Copyright © 2015 The Korean Association for Health Technology Assessment
Introduction
Heart failure (HF) is currently known as a common cause of death arising from cardiovascular diseases. It is a very impor- tant disorder not only from medical perspective but also from socioeconomic perspective due to the trend of increasing prevalence rate as the result of the increase in the chronic car- diac disorder patients and elderly population.1) Although there has been substantial advancement in the diagnosis and treat- ment of HF in the recent years, the prognosis of HF still re- mains poor. On the basis of data from National Health and Nutrition Examination Survey 2009 to 2012, an estimated 5.7 million Americans adults have HF and one in 9 deaths include HF. Also about half of people who develop HF die within 5 years of diagnosis.2,3) Therefore, biochemical markers that can predict the prognosis of HF are not only very important but also establishing themselves as an indispensable test.
Suppression of tumorigenicity 2 (ST2) is a cardiac biomark-
er that has been recently disclosed as a substance secreted into the blood in the event of cardiac disorder or damages. ST2 is a type of interleukin-1 receptor and can be categorized into 2 types, namely, soluble ST2 and isoform format of ST2 receptor (transmembrane ST2 isoform).4) It is a biomarker for determi- nation of prognosis of cardiac disorders along with B-type na- triuretic peptide (BNP) and N-terminal pro-BNP (NT pro- BNP).5) The ligand of ST2 is IL-33, which is the substance in- volved in the fibrosis or hypertrophy of mechanically strained tissues.6) When the concentration of ST2 increases, it combines with IL-33 to inhibit the proper operation of the cardio-pro- tective signaling system and may induce cardiac cell death, tis- sue fibrosis and degradation of cardiac functions.7,8)
According to the guidelines by the American College of Cardiology Foundation and the American Heart Association in 2013, ST2, which is a biomarker of myocardial fibrosis, was reported to be capable of not only predicting the death and hospitalization of HF patients but also adds prognosis assess-
Effectiveness of the Suppression of Tumorigenicity 2 for Prognosis in Heart Failure: Systematic Reviews
So Young Kim and Hee Young Bang
Division for New Health Technology Assessment, National Evidence-Based Healthcare Collaborating Agency, Seoul, Korea
Received November 2, 2015 Revised November 10, 2015 Accepted November 24, 2015 Address for Correspondence:
So Young Kim
Division for New Health Technology Assessment, National Evidence-Based Healthcare Collaborating Agency, 173 Toegye-ro, Jung-gu, Seoul 04554, Korea Tel: +82-2-2174-2855 Fax: +82-2-741-7060 E-mail: [email protected]
Objectives: Suppression of tumorigenicity 2 (ST2) reflects activity of the cardioprotective signal and it is a prognostic marker in heart failure. The purpose of this study is to assess the effectiveness of the ST2 for determination of the prognosis of patient with heart failure. Methods: We searched the eight Korean databases and Ovid-MEDLINE, Ovid-EMBASE, Cochrane Library. Total 365 stud- ies were searched and 19 studies were included in the final assessment. Each of the stages from litera- ture search and extraction of data were carried out independently by 2 researchers. We used tools of Scottish Intercollegiate Guidelines Networks for assessment of the quality of studies. Results: The effectiveness of the ST2 was assessed by means of association with prognosis [risk ratio (RR) or odds ratio (OR), accuracy of forecasting of the prognosis, stratification of risk], correlation with the comparators and relevance with clinical symptoms. The RR or OR of the death arising from ST2 was 1.01−4.56, the RR of hospitalization was 1.054−2.4. On the other hand, RR of hospitalization of B-type natriuretic peptide (BNP) was 1.15−2.0, the RR or OR of death arising from N-terminal pro- BNP (NT pro-BNP) was 0.19−1.241. The sensitivity/specificity of the ST2 was 64−87%/51−82% and area under the ROC curve values were 0.689−0.84. The stratification of risk (net reclassification im- provement) on the death rate were reported to be significant at 9.4 and 9.9 in the 2 studies, but 1 study reported that stratification of risk of the death rate was 0.049 and stratification of risk of hos- pitalization rate was 0.0638. The correlation coefficients with BNP was 0.16−0.409 and with NT pro-BNP was 0.28−0.523. Conclusion: The ST2 is effective in determining the prognosis of pa- tients with heart failure.
Key Words Heart failure · Prognosis · ST2 · Systematic review.
Original Article
JoHTA
ment value to the natriuretic peptide level. Moreover, it was re- ported that application of various biomarkers simultaneously is useful in treatment of HF.9)
The purpose of this study was to evaluate whether ST2 is ef- fective in predicting the prognosis of the HF.
Methods
Search strategy
To identify and retrieve all relevant literature describing the effectiveness of ST2 for prognosis in HF patients, we searched databases including Ovid-MEDLINE (1948 to 8 August 2014), Ovid-EMBASE (1980 to 8 August 2014), Cochrane Central Register of Controlled Trials on The Cochrane Library and eight Korean databases. Language restrictions did not apply to any of the searches. Search terms included both keywords and corresponding Medical Subject Headings; thus “heart failure”
AND “ST2” (Table 1).
