Korean Journal of Neuromuscular Disorders 2018 13 Joong-Yang Cho | Neurolymphomatosis
Received: November 27, 2018 / Revised: December 14, 2018 / Accepted: December 14, 2018 Address for correspondence: Joong-Yang Cho, MD, PhD
Department of Neurology, Ilsan Paik Hospital, Inje University College of Medicine, 170 Juhwa-ro, Ilsanseo-gu, Goyang 10380, Korea Tel: +82-31-910-7929, Fax: +82-31-910-7368, E-mail: [email protected]
ISSN 2093-3312
Korean Journal of Neuromuscular Disorders Vol. 10 No. 2, December 2018
Review
말초신경계의 신경림프종증
인제대학교 의과대학 일산백병원 신경과
조 중 양
Neurolymphomatosis of Peripheral Nervous System
Joong-Yang Cho, MD, PhD
Department of Neurology, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea
KEYWORDS Neurolymphomatosis, Cranial nerves, Peripheral nervous system
Neurolymphomatosis (NL) is a rare disease characterized by the infiltration of the cranial nerves or peripheral nervous system by lymphoma cells. High suspicion with regard to the identification of the disease is important because the various presenting symptoms require a consideration of many differential diagnoses. In recent years, there has been increasing prevalence of the condition which is associated with the increasing use of fluorodeoxyglucose positron emission tomography (FDG-PET) and magnetic resonance imaging (MRI) in evaluating peripheral nervous system disorders. This paper presents a review of the literature about neurolymphomatosis.
서 론
암과 관련된 신경학적 합병증 중에 말초신경병증은 드물 지 않다. 암 환자에서 나타날 수 있는 말초신경병증의 원인 으로는 암에 의한 직접적인 신경 압박 또는 암의 침윤, 치 료와 관련된 신경 독성, 영양 결핍, 대사 불균형 그리고 신 생물딸림질환 등이 있다.1
여러 원인(감염, 항암제의 부작용, 면역기전, 신경조직에 대한 암세포 침윤 등)에 의하여 림프종에서 말초신경병증 이 발생하고(약 5%),2 그중에서 신경조직에 대한 직접적인 암세포 침윤을 신경림프종증(neurolymphomatosis, NL)이라 고 하며, 비호지킨 림프종(non-Hodgkin lymphoma, NHL)의 약 0.2%에서 발생한다고 추정된다.3 신경림프종증은 뇌신 경(cranial nerves) 및 말초신경계(peripheral nervous system [PNS], nerves, roots, plexus)를 침범하는 임상적으로 매우
드문 질환으로,4 대부분 말기 림프종 환자에서 감각운동성 다발신경병증으로 발현되지만 림프종 진단 시나 치료 도중 에 발현되는 경우도 있다.4
신경림프종증은 림프종에서 동반되는 말초신경질환 (paraneoplastic PNS involvement and radiation-and chemo- therapy-induced damage to the PNS)과 감별이 중요하다.5 두 드러진 비대칭성과 통증 및 신경영상에서 결정성의 침범 (nodular involvement)은 신생물딸림 면역탈수초신경병증 과의 감별점이기도 하다.6 최근 조영증강 자기공명영상 (magnetic resonance imaging, MRI) 및 양전자방출전산화단 층촬영(positron emission tomography-computed tomography, PET-CT) 등의 영상학적인 방법을 이용하여, 의심되는 신경 의 영상 변화를 포착하여 진단율이 높아지고는 있으나 임 상적으로 신경림프종증 자체를 추정하지 못하여 진단 및 치료가 늦어지는 경우가 많다.7 따라서 임상적으로 조기에
대 한 신 경 근 육 질 환 학 회 지 2 0 18 14
Korean Journal of Neuromuscular Disorders Vol. 10 No. 2, 2018
감별진단에 고려하는 것이 중요하다.
