg. 2000;106:615-623.
3) Cervelli V, Brinci L, Spallone D, et al. The use of MatridermⓇ and skin grafting in post-traumatic wounds. Int Wound J. 2011;
8:400-405.
4) Wetzig T, Gebhardt C, Simon JC. New indications for artificial collagen-elastin matrices? Covering exposed tendons. Derma- tology. 2009;219:272-273.
5) Haslik W, Kamolz LP, Nathschlöger G, et al. First experiences with the collagen-elastin matrix MatridermⓇ as a dermal subs- titute in severe burn injuries of the hand. Burns. 2007;33:
364-368.
6) Ryssel H, Gazyakan E, Germann G, et al. The use of MatridermⓇ in early excision and simultaneous autologous skin grafting in burns-A pilot study. Burns. 2008;34:93-97.
7) Dantzer E, Queruel P, Salinier L, et al. Dermal regeneration template for deep hand burns: clinical utility for both early grafting and reconstructive surgery. Br J Plast Surg. 2003;
56:764-774.
8) Heitland A, Piatkowski A, Noah EM, et al. Update on the use of collagen/glycosaminoglycate skin substitute-six years of experiences with artificial skin in 15 German burn centers.
Burns. 2004;30:471-475.
9) Pauchot J, Elkhyat A, Rolin G, et al. Dermal equivalents in oncology: benefit of one-stage procedure. Dermatol Surg.
2013;39:43-50.
10) Atherton DD, Tang R, Jones I, et al. Early excision and app- lication of Matriderm with simultaneous autologous skin grafting in facial burns. Plast Reconstr Surg. 2010;125:60-61.
11) Haslik W, Kamolz LP, Manna F, et al. Management of full-thickness skin defects in the hand and wrist region: first long-term experiences with the dermal matrix MatridermⓇ J Plast Reconstr Aesthet Surg. 2010;63:360-364.
12) Ryssel H, Germann G, Czermak C, et al. MatridermⓇ in depth-adjusted reconstruction of necrotising fasciitis defects.
Burns. 2010;36:1107-1111.
13) Greenwood JE, Mackie IP. Neck contracture release with Matriderm collagen/elastin dermal matrix. Eplasty. 2011;11:
137-151.
14) Cervelli V, Brinci L, Palla L, et al. Skin necrosis of scrotum
due to endovascular embolisation: a case report. Int Wound J. 2012;9:70-75.
15) Cervelli V, Lucarini L, Cerretani C, et al. The use of MatridermⓇ and autologous skin grafting in the treatment of diabetic ulcers: a case report. Int Wound J. 2010;7:291-296.
16) Riml S, Wallner H, Larcher L, et al. Aesthetic Improvements of Skin Grafts in Nasal Tip Reconstruction. Aesthetic Plast Surg. 2011;35:475-479.
17) Ryssel H, Germann G, Kloeters O, et al. Dermal substitution with MatridermⓇ in burns on the dorsum of the hand. Burns 2010;36:1248-1253.