The Journal of the Korean Society for Surgery of the Hand VOLUME 13, NUMBER 2, June 2008
Dislocation of the Extensor Tendon at the Metacarpophalangeal Joint without Rheumatoid Arthritis
Eun-Sun Moon, Yong-Cheol Park, Myung-Sun Kim, Jong-Seok Kim
1Department of Orthopedic Surgery, Chonnam National University Hospital, Gwang-ju,Korea
Department of Orthopedic Surgery, Sangmoo Hospital, Gwang-ju, Korea1
Purpose: Extensor tendon dislocation at metacar- pophalangeal joint without rheumatoid arthritis is not common condition. We studied the treatment methods for the different causes and the results.
Materials and Methods: We followed 6 cases for 12 months (8-17) in average. The causes are traumatic in 5 cases and congenital in 1 case. The location is 2 cases of third finger, 2 cases of fifth finger, 1 case of both second and third finger and 1 case of ulnar 4 fingers. The direc- tion of dislocations was ulnar side in all except the sec- ond finger which happened in case of both second and third finger. This second extensor tendon was dislocated to the radial side. All cases had pain over two weeks and were operated.
Results: In 4 cases which showed the rupture of sagit- tal band, sagittal band repair was performed. In one case of capsular injury, capsular reefing was performed. In case which showed dislocation of ulnar 4 fingers, sagittal
band repair and looping with extensor hood was per- formed. At last follow-up, recurrent dislocation, pain and limitation of motion was not observed in all cases.
Conclusion: The operative treatment of extensor ten- don dislocation at metacarpophlangeal joint can get a good results. The proper treatment method should be chosen after the exploration about the pathology neces- sarily.
Key Words: Extensor tendon dislocation, Metacar- pophalangeal joint, Operative treatment
서 론
신전건의 중수지 관절부 탈구는 류마티스 관절염 환 자에서는 흔히 발견되지만, 류마티스 관절염 환자가 아닌 경우는 비교적 드문 질환으로 알려져 있다. 원인 은 선천성, 외상성, 자발성(spontaneous) 또는 퇴행 성으로 나눌 수 있다1,2. 1989년 Ishizuki2는 16예를 보고하면서 탈구와 아탈구의 해부학적 차이를 보고하 였고, Inoue와 Tamura1는 27예를 외상성, 자발성, 선천성으로 나누어 보고하기도 하였다. 저자들은 6예 의 중수지관절부 신전건 탈구를 경험하였기에 원인에 따른 치료 방법과 결과를 보고하고자 한다.
연구 대상 및 방법
2007년 1월부터 2007년 10월까지 본원에서 진단받 은 6예에 대해 평균 12개월(8~17개월)간 추시하였다.
평균 연령은 24.1세(17~32)였고, 5예가 남자, 1예가 여자였다. 3예에서 초음파 검사를 시행하여 진단하였 고, 3예는 임상 소견으로 진단하였다. 발생 부위는 제 3수지가 2예, 제 5수지가 2예, 2번 및 3번 수지 동시 발생이 1예, 2번부터 5번 수지까지 이환된 경우가 1예 였다. 탈구 방향은 모두 척측 탈구였으나 2번 및 3번
류
류마 마티 티스 스 병 병력 력이 이 없 없는 는 환 환자 자에 에서 서 중 중수 수지 지 관 관절 절부 부 신 신전 전건 건 탈 탈구 구
전남대학교 의과대학 정형외과학 교실, 광주 상무병원 정형외과1 문은선∙박용철∙김명선∙김종석1
통신저자: 박박 용용 철철
광주광역시 동구 학동 8 전남대학교병원 정형외과
TEL: 062-220-6336, FAX: 062-225-7794 E-mail: [email protected]
* 본 논문의 요지는 2007년도 대한수부외과학회 추계학술대회 에서 발표되었음.
수지에서 동시 발생한 예에서 제 2수지는 요측 탈구를 보였다. 2번부터 5번 수지까지 발생했던 예는 반대측 손에서도 제 2수지와 제 3수지 신전건의 척측 탈구를 보였다. 원인은 5예가 외상에 의한 발생이었고, 1예는 선천적 발병이었다. 증상 발현 기간은 평균 23주 (2~52)였으며, 모든 예에서 동통 등의 증상을 동반하
여 수술적 치료를 시행하였다. 결과는 임상적으로 재발 여부와 통증의 유무, 관절 운동 범위를 평가하였다.