본 론
신경림프종증은 원인으로 B세포림프종이 가장 흔하고 T 세포림프종이 드물게 보고된다.8 또한 신경림프종은 NHL, 특히 광범위 큰B세포림프종(diffuse large B cell lymphoma, DLBCL) 및 급성 백혈병과 관련이 있다.9 말초성 T세포림 프종(peripheral T-cell lymphomas, PTCLs)은 성인 NHL에서 약 10-15% 정도 차지하는 것으로 알려져 있다.10
신경림프종증은 일차성과 이차성으로 나누어지는데, 일 차성 신경림프종증(primary NL)은 혈액암(hetamtologic ma- lignancy)의 첫 증상이 신경림프종증인 것이고, 림프종 또는 백혈병의 재발이나 진행에 의한 신경림프종증이라면 이차 성 신경림프종증(secondary NL)으로 분류된다.11 이차성 신 경림프종증에 비하여 일차성 신경림프종증은 진단 자체가 어렵고, 일차성 신경림프종증으로 침범된 뇌신경 병변과 일 차성 중추신경계 림프종(primary central nervous system lymphoma, PCNSL)의 감별이 잘 정립되어 있지 않아 진단 및 감별이 어려울 때가 많다.12 PCNSL은 림프절외(extranodal) 고등급(high grade) 비호지킨 B세포 종양으로, 대개 큰세포 또는 면역모세포 타입으로 알려져 있다. 뇌, 연질뇌척수막, 척수 또는 눈에서 기원하며 전형적으로 중추신경계에 국한 되고, 드물게 중추신경계 외로 퍼지기도 한다.
Currie와 Henson13은 NHL 환자 228명 중 오직 1예에서 말초신경계를, 다른 1예에서 뇌신경을 침범하였다고 하였 다. Richmond 등14은 1%에서만 말초신경계를 침범하였다고 보고하였다. 그러나 Baehring 등15은 NHL로 사망한 145명 의 환자에 대한 부검 결과 40%에서 림프종세포가 말초신경 을 침범한 증거가 있었다고 보고하였다. 이처럼 신경림프종 증은 부검에서는 침범되어 있으나, 임상적으로 진단된 경우 가 매우 드물며, 특히 증상이 아급성으로 수개월에 걸쳐 서 서히 나타나는 경우는 더욱 진단이 어렵다.
신경림프종증의 임상양상은 다양하며 말초신경(60%), 척 수신경근(48%), 뇌신경(46%), 신경총(40%) 및 여러 곳을 동시 다발적으로 침범(58%)할 수 있다.11 또한 통증 동반 여 부와 침범 부위에 따라 4개의 임상양상으로 분류하기도 한 다; 1) 통증성 또는 비통증성 단일신경병증 또는 다발성단 일신경염(painful or painless peripheral mononeuropathy or mononeuritis multiplex), 2) 통증성 다발신경병증 또 는 다발신경근병증(painful peripheral polyneuropathy or polyradiculopathy), 3) 비통증성 다발신경병증(painless poly-
neuropathy), 4) 통증성 또는 비통증성 뇌신경병증(painful or painless cranial neuropathy).16,17 Chamberlain과 Fink4는 림프 종이 진단되기 전에 신경림프종증 임상 증상이 발현되는 경우(10%)와 림프종 진단과 동시에 발견되거나(25%), 림프 종의 재발로서 나타나는 경우로 나누었다(40%). 그러나 신 경림프종증은 전신질환보다 앞서 나타난다고 하더라도 결 국 전신 림프종으로 발현하는 경우가 많다(약 73%).18
최근에 Avila와 Vivar3는 2013년도부터 2015년도까지 발 표된 82개의 증례를 분석하여 보고하였다. 남녀비는 57:43 으로 남자가 조금 더 많았으며, 평균 연령은 60세(27-85), 일차성 신경림프종증이 37%, 이차성 신경림프종증이 63%
였으며, 신경림프종증과 관련된 혈액암 중에 가장 흔한 것은 DLBCL이었다(76%).3 임상양상은 통증성 신경(근)병증 (38%), 단일신경병증(24%), 뇌신경병증(23%), 다발성 단일 신경병증(10%), 비통증성 신경병증(5%) 순이었다. 뇌척수 액검사에서 악성 세포가 검출된 경우는 40%, 조영증강 MRI에서 양성인 경우는 83%였으며, fluorodeoxyglucose PET (FDG- PET)에서는 91%, 신경조직검사에서 91%에서 이상 소견을 보였다.3 Martinez-Thompson 등19도 1992년부 터 2016년까지 단일센터(Mayo Clinic in Rochester)에서 조 직검사로 확진된 49명의 환자들의 특성을 분석하였다. 일 차성 신경림프종증이 59%, 이차성 림프종증이 41%였다.
