서 론
스타틴은 혈중 저밀도지질단백(low density lipoprotein cholesterol, LDLC)과 심혈관질환의 위험도를 효과적으로 감소시키는 약물이다.
그러나 스타틴의 효과는 복약 순응도가 떨어짐에 따라 감소한다.1) 실 제 임상진료에서 임상의들이 스타틴을 지속적으로 처방하면서 추적 지질검사를 했을 때 LDLC 목표치에 도달하지 못하는 경우가 많다.
이런 상황은 임상의에게는 딜레마이다.2-5) 이때 임상의는 다음과 같 은 여러 상황을 고려한다. 첫째, 처방한 스타틴의 용량이 적은 경우, 둘째, 복용하는 스타틴 제재가 환자에게 반응이 좋지 않은 경우, 셋 째, 생활습관교정이 안 된 경우, 마지막으로 복약 순응도가 떨어지는 경우 등이다. 이때 임상의들은 기존에 복용하던 스타틴의 용량을 증 량시키거나 기존의 제재를 다른 제재로 대체하고 생활습관교정을 교육하기도 한다. 그러나 LDLC의 목표치에 도달하지 못하는 경우가
Original Article
고지혈증 환자군에서 스타틴 순응도 측정에 있어 모리스키 복약순응검사의 유용성
김재인, 김은정*, 김주혁, 오춘옥
부산보훈병원 가정의학과
Validity of Morisky Medication Adherence Scales in Assessment of Statin Adherence in Dyslipidemic Patients
Jane Kim, Eun-Jeung Kim*, Joo-Hyuk Kim, Chun-Ok Oh
Department of Family Medicine, Busan Veterans Hospital, Busan, KoreaBackground: Statins are potent drugs for lowering the levels of low density lipoprotein cholesterol (LDLC) and thus, preventing cardiovascular diseases.
However, their effectiveness is significantly compromised by inadequate dose, inadequate response, failure to make life style modifications, and medication non-adherence. With respect to poor adherence to medication, clinicians have to identify the adherence problem in a clinically relevant manner.
Methods: Seventy patients who were selected randomly completed the Morisky Medication Adherence Scale (MMAS) questionnaire. Four patients undergoing secondary prevention were excluded. Sixty patients were divided into two groups based on whether they achieved the LDLC goal. This prospective study examined the relationship between MMAS scores and LDLC goal achievement.
Results: The average age of the selected patients was 64.57 years, and 84.8% of them were men. Forty patients achieved their LDLC goal. T-test revealed that the patients who achieved the LDLC goal had significantly lower LDLC levels (79.03± 17.45 mg/dL vs. 118.81± 25.57 mg/dL, P< 0.001) and higher MMAS scores (3.43± 0.636 points vs. 2.42± 0.785 points, P< 0.001) than the patients who did not achieve their LDLC goal. Additionally, as per the results of the chi-square test, the goal achievers were more adherent than the non-achievers (odds ratio, 1.35; 95% confidence interval, 107.67-129.95; P= 0.002).
Conclusion: Medication non-adherence may be responsible for failure to achieve the LDLC goal in many patients who are prescribed statins. In routine clinical care, the structured MMAS questionnaire may prove to be an effective tool for clinicians to assess medication non-adherence.
Keywords: LDL Cholesterol Achievement; Medication Adherence; Statins; Treatment Failure
http://www.kafm.or.kr/kjfp.2015.5.3.332pISSN 2233-9019 · eISSN 2233-9116 Korean J Fam Pract. 2015;5(3):332-337
KJFP