결 과
수술 소견상 4예는 시상대 파열 소견을 보여 시상대 Table 1. Summary of cases.
Case Sx duration Trauma Hx Site Sx Direction Operation
25/M 6 mos (-) 2,3,4,5th Pain c snapping Ulnar Only 2nd finger
Looping &Reefing
17/M 5 wks (+) 5th Pain Ulnar SB* repair
31/M 1 yr (+) 3rd Pain Ulnar SB repair
32/M 2 wks (+) 3rd Pain Ulnar SB repair
21/F 11 mos (+) 5th Pain c catching Ulnar Capsular repair &
reefing
19/M 3 mos (+) 2,3rd Pain 2nd-Radial 2,3rd finger
3rd-Ulnar SB repair
*SB: Sagittal band
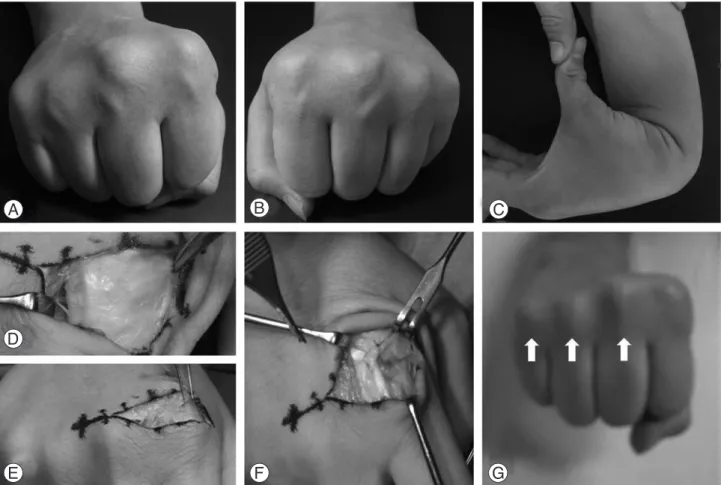
Fig. 1. Twenty five year-old man. (A, B) He showed bilateral multiple extensor tendon dislocations. (C) He had the mild tendency of joint laxity. (D) The operative finding showed not the deficiency but the attenuation of sagittal band. (E) After reduction of the second extensor, the other three ulnar extensors were relocated spontaneously. (F) The sagittal band repair and looping with extensor hood was performed. (G) This follow-up photograph showed that the third, fourth, fifth extensor tendons were in right place (arrows).
봉합술을 시행하였고, 1예에서는 관절낭 손상으로 인 한 이완 소견보여 관절낭 봉합 및 보강술을 시행하였 다. 양측 손에서 발병하고 과다 관절 운동 소견보여 선 천적 발병으로 생각된 1예에서는 제 2수지 시상대가 얇아진 소견보여 시상대 봉합술 및 신전건두포(exten- sor hood)를 이용한 고리 보강술을 시행하였으며, 제 2수지 신전건의 정복만으로 제 3,4,5수지 신전건의 정 복이 이루어져 이들 수지에 대해서는 좌측 제 2,3수지 와 함께 수술적 치료를 시행하지 않았다. 추시상 모든 예에서 탈구의 재발이나 통증은 없었고 관절 운동범위 정상이었다.
증례 보고
증례 1.
25세 남자 환자로 3년 전부터 시작된 우측 제 2 중 수지 관절 배부의 통증을 주소로 내원하였다. 외상력 은 없었으며, 진찰 소견상 우측 2, 3, 4, 5수지와 좌 측 2,3수지 중수지 관절부에서 탄발음을 동반한 신전
건 탈구 소견이 관찰되었다(Fig. 1A, B). 관절 운동 범위는 정상이었으며, 관절의 과다 유연성 소견 보이 고 있었다(Fig. 1C). 수술 소견상 제 2 수지 요측 시 상대가 얇아진 소견보였으며(Fig. 1D), 제 2수지 신 전건의 정복만으로 제 3,4,5 수지 신전건의 정복을 얻 을 수 있었다(Fig. 1E). 제 2수지에 대해서만 시상대 봉합술 및 신전건두포를 이용한 고리 보강술 시행하였 다(Fig. 1F). 17개월 추시상 통증이나 재발 소견은 보이지 않았으며 관절 운동 범위는 정상이었다.