가장 흔한 임상양상은 비대칭성 통증성 신경근신경총 신경 병증(37.5%), 다발신경근병증(23%), 다발성/단일신경병증 (multiple/single mononeuropathies, 18%) 순이었다.19 MRI가 림프종을 진단하는 데는 컴퓨터단층촬영(CT) 또는 PET보 다는 우월하였다(MRI vs. CT vs. PET, 84% vs. 46% vs.
58%). 일차성 신경림프종증과 이차성 신경림프종증 모두에 서 DLBCL 비율이 가장 높았다(96%). 원위부 피부 또는 근 위부 신경다발(nerve fascicle) 조직검사에서 탈수초성 병변 과 빈신경띠(empty nerve strands)가 보였으며, 축삭변성은 일차성 신경림프종증보다 이차성 신경림프종증에서 뚜렷하 고(31% vs. 7%; p=0.005), 이차성 신경림프종증이 일차성 림프종증에 비하여 치료에 대한 반응이 좋지 않았으며(33%
vs. 62%, p=0.02), 사망률은 이차성 림프종증이 더 높았다 (60% vs. 24%, p=0.015).19
신경림프종증은 다양한 형태로 나타날 수 있기 때문에 진단이 쉽지 않으며, 확진을 위해서는 신경조직검사가 필요 하다. 그러나 신경조직검사 자체가 침습적이며, 병변의 위 치 특성상 검사 자체가 어려운 경우가 많고 조직검체가 충 분하지 않을 경우, 검사 결과가 음성으로 나올 확률도 높다.
따라서 최근에 영상기술을 포함한 여러 진단기술의 발전에 따라 점차 조직검사가 생략되는 경우가 많고, 임상증상, 전
Korean Journal of Neuromuscular Disorders 2018 15 Joong-Yang Cho | Neurolymphomatosis
A B C
D E
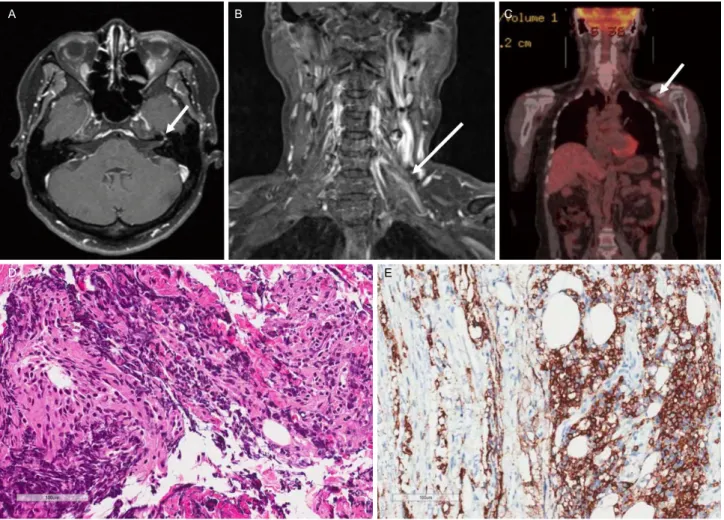
Figure 1. A 59-year-old female diagnosed with diffuse large-B-cell lymphoma which presented itself sequentially as diplopia, facial palsy, and brachial. Analysis of brain and spinal MRI showed thickened and enhancing left facial (A, arrow), thickened and heterogeneous enhancement of left brachial plexus (B, arrow). PET-CT showed mild linear FDG uptake along the left brachial plexus (C, arrow). Biopsy of the C7 root showed infiltration comprising predominantly of small lymphocytes (D; haematoxylin and eosin, ×200) and diffuse CD20-positive cells (E; immunochemical stain,
×200). Revised from reference 21. MRI, magnetic resonance imaging; PET-CT, positron emission tomography-computed tomography; FDG, fluorodeoxyglucose.