Korean Journal of Family PracticeReceived February 3, 2015 Accepted August 28, 2015 Corresponding author Eun-Jeung Kim
Tel: +82-51-601-6067, Fax: +82-51-601-6339 E-mail: [email protected]
Copyright © 2015 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
김재인 외. 모리스키 복약검사의 유용성 Korean Journal of Family Practice
KJFP
Original Article
Korean Journal of Family Practice 환자의 복약 불순응 때문이라면 앞의 처치는 부적절하다.6-8) 이때 복
약 순응도를 확인하여야 한다. 그리고 임상의는 순응도 문제를 임상 적으로 간편하면서 적절한 방법으로 확인하는 것이 바람직하다.9)
순응도는 환자가 의사가 처방한 대로 약을 정확히 복용하는 정도 로 알려져 있다.10) 스타틴 복용군을 대상으로 했던 연구에서는 1년 후 약 절반 미만의 복용자들만이 약물복용에 순응하는 것으로 알려 졌다.11) 또 다른 연구에서는 스타틴을 10년 이상 복용 시 약 75% 정도 의 스타틴 복용자들이 복약에 순응하지 않는 것으로 보여졌다.12-14) 약국조제기록, 약 개수 확인, 전자장비 등을 이용한 복약 확인 등이 복약의 순응도를 확인하는 여러 연구에서는 널리 쓰여 왔고, 순응도 확인에 있어서 예측인자들로 사용되어지고 있다.15,16) 그러나 이러한 방법들은 일상적인 임상진료에서는 아직 활용도가 떨어지는 것으로 보여진다.17)
환자가 복약 순응도를 자가 보고하는 신속하고 검증된 바 있는 모 리스키 복약순응검사(Morisky Medication Adherence Scale, MMAS) 설문지는 실제 임상에서 LDLC의 목표치의 성취 정도와 연관 지어 연구되어 연관성이 높았다.7,18,19) MMAS는 이후 계속 다른 연구에서 보완된 형태로 사용되면서 복약 순응도를 측정하였다. 이런 연구결 과에서 타당성이 입증되었다.19) 또 스타틴 복용자를 대상으로 하지 않는 다른 연구들에서도 경구혈당강하제 복약 순응도와 당화혈색 소의 관계나 혈압강하제 복약 순응도와 혈압 측정과의 정도에 있어 서도 연관성이 있어 순응도 확인에 유용한 것으로 입증되었다.20)
환자의 약물에 대한 믿음이 환자의 복약순응 여부의 결정과 불순 응 시 이런 행태의 동기와 연관이 있다는 연구가 있다.21) 이 연구에서 일반적인 약물에 대한 환자의 믿음에 관한 설문지(Beliefs about Med- icines Questionnaire–general, BMQ-G)를 사용하였다. 그러므로 MMAS의 결과인 순응도를 BMQ-G와 연관 지어 연구할 시 이런 불 순응행태의 동기를 알고, 여기에 대한 해결방법을 찾을 수 있을 것으 로 보인다.22,23)
본 연구에서는 부산의 부산보훈병원 가정의학과 외래 환자들에
서 고지혈증과 심혈관질환의 일차 예방으로 스타틴을 복용하는 환 자들에서 복약 순응도를 MMAS 설문지를 통해 확인하였고, MMAS 점수와 LDLC 목표 성취도와의 정도를 연관 지었다. 그리하여 복약 순응도 측정에 대한 MMAS 유용성 여부를 고찰하였다. 또한 이후 전개될 연구를 위해 복약에 순응하는 행태의 동기를 BMQ-G로 파 악하여 MMAS 점수와 연관 지어 연구해 보고자 한다.
방 법
1. 연구대상
본 논문의 연구는 2014년 3월과 4월 무작위로 추출된 부산의 부산 보훈병원 가정의학과 외래에서 스타틴을 복용한 환자군 70명을 대 상으로 한 전향적 연구이다. 2차 예방대상인 협심증, 심근경색, 말초 동맥질환, 심혈관시술의 과거력을 가진 환자 4명은 배제하였으며, 심 혈관계 위험인자(당뇨, 고혈압, 이상지질혈증, 흡연)를 가진 환자 중 1 차 예방으로 스타틴을 복용하는 66명의 환자를 대상으로 하였다.
2. 연구방법
2014년 3월과 4월 외래 내원 환자에게 서론에서 밝힌 검증된 양식 의 설문지를 배포하고 작성을 거부한 11명의 환자를 제외한 70명의 환자를 추출하여 2014년 11월부터 내원 약 6개월 뒤의 혈액검사소견 을 관찰해 순응도와 LDLC의 목표성취도 사이의 관계를 목표 성취 군과 목표 미성취군으로 나누었다. 환자에 대한 내과적 병력, 임상검 사결과, 복약 중인 약, 심혈관계 위험인자, 통계학적 자료는 병원기록 을 참고하여 작성하였다. LDLC 목표성취 정도는 third report of Na- tional Cholesterol Education Program Adult Treatment Panel III에 따라 심혈관질환의 위험도에 따라 성취목표를 달리하여 정하였다.24)
환자에게 배포한 MMAS 설문지와 BMQ-G 설문지는 표에서 제시
Table 1. The MMAS*
Questionnaire Answer
1. Do you ever forget to take your medicine? Yes/ no 2. Are you careless at times about taking your medicine? Yes/ no 3. When you feel better do you sometimes stop taking your
medicines?
Yes/ no
4. Sometimes if you feel worse when you take the medicine, do you stop taking it?
Yes/ no
Negative answer to an MMAS question received of 1.
MMAS, Morisky Medication Adherence Scale.