증례 2.
19세 남자 환자로 3개월 전 발생한 제 2, 3중수지 관절 배부 통증을 주소로 내원하였다. 3개월 전에 주 먹 가격한 외상력이 있었으며, 무거운 물건을 들 때 신전건이 빠지는 것 같은 느낌을 호소하였다. 진찰 소 견상 종창은 없었으며, 제 3수지 신전건의 척측 탈구 소견이 보였으나, 제 2수지 신전건은 특이 소견 관찰 할 수 없었다(Fig. 2A). 확진을 위해 시행한 초음파 소견상, 종주사 소견상 특이 소견없었으며, 횡주사 소 Fig. 2. Nineteen year-old man. (A) A gross finding documented the ulnar dislocation of the third extensor and the radial dislocation of the second finger. (B) US can confirmed the divergent dislocation of the second (upper) and the third (lower) extensor ten- don (arrow). (C) When clenched the fist, the second extensor tendon was dislocated to ulnar side. (D) This postoperative 2 months’ follow-up photograph did not show the re-dislocation of extensor.
견상 주먹을 쥘 때 제 2신전건의 요측 탈구와 제 3신 전건의 척측 탈구를 확인할 수 있었다(Fig. 2B). 수 술 소견상 제 2신전건의 척측 시상대와 제 3 신전건의 요측 시상대 파열 소견보여(Fig. 2C), 각각 시상대 봉합술 시행하였다. 8개월째 전화를 통한 추시상 통증 이나 재발은 없었으며 관절 운동범위는 정상이었다.
고 찰
중수지 관절에서 신전건의 탈구는 중수지관절 배부 에 위치하는 신전건두포의 이상에 의해 발생한다3. 시 상대는 신전건에서 시작되어 중수골 두부의 요측 및 척측으로 지나 수장판(palmar plate)에 붙게 되며, 중수지 관절의 운동이 시작될 때 근위부 및 원위부로 약간의 운동을 허용하면서 이 섬유들에 의해 신전건을 중앙부에 위치하도록 도와준다. 중수지 관절에서 신전 건은 능동적으로는 신전건두포와, 수동적으로는 보조 건과 시상대에 의해 안정성이 유지되며, 외상이나 관 절염 등의 원인에 의해 이 구조물들이 손상을 받게되 면 신전건의 탈구를 유발하게 된다. 신전건두포의 아 래에는 관절막이 존재한다. 시상대는 신전건의 배부를 덮는 천층과 신전건의 양 옆에서 기시하여 인대를 제 자리에 유지시키는 심층으로 이루어져 있다. 또한 보 조건(juncturae tendinum)은 각각의 신전건을 사상 으로 연결하는 근막으로 이루어진 해부학적 변이가 많 은 연결 구조이다. 이 구조는 중수지 관절에서 신전건 을 안정시키는 역할을 한다.
Inoue와 Tamura1는 27예의 신전건 탈구를 보고하 면서 16에의 외상성, 7예의 자발성, 4예의 선천성 탈 구를 보고하였다. 그들은 외상성 탈구는 외상력이 있 는 경우 진단하였고 손상된 시상대의 봉합을 통해 치 료하였다. 자발성 탈구는 외상력이 없이 일상 생활간 에 탈구가 발생한 경우라고 하였다. 선천성 탈구의 경 우는 양측에서 발생하였고 다른 관절의 과다 유연성이 보였다고 하였으며, 수술 소견은 2예에서는 시상대가 없었고 2예는 느슨하거나 얇았다고 보고하였다. 한편, Posner와 McMahon4은 시상대가 약화(attenua- tion)되어 있다고 하였다. 저자들의 예에서도 전신 관 절의 과다 유연성 소견이 보였고, 양측에서 탈구가 발 생하여 선천성 탈구로 판단하였으며, 수술 소견상 시 상대가 약화된 소견을 관찰할 수 있었다.