기생리학적 검사, MRI 및 PET 등의 영상검사만으로도 조 직검사 없이 신경림프종증을 진단하기도 한다.20 검사들의 민감도는 연구마다 차이가 나는데, PET-CT의 민감도는 87.5-100%, MRI의 민감도는 40%, 뇌척수액 검사의 민감도 는 21%로 보고된 연구도 있어,9,21 다른 연구들과 민감도에 서 차이가 나지만,3,19 PET와 MRI 검사를 모두 이용한다면 진단율을 높일 수 있으며, 뇌척수액검사는 민감도가 높지 않기 때문에 해석에 주의를 요하며 신경림프종증이 강력히 의심된다면 반복적 검사가 필요할 수 있다.
스테로이드는 단기간 증상 완화에 도움이 되며, 정주 면 역글로블린은 이차성 신경림프종증에 초기 반응이 있다고 알려져 있다.22 표준화된 치료 방법은 아직 확립되지 않았으 며, 대개 악성 중추신경계 림프종에 준해서 치료하게 된다.
신경림프종증은 드문 질환이며 림프종세포가 신경을 침 범하여, 원위부에서 탈수초를 유발하고 축삭변성을 일으킨 다. 또한 초기 발현양상이 다양하고 염증성 신경근/신경총/
말초신경병증 및 다른 형태의 국소성 말초신경병증과의 감 별은 쉽지 않으며, 여러 감별진단(바이러스, 염증성 또는 신 생물딸림 신경병증, 다발성 뇌신경염, 연수막림프종증, 신 경근 압박)이 필요하여, 진단이 어렵고 늦어지는 경우가 많 다.23 이렇듯 조기진단과 감별진단이 어렵기 때문에 아급성, 통증성 말초신경병증으로 적절한 면역 치료를 하였는데도 불구하고 심한 통증과 진행양상을 보인다면 신경림프종을 의심해 보는 것이 좋다.24
대 한 신 경 근 육 질 환 학 회 지 2 0 18 16
Korean Journal of Neuromuscular Disorders Vol. 10 No. 2, 2018
결 론
신경림프종증은 아급성, 통증성 말초신경증후군(subacute, painful peripheral nerve syndrome)으로 이해하는 것이 필요 하다.19 신경림프종증이 림프종의 첫 임상증상이거나 재발 이나 종양의 진행의 양상으로 나타날 수 있기 때문에 앞서 언급한 증상들이 나타나면 신경림프종증의 가능성을 고려 하고 것이 좋으며, MRI와 FDG-PET 등을 이용하고, 필요시 조직검사를 시행한다면 진단율을 높일 수 있다(Fig. 1).
REFERENCES
1. Kim SY. Cancer-related Neuropathies. Korean J Neuromuscul Disord 2015;7:56-63.
2. Hughes RA, Britton T, Richards M. Effects of lymphoma on the peripheral nervous system. J R Soc Med 1994;87:526-530.
3. Avila JD, Vivar C. Neurolymphomatosis: a review of 82 cases.
Neurology 2017;88(16 Supplement):P5.141.
4. Chamberlain MC, Fink J. Neurolymphomatosis: a rare metastatic complication of diffuse large B-Cell lymphoma. J Neurooncol 2009;95:285-288.
5. Peterson J, Caliskan B, Bonyadlou S. Positron emission tomography/computerized tomography imaging of multiple focus of neurolymphomatosis. Indian J Nucl Med 2014;29:252-253.