*A 4-item questionnaire used to identify non-adherence patients and type of non-adherence.17)
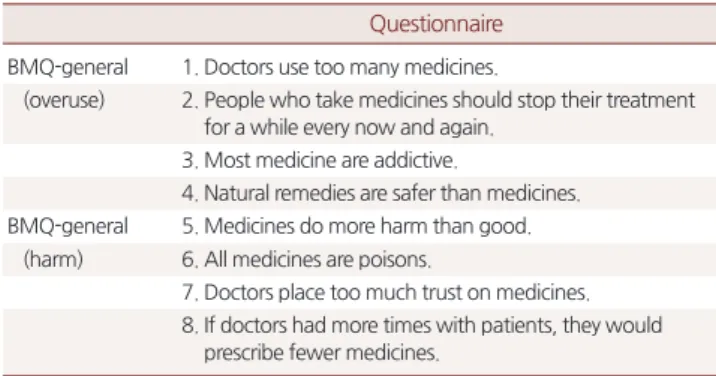
Table 2. BMQ-general*
Questionnaire BMQ-general 1. Doctors use too many medicines.
(overuse) 2. People who take medicines should stop their treatment for a while every now and again.
3. Most medicine are addictive.
4. Natural remedies are safer than medicines.
BMQ-general 5. Medicines do more harm than good.
(harm) 6. All medicines are poisons.
7. Doctors place too much trust on medicines.
8. If doctors had more times with patients, they would prescribe fewer medicines.
BMQ, Belief about Medicine Questionnaire.
*An 8-item questionnaire with Likert scale response (1=strongly disagree to 5= strongly agree).22)
Jane Kim, et al. Validity of Morisky Medication Adherence Scales
Korean Journal of Family Practice
KJFP
하였다(Tables 1, 2). MMAS 설문지는 모리스키에 의해 고안된 검증된 기본적 양식을 사용하였다.17) 이 양식을 선택한 이유는 본 연구의 대 상인 고령의 환자들에게 비교적 인지하기 쉬운 양식으로 되어있기 때문이다. BMQ-G 역시 기본적인 인지하기 쉬운 양식을 선택하였 다.22) 각 MMAS 설문지에 대한 부정적 대답은 1점으로 채점되었고, MMAS 설문지 4점을 순응도가 있는 것으로 보았다. 또한 순응도를 비의도적인 경우와 의도적인 경우로 분류하고 1번과 2번 문항을 비 의도적인 경우로 보고 3번과 4번을 의도적인 경우로 보고 분석하였 다. BMQ-G 설문지의 경우는 약물의 과용과 부작용에 의한 위해에 대한 환자의 인지형태로 나뉘어 구성돼 있다. 응답은 리커트(Likert) 형에 기반하여 1번(매우 아니다)에서 5번(매우 그렇다)로 나눠 작성 되었다. 최고 점수는 40점이었으며 점수가 높을수록 복약에 대해 인 식이 부정적인 것으로 평가됐다. 일차적인 연구결과는 이 연구에서 불순응의 정도와 형태이며 이차적인 연구결과는 LDLC과 순응도 사 이의 관계분석이다.
3. 통계분석
연속변수는 평균± 표준편차로 나타냈고, 범주형 변수는 빈도(%) 로 요약되었다. 정규분포를 이룬 연속변수는 독립 T검정으로 분석되 었다(양측 검정, α= 0.05). Chi-square 분석은 범주형 자료를 비교하는 데 사용되었다. MMAS 점수는 연속변수와 범주형 변수로 각각 나눠 져 분석되었다. 다변량회귀분석을 LDLC를 반응변수로 하여 연령,
나이, 수축기혈압, 확장기혈압, 신기능검사, 간기능검사, BMQ-G 점 수, MMAS 분석결과 중 완전 순응 여부와 연관 지어 분석하였다. 또 한 의도적 불순응, 비의도적 불순응을 LDLC 성취 여부와 관련하여 독립 T검정을 시행하여 분석하였다. 또한 BMQ-G 점수를 나이, 수축 기혈압, 확장기혈압, 지질단백, MMAS 점수와 연관 지어 단변량회귀 분석을 시행하였다. 모든 분석은 PASW SPSS ver. 18.0 (SPSS Inc., Chi- cago, IL, USA)으로 시행하였고 통계적 유의성 수준은 P값 0.05 미만 으로 정의하였다.