Rayan 등5은 치료의 목적이 불안정성의 회복보다는 통증의 호전이라고 하였으며, 부목 고정과 수술적 치 료를 시행할 수 있다. 보존적 치료는 중수관절 신전 상태에서 약 2주간 부목 고정으로 실시하며, 그 시기 에 대해서는 증상 발현 이후 10일 이내6, 2주 이내1 또 는 3주 이내5로 그 보고가 다양하다. 저자들은 모든 예
에서 2주 이상 지연된 통증을 보여 수술적 치료를 시 행하였으며, 선천성 탈구 환자에서 제 2번, 3번 수지 신전건의 탈구를 보였던 좌수에 대해서는 증상이 없어 치료를 시행하지 않았다.
Rayan 등5은 시상대 손상 형태에 따라 치료방법을 달리해야 한다고 하였다. 대부분 척측 시상대 유리술과 요측 시상대 봉합술을 시행하였으며, 결손(defect), 큰 파열(large tear), 얇아진 시상대가 있는 경우에 봉합술만으로 정복이 불가능하다면 주변 조직을 이용 하여 안정화시켜야 한다고 하였다. 주변 조직을 활용하 는 방법으로는 Wheeldon7, McCoy와 Winsky8, Carrol 등9이 제안한 방법이 흔히 사용되고 있다. 한 편, 측부 인대 손상이나 관절막 손상에 의한 신전건 불 안정성의 유무를 감별 진단하여 원인에 맞는 치료가 필 요하다고 하였다5. 저자들의 경우 선천적으로 발병한 1 예에서 제 2수지 요측 시상대가 얇아진 소견을 보였으 며, 제2수지 신전건 정복시 손상되지 않은 보조건에 의해 3, 4, 5수지 신전건이 정복되는 소견였다. 제 3, 4, 5수지 신전건 정복에 필요한 제 2수지 보조건을 유 지하기위해 요측 시상대를 이용하여 고리 보강술을 시 행하였다. 제 5수지에서 발생한 1예에서는 관절낭 손 상에 의한 이완 소견 보여 관절낭 봉합술 및 보강술 시 행하였다.
결 론
중수관절부 신전건 탈구의 치료에 있어서 탈구의 원 인을 밝히는 것이 치료 계획을 세우는데 중요하며, 수 술 소견에 따라 수술 방법을 달리해야한다. 적절한 수 술 적응증을 가지고 원인에 따른 치료를 한다면 환자 의 만족도가 높고 좋은 결과를 얻을 수 있을 것으로 사료된다.
참고문헌
01) Inoue G, Tamura. Dislocation of the extensor tendons over the metacarpophalangeal joint s. J Hand Surg Am. 1996;
21: 464-9.
02) Ishizuki M. Traumatic and spontaneous dislocation of extensor tendon of the long finger. J Hand Surg Am. 1990;
15:967-72.
03) Green DP, Hotchkiss RN, Pederson WC, Wolfe SW.
Green's operative hand surgery. 5th ed. Philadelphia:
Churchill Livingstone; 2005. p209-12.
04) Posner MA, McMahon MS. Congenital radial subluxation of the extensor tendons over the metacarpophalangeal joints: a case report. J Hand Surg Am. 1994; 19: 659-62.
05) Rayan GM, Murray D, Falls T. Classification and treat- ment of closed sagittal band injuries. J Hand Surg Am.
1994;19:590-4.
06) Araki S, Ohtani T, Tanaka T. Acute dislocation of the extensor digitorum communis ten don at the metacar- pophalangeal joint. J Bone Joint Surg Am. 1987;69:616-9.
07) Wheeldon FT. Recurrent dislocation of extensor tendons
in the hand. J Bone Joint Surg Br. 1954;36:612-7.
08) McCoy FJ, Winsky AJ. Lumbrical loop operation for luxa- tion of the extensor tendons of the hand. Plast Reconstr Surg. 1969;44:142-6.
09) Carroll C, Moore JR, Weiland AJ. Posttraumatic ulnar subluxation of the extensor tendo ns: A reconstructive technique. J Hand Surg Am. 1987;12:227-31.