6. Bourque PR, Warman Chardon J, Bryanton M, Toupin M, Burns BF, Torres C. Neurolymphomatosis of the brachial plexus and its branches: case series and literature review. Can J Neurol Sci 2018;45:137-143.
7. Kuntz C 4th, Blake L, Britz G, Filler A, Hayes CE, Goodkin R, et al. Magnetic resonance neurography of peripheral nerve lesions in the lower extremity. Neurosurgery 1996;39:750-756; discussion 756-757.
8. Kelly JJ, Karcher DS. Lymphoma and peripheral neuropathy: a clinical review. Muscle Nerve 2005;31:301-313.
9. Choi YJ, Shin JA, Kim YH, Cha SJ, Cho JY, Kang SH, et al.
Neurolymphomatosis of brachial plexus in patients with non-Hodgkin's lymphoma. Case Rep Oncol Med 2013;2013:492329.
10. Vose J, Armitage J, Weisenburger D; International T-Cell Lymphoma Project. International peripheral T-cell and natural killer/T-cell lymphoma study: pathology findings and clinical
outcomes. J Clin Oncol 2008;26:4124-4130.
11. Grisariu S, Avni B, Batchelor TT, van den Bent MJ, Bokstein F, Schiff D, et al. Neurolymphomatosis: an International Primary CNS Lymphoma Collaborative Group report. Blood 2010;115:
5005-5011.
12. Sakai N, Ito-Yamashita T, Takahashi G, Baba S, Koizumi S, Yamasaki T, et al. Primary neurolymphomatosis of the lower cranial nerves presenting as Dysphagia and hoarseness: a case report. J Neurol Surg Rep 2014;75:e62-e66.
13. Currie S, Henson RA. Neurological syndromes in the reticuloses.
Brain 1971;94:307-320.
14. Richmond J, Sherman RS, Diamond HD, Craver LF. Renal lesions associated with malignant lymphomas. Am J Med 1962;
32:184-207.
15. Baehring JM, Damek D, Martin EC, Betensky RA, Hochberg FH.
Neurolymphomatosis. Neuro Oncol 2003;5:104-115.
16. Diaz-Arrastia R, Younger DS, Hair L, Inghirami G, Hays AP, Knowles DM, et al. Neurolymphomatosis: a clinicopathologic syndrome re-emerges. Neurology 1992;42:1136-1141.
17. Gordon PH, Younger DS. Neurolymphomatosis. Neurology 1996;46:1191-1192.
18. Shree R, Goyal MK, Modi M, Gaspar BL, Radotra BD, Ahuja CK, et al. The diagnostic dilemma of neurolymphomatosis. J Clin Neurol 2016;12:274-281.
19. Martinez-Thompson J, Suanprasert N, King R, Macon W, Mauermann M, Amrami K, et al. Neurolymphomatosis: clinical, radiographic, and pathologic characteristics. Neurology 2017;88 (16 Supplement):S45.005.
20. Lin M, Kilanowska J, Taper J, Chu J. Neurolymphomatosis- -diagnosis and assessment of treatment response by FDG PET- CT. Hematol Oncol 2008;26:43-45.
21. Lee HJ, Kim GS, Song P, Lee JJ, Sung JJ, Choi KM, et al.
Neurolymphomatosis presenting as brachial plexopathy with involvement of cranial nerves. Ann Clin Neurophysiol 2018;20:
44-48.
22. Sideras PA, Matthews J, Sakib SM, Ofikwu F, Spektor V.
Neurolymphomatosis of the peripheral nervous system: a case report and review of the literature. Clin Imaging 2016;40:1253-1256.
23. Gan HK, Azad A, Cher L, Mitchell PL. Neurolymphomatosis:
diagnosis, management, and outcomes in patients treated with rituximab. Neuro Oncol 2010;12:212-215.
24. Sabatelli M, Laurenti L, Luigetti M. Peripheral nervous system involvement in lymphoproliferative disorders. Mediterr J Hematol Infect Dis 2018;10:e2018057.