결 과
1. 연구대상의 일반적 특성
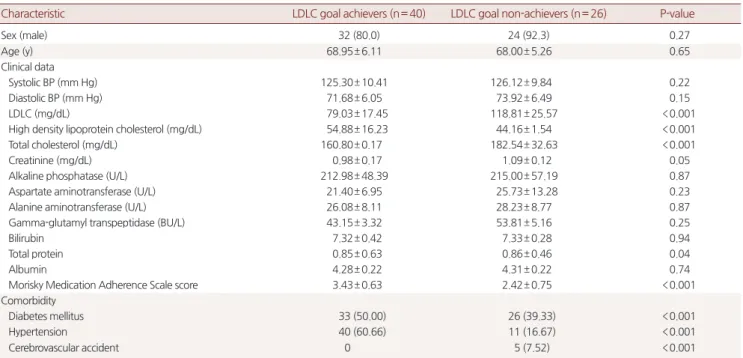
설문조사에 참여한 환자는 총 70명이었으나 심혈관질환의 2차 예 방을 배제한 기준에 따라 4명이 배제되었다. 환자의 평균 연령은 68.57세였으며, 부산보훈병원의 특성상 이 중 84.8%의 환자가 남성이 었다. 66명의 환자 중 40명의 환자는 LDLC 목표치에 도달하였고, 환 자들의 임상검사상의 특징, 통계학적 자료, 심혈관질환의 위험도와 관련된 주된 동반질환은 LDLC 목표 성취군과 LDLC 목표 미성취군 으로 나누어 제시하였다(Table 3).
2. Low Density Lipoprotein Cholesterol 목표 성취 여부
LDLC은 목표 성취군에서 목표 미성취군보다 유의하게 낮았다
Table 3. Characteristics of the 66 patients responding to questionnaire
Characteristic LDLC goal achievers (n= 40) LDLC goal non-achievers (n= 26) P-value
Sex (male) 32 (80.0) 24 (92.3) 0.27
Age (y) 68.95± 6.11 68.00± 5.26 0.65
Clinical data
Systolic BP (mm Hg) 125.30± 10.41 126.12± 9.84 0.22
Diastolic BP (mm Hg) 71.68± 6.05 73.92± 6.49 0.15
LDLC (mg/dL) 79.03± 17.45 118.81± 25.57 <0.001
High density lipoprotein cholesterol (mg/dL) 54.88± 16.23 44.16± 1.54 <0.001
Total cholesterol (mg/dL) 160.80± 0.17 182.54± 32.63 <0.001
Creatinine (mg/dL) 0.98± 0.17 1.09± 0.12 0.05
Alkaline phosphatase (U/L) 212.98± 48.39 215.00± 57.19 0.87
Aspartate aminotransferase (U/L) 21.40± 6.95 25.73± 13.28 0.23
Alanine aminotransferase (U/L) 26.08± 8.11 28.23± 8.77 0.87
Gamma-glutamyl transpeptidase (BU/L) 43.15± 3.32 53.81± 5.16 0.25
Bilirubin 7.32± 0.42 7.33± 0.28 0.94
Total protein 0.85± 0.63 0.86± 0.46 0.04
Albumin 4.28± 0.22 4.31± 0.22 0.74
Morisky Medication Adherence Scale score 3.43± 0.63 2.42± 0.75 <0.001
Comorbidity
Diabetes mellitus 33 (50.00) 26 (39.33) <0.001
Hypertension 40 (60.66) 11 (16.67) <0.001
Cerebrovascular accident 0 5 (7.52) <0.001
Values are presented as number (%) or mean± standard deviation.
LDLC, low density lipoprotein cholesterol; BP, blood pressure.
김재인 외. 모리스키 복약검사의 유용성 Korean Journal of Family Practice
KJFP
(79.03±17.45 mg/dL vs. 118.81± 25.57 mg/dL, P<0.001). LDLC 목표 성 취군에서는 목표 미성취군과 비교하였을 때 총 콜레스테롤(160.83±
0.17 mg/dL vs. 182.54±32.54 mg/dL, P<0.001), high density lipoprotein cholesterol (HDLC; 54.88±16.23 mg/dL vs. 44.16±1.54 mg/dL, P<0.001) 는 유의한 차이가 있었다, 이 외의 임상적 특징은 표에 제시되어 있다 (Table 3).
또한 LDLC 목표 성취군과 LDLC 목표 미성취군 사이에 MMAS 점 수는 연속변수로 하여 두 군에서 T검정으로 비교한 결과 순응도 측 정 여부와 관계없이 목표성취군에서 높게 나왔다(3.43± 0.636점 vs.
2.42± 0.785점, P<0.001). Chi-square 검정에서는 MMAS 점수 4점을 완전순응으로 본 순응도가 목표 성취군와 목표 미성취군에서 유의 한 차이가 있었다(odds ratio, 1.35; 95% confidence interval, 107.67- 129.95; P= 0.002) (Table 4). LDLC를 반응변수로 하여 다변량회귀분석 을 시행한 결과 총 콜레스테롤(P<0.001), HDLC (P<0.001)을 제외하 고는 의미 있는 결과는 없었다.
3. 순응도의 척도
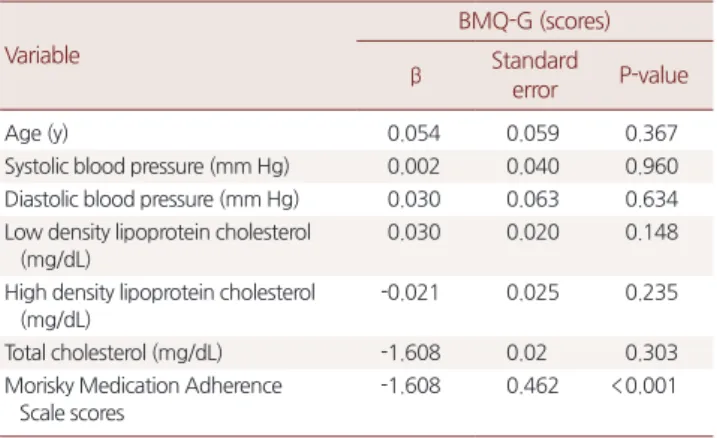
총 22명의 환자가 완전순응을 보였으며 불순응군 중 13명이 의도 적 불순응이었으며, 38명은 비의도적 불순응이며 5명은 의도적 불 순응과 비의도적 불순응 두 가지 경우 다 해당되었다. 완전순응인 경 우 유의한 차이가 있는 BMQ-G 점수(20.21± 2.14점 vs. 23.53± 2.81점, P= 0.002)를 보여 주었다. 그리고 BMQ-G 점수는 비의도적 불순응군 과 의도적 불순응군에서 유의한 차이를 보여주었다(22.17± 2.79점 vs. 24.23 ±3.49점, P<0.001). 다변량회귀분석결과 BMQ-G는 오직 MMAS 점수와 유의미한 관계가 있었다(P<0.001) (Table 5).
4. 제형과 순응도의 관계
본원 외래에서는 주로 atovastatin과 rosuvastatin을 처방했다. 연구 군에서 MMAS 4점을 완전순응으로 정의하고 chi-square 검정을 시 행한 결과, 완전순응군에서 atovastatin 복용자 15명(68.2%)과 rosuv- astatin 복용자 7명(31.8%)으로 atovastatin과 완전순응 간(P= 0.017), rosuvastatin과 완전순응 간(P= 0.017)으로 유의미한 차이가 있었다.
고 찰
스타틴은 심혈관질환의 위험을 낮추는 약물이나 순응도가 낮은 것으로 알려져 있다. 스타틴의 순응도 확인방법을 통한 여러 연구를 통하여 순응도에 영향을 미치는 인자들이 연구되어 왔다. 그러나 이 연구들에서 사용한 방법은 약국조제기록, 약 개수 확인, 전자장비를 이용한 복약 확인 등 순응도를 손쉽게 확인할 수 있는 방법이 아니었 다.15) 외래 환자에게 순응도를 신속하고 간편하게 확인하는 방법이 필요하다는 점에서 본 연구는 자가보고방법에 중점을 두고 고찰하 고자 한다.
MMAS는 모리스키가 고혈압 환자에서 혈압조절 여부와 투약의 순응도 사이의 관계를 측정하기 위해 고안된 자가보고 설문지이다.18) 여러 연구결과에서 이 자가보고방법이 타당성과 신뢰성이 입증되었
다.25,26) Cook 등27)의 연구에서도 타당성이 입증된 MMAS 검사결과
와 약국조제기록 사이 상관관계가 높은 것으로 나타났다. Berming- ham 등26)의 연구에서는 LDLC의 목표도달 여부와 MMAS 점수가 종 속적으로 연관성이 높은 것으로 나왔으며, 본 연구에서도 일치하였 다. 이러한 MMAS를 사용하는 순응도 측정은 임상적으로 유용성이 있는 것으로 보여진다. 그러므로 치료 실패 시 환자에게 MMAS를 통 해 외래에서 우선적으로 간단하게 순응도를 측정해 볼 수 있다고 보 여진다. 조직적으로 구성된 자가순응보고 설문지는 빠르고 싸며 외 래에서 의료진에 의해 간편하게 측정될 수 있다는 장점이 있다. 이 방 법은 약국조제기록, 약 개수 확인, 전자장비를 이용한 복약 확인보다 실제 임상에서 더 실용적일 수 있다.15) 이 방법은 역시 환자에게 외래 에서 직접 구두로 확인하는 방법보다 의사에게도 순응도 확인 여부 에 대한 자신감을 줄 수 있다.16)
이전 연구와 본 연구를 비교해 보았을 때 약간의 차이가 있다.
Afonso 등6)의 연구에서도 순응도가 높은 환자군에서 LDLC 목표 성 Table 4. Relationship between adherence and goal achievement
Variable Adherence
Partial (n= 44) Complete (n= 22)
Goal non-achiever 23 (34.4) 3 (4.5)
Goal achiever 21 (31.8) 19 (28.8)
Values are presented as number (%). Analyzed by chi-square test; significantly different by adherent group (P<0.001). Goal achiever: low density lipoprotein cholesterol goal achiever; partial adherence, MMAS scores≤ 3; complete adher- ence, MMAS scores= 4.
MMAS, Morisky Medication Adherence Scale.
Table 5. Related factors and BMQ-G scores Variable
BMQ-G (scores)
β Standard
error P-value
Age (y) 0.054 0.059 0.367
Systolic blood pressure (mm Hg) 0.002 0.040 0.960 Diastolic blood pressure (mm Hg) 0.030 0.063 0.634 Low density lipoprotein cholesterol
(mg/dL)
0.030 0.020 0.148
High density lipoprotein cholesterol (mg/dL)
-0.021 0.025 0.235
Total cholesterol (mg/dL) -1.608 0.02 0.303
Morisky Medication Adherence Scale scores
-1.608 0.462 <0.001
Analyzed by linear multiple regression.
BMQ, Belief about Medicine Questionnaire.
Jane Kim, et al. Validity of Morisky Medication Adherence Scales
Korean Journal of Family Practice
KJFP
취군이 더 많다고 하였다. Afonso 등6)은 본 연구와 달리 MMAS 점수 를 3점 이상부터 순응도가 있다고 보았다. Bermingham 등26)은 본 연 구와 같이 4점을 순응도가 있는 것으로 보았는데, 본 연구와 같이 많 은 경우의 의도적 불순응에서 MMAS 점수가 3점이었기 때문이다.
이 연구에 있어 설문지는 의료진이 없는 장소에서 환자에 의해 작성 되었으므로 그 결과에 신뢰도가 비교적 높다고 볼 수 있다. 그러므로 본 연구에서 MMAS 점수를 4점으로 하는 것이 적절하다고 본다.
2가지 형태의 불순응형태가 본 연구의 환자군에서 보여졌다. 의도 적 불순응과 비의도적 불순응이다. 의도적 불순응이 자신의 개인적 경험이나 복약에 대한 믿음에 의해 복약을 빠뜨리거나 바꾸는 적극 적 경우라면 비의도적 불순응은 전혀 다른 형태로 고령이나 임상적 동반질환 같은 문제로 복약에 충실하지 못한 경우이다.23) 비의도적 불순응의 경우는 복약을 충실히 할 수 있도록 하는 보조적 도구가 필요한 경우라면 의도적 불순응의 경우는 환자에게 다른 방식의 접 근이 필요하다고 보여진다. 이런 경우 환자의 약에 대한 믿음을 파악 할 수 있는 것이 BMQ-G 설문지이다.
본 연구에서 MMAS에서 순응도가 높은 경우 BMG-Q 점수 역시 유의하게 낮았다. 본 연구에서 LDLC 목표성취와 BMQ-G 간에 직접 적인 상관관계는 없었다. 그러나 약에 대한 믿음은 순응도를 통하여 간접적으로 나타나는 듯 보인다. 환자에 대한 처방이라던가 환자의 복약에 대한 인식은 비의도적 불순응이나 의도적 불순응의 형태로 나타날 수 있다. 이러한 불순응은 환자 치료결과에 영향을 미친다.
복약에 부정적 사고를 가지거나 약의 부작용에 대한 염려가 많은 경 우 순응도가 떨어질 수 있기 때문이다. 그러므로 순응도 낮은 경우 환자에게 BMQ-G를 실시함으로써 교육으로 교정 가능한 환자 측 요 인을 발견할 수 있다고 보여진다.
본 연구에는 몇 가지 한계점이 있다. 첫째, 연구 종결점인 MMAS 점수가 다른 복약을 확인할 수 있는 약국조제기록이나 병원처방기 록과 비교되지 않아서 순응도의 자가보고와 실제 순응도 사이의 관 계가 정확한지 여부를 확인할 수 없다는 것이다. 둘째, 환자의 기억에 만 의지하므로 고령의 환자들이 많고 경도의 인지기능장애가 있을 것으로 예상되는 본원 환자들 중 많은 수에서 순응도 정도가 정확하 게 보고가 되었는지 의심스러운 점이 있다. 셋째, 비록 의료진 앞에서 작성되지 않았기 때문에 환자가 결과를 과장해서 보고하는 편견이 많은 부분 제거되었을 수 있으나 여전히 환자가 의료진에게 긍정적 인상을 주려고 결과를 과장하였을 가능성이 남아있다고 볼 수 있다.
그래서 응답의 신뢰성을 확보하기 어렵다.
이 연구에 있어서 네 번째 다른 한계점은 다양한 연령과 인구통계 학적 특성을 지닌 집단을 대상으로 하지 않고 공통점이 많은 특정 집단인 표본 수가 적고 여성에 비해 남성의 비율이 높고 연령대의 편
차가 크지 않은 보훈병원 환자군을 대상으로 한 점이다. 그러므로 일 반인구집단을 대표할 수 없어 결과를 일반화하기 어렵다. 이에 이후 인구통계학적 인자가 다양한 다수의 일차 예방군을 대상으로 한 연 구로 MMAS 검사의 유효성을 확인할 필요가 있다고 생각된다.
그럼에도 불구하고 이번 연구결과는 MMAS 결과와 LDLC 성취도 와의 높은 상관성으로 MMAS는 환자의 순응도를 측정하는 데 있어 외래에서 간편하게 시행될 수 있는 검사로 여겨진다. 이에 순응도를 측정하는 도구로써 MMAS를 실용화하는 데 초점을 두고 보완해 나 간다면 이 설문지는 순응도 확인에 유용할 것을 보여진다.
요 약
연구배경:
스타틴은 혈중 저밀도지질단백(low density lipoprotein cholesterol, LDLC)과 심혈관질환의 위험을 감소시키는 강력한 약물 이다. 반면에 스타틴의 효과는 복약 순응도가 떨어짐에 따라 감소한 다. 부적절한 용량, 스타틴에 대한 반응 감소, 생활습관교정 실패, 복 약 순응도 감소 등이 원인이다. 그 중 복약 순응도가 감소한 경우 임 상의는 복약 순응도 문제를 임상적으로 적절하며 간편한 방법으로 확인하여야 한다. 이 연구는 설문조사를 통한 복약 순응도를 신속하 게 확인할 수 있는지의 여부를 고찰하고자 한다.방법:
무작위로 추출된 70명의 환자가 모리스키 복약순응검사 (Morisky Medication Adherence Scale, MMAS) 설문지에 응답하였고, 이 중 2차 예방군인 4명이 배제되고 66명이 추출되어 LDLC 목표 성 취군과 목표 미성취군으로 나눠졌다. 그리고 본 연구에서 MMAS에 서 순응도의 정도와 LDLC 성취 정도를 두 군으로 나눠 연관 지어 분 석하였다.결과:
추출된 환자들의 평균 연령은 64.57세였으며 84.8%는 남자였 다. 조사대상은 설문지에 답변한 환자군 66명이었고, 그 중 40명의 LDLC 목표 성취군이었다. 목표 성취군 유의하게 낮은 LDLC (79.03±17.45 mg/dL vs. 118.81± 25.57 mg/dL, P<0.001), 평균적으로 높은 MMAS 점수(3.43± 0.636점 vs. 2.42± 0.785점, P<0.001)를 보여주었고, 또한 MMAS 점수 4점을 순응도 있는 것으로 보았을 때 미성취군에 비해 좀 더 순응도가 있는 것으로 나왔다(odds ratio, 1.35; 95% confi- dence interval, 107.67-129.95; P= 0.002).
결론:
복약 불순응은 스타틴을 복약하는 환자군에서 LDLC 목표에 도달하지 못하게 하는 요인 중의 하나이다. 이에 본 연구에서는 일상 적인 외래 진료에서 검증된 MMAS는 순응도를 확인할 수 있는 신속 하고 검증된 방법임을 입증하였다.중심단어:
LDL Cholesterol 목표 성취; 복약 순응; 스타틴; 치료 실패김재인 외. 모리스키 복약검사의 유용성 Korean Journal of Family Practice
KJFP
REFERENCES
1. Mann DM, Allegrante JP, Natarajan S, Halm EA, Charlson M. Predictors of adherence to statins for primary prevention. Cardiovasc Drugs Ther 2007;21:311-6.
2. Davidson MH, Maki KC, Pearson TA, Pasternak RC, Deedwania PC, McK- enney JM, et al. Results of the National Cholesterol Education (NCEP) Pro- gram Evaluation ProjecT Utilizing Novel E-Technology (NEPTUNE) II sur- vey and implications for treatment under the recent NCEP Writing Group recommendations. Am J Cardiol 2005;96:556-63.
3. Geller JC, Cassens S, Brosz M, Keil U, Bernarding J, Kropf S, et al. Achieve- ment of guideline-defined treatment goals in primary care: the German Coronary Risk Management (CoRiMa) study. Eur Heart J 2007;28:3051-8.
4. Goldberg KC, Melnyk SD, Simel DL. Overcoming inertia: improvement in achieving target low-density lipoprotein cholesterol. Am J Manag Care 2007;
13:530-4.
5. Kotseva K, Wood D, De Backer G, De Bacquer D, Pyorala K, Keil U, et al.
Cardiovascular prevention guidelines in daily practice: a comparison of EU- ROASPIRE I, II, and III surveys in eight European countries. Lancet 2009;
373:929-40.
6. Afonso NM, Nassif G, Aranha AN, Delor B, Cardozo LJ. Low-density lipo- protein cholesterol goal attainment among high-risk patients: does a com- bined intervention targeting patients and providers work? Am J Manag Care 2006;12:589-94.
7. Parris ES, Lawrence DB, Mohn LA, Long LB. Adherence to statin therapy and LDL cholesterol goal attainment by patients with diabetes and dyslipid- emia. Diabetes Care 2005;28:595-9.
8. Shroufi A, Powles JW. Adherence and chemoprevention in major cardiovas- cular disease: a simulation study of the benefits of additional use of statins. J Epidemiol Community Health 2010;64:109-13.
9. Lee JK, Grace KA, Taylor AJ. Effect of a pharmacy care program on medica- tion adherence and persistence, blood pressure, and low-density lipoprotein cholesterol: a randomized controlled trial. JAMA 2006;296:2563-71.
10. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med 2005;353:
487-97.
11. Morisky DE, Ward HJ, Liu KY. Self-reported medication taking behavior: a valid indicator for assessing compliance (abstract 263520). Proceedings of 129th meeting of the American Public Health Association; 2001 Oct 21-25;
Atlanta, USA. Washington (DC): American Public Health Association;
2001.
12. Benner JS, Glynn RJ, Mogun H, Neumann PJ, Weinstein MC, Avorn J. Long- term persistence in use of statin therapy in elderly patients. JAMA 2002;288:
455-61.
13. Jackevicius CA, Mamdani M, Tu JV. Adherence with statin therapy in elderly patients with and without acute coronary syndromes. JAMA 2002;288:462-7.
14. Perreault S, Blais L, Lamarre D, Dragomir A, Berbiche D, Lalonde L, et al.
Persistence and determinants of statin therapy among middle-aged patients for primary and secondary prevention. Br J Clin Pharmacol 2005;59:564-73.
15. Choo PW, Rand CS, Inui TS, Lee ML, Cain E, Cordeiro-Breault M, et al. Val- idation of patient reports, automated pharmacy records, and pill counts with electronic monitoring of adherence to antihypertensive therapy. Med Care 1999;37:846-57.
16. George CF, Peveler RC, Heiliger S, Thompson C. Compliance with tricyclic antidepressants: the value of four different methods of assessment. Br J Clin Pharmacol 2000;50:166-71.
17. Hawkshead J, Krousel-Wood MA. Techniques for measuring medication adherence in hypertensive patients in outpatient settings. Dis Manag Health Outcomes 2007;15:109-18.
18. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care 1986;24:67-74.
19. Morisky DE, Kominski GF, Afifi AA, Kotlerman JB. The effects of a disease management program on self-reported health behaviors and health out- comes: evidence from the “Florida: a healthy state (FAHS)” Medicaid pro- gram. Health Educ Behav 2009;36:505-17.
20. Shalansky SJ, Levy AR, Ignaszewski AP. Self-reported Morisky score for identifying nonadherence with cardiovascular medications. Ann Pharmaco- ther 2004;38:1363-8.
21. Horne R. Representations of medication and treatment: advances in theory and measurement. In: Petrie KJ, Weinman JA, editors. Perceptions of health and illness: current research and applications. Amsterdam: Harwood Aca- demic; 1997. p. 155-87.
22. Horne R, Weinman J, Hankins M. The beliefs about medicines question- naire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health 1999;14:1-24.
23. Wroe AL. Intentional and unintentional nonadherence: a study of decision making. J Behav Med 2002;25:355-72.
24. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cho- lesterol in Adults. Executive summary of the third report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evalua- tion, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285:2486-97.
25. Krousel-Wood M, Muntner P, Jannu A, Desalvo K, Re RN. Reliability of a medication adherence measure in an outpatient setting. Am J Med Sci 2005;
330:128-33.
26. Bermingham M, Hayden J, Dawkins I, Miwa S, Gibson D, McDonald K, et al. Prospective analysis of LDL-C goal achievement and self-reported medi- cation adherence among statin users in primary care. Clin Ther 2011;33:
1180-9.
27. Cook CL, Wade WE, Martin BC, Perri M 3rd. Concordance among three self-reported measures of medication adherence and pharmacy refill re- cords. J Am Pharm Assoc (2003) 2005;45:151-9.