Study selection
Two researchers independently assessed publications con-
sidered to be eligible for inclusion at the title and/or abstract level. Full test reviews were conducted if it was difficult to as- certain from the abstract whether the article met our inclu- sion/exclusion criteria. Studies were included: 1) if patients with HF were performed; 2) if ST2 test performed to evaluate prognosis of HF; 3) if appropriate outcomes were reported. We excluded: 1) non-human, pre-clinical studies; 2) studies that
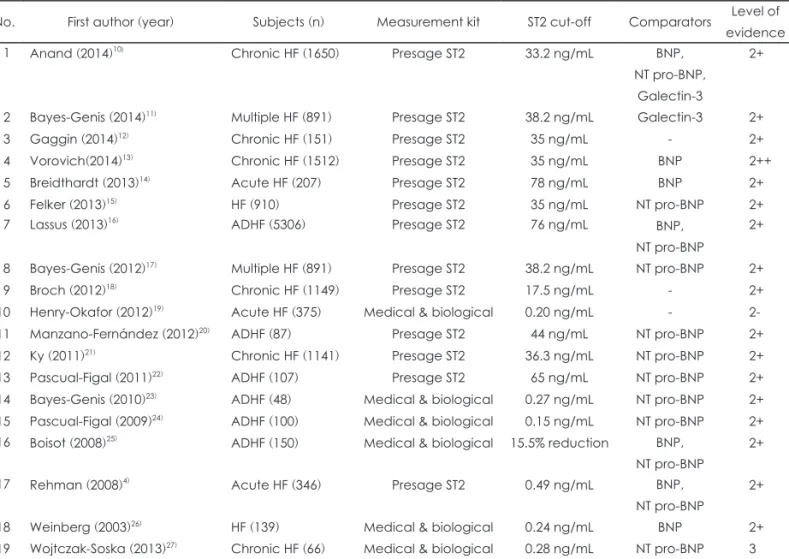
Table 2. Study selected for evaluation of ST2
No. First author (year) Subjects (n) Measurement kit ST2 cut-off Comparators Level of evidence
1 Anand (2014)10) Chronic HF (1650) Presage ST2 33.2 ng/mL BNP,
NT pro-BNP, Galectin-3
2+
2 Bayes-Genis (2014)11) Multiple HF (891) Presage ST2 38.2 ng/mL Galectin-3 2+
3 Gaggin (2014)12) Chronic HF (151) Presage ST2 35 ng/mL - 2+
4 Vorovich(2014)13) Chronic HF (1512) Presage ST2 35 ng/mL BNP 2++
5 Breidthardt (2013)14) Acute HF (207) Presage ST2 78 ng/mL BNP 2+
6 Felker (2013)15) HF (910) Presage ST2 35 ng/mL NT pro-BNP 2+
7 Lassus (2013)16) ADHF (5306) Presage ST2 76 ng/mL BNP,
NT pro-BNP
2+
8 Bayes-Genis (2012)17) Multiple HF (891) Presage ST2 38.2 ng/mL NT pro-BNP 2+
9 Broch (2012)18) Chronic HF (1149) Presage ST2 17.5 ng/mL - 2+
10 Henry-Okafor (2012)19) Acute HF (375) Medical & biological 0.20 ng/mL - 2-
11 Manzano-Fernández (2012)20) ADHF (87) Presage ST2 44 ng/mL NT pro-BNP 2+
12 Ky (2011)21) Chronic HF (1141) Presage ST2 36.3 ng/mL NT pro-BNP 2+
13 Pascual-Figal (2011)22) ADHF (107) Presage ST2 65 ng/mL NT pro-BNP 2+
14 Bayes-Genis (2010)23) ADHF (48) Medical & biological 0.27 ng/mL NT pro-BNP 2+
15 Pascual-Figal (2009)24) ADHF (100) Medical & biological 0.15 ng/mL NT pro-BNP 2+
16 Boisot (2008)25) ADHF (150) Medical & biological 15.5% reduction BNP, NT pro-BNP
2+
17 Rehman (2008)4) Acute HF (346) Presage ST2 0.49 ng/mL BNP,
NT pro-BNP
2+
18 Weinberg (2003)26) HF (139) Medical & biological 0.24 ng/mL BNP 2+
19 Wojtczak-Soska (2013)27) Chronic HF (66) Medical & biological 0.28 ng/mL NT pro-BNP 3 ST2: suppression of tumorigenicity 2, HF: heart failure, BNP: B-type natriuretic peptide, NT pro-BNP: N-terminal pro-BNP, ADHF:
acute decompensated heart failure
Table 1. Ovid-MEDLINE and EMBASE search strategy
PICO No. Search terms MEDLINE EMBASE
Patient 1 Exp heart failure/ 88330 297397 2 Heart failure*.mp. 140909 238130
3 HF.mp. 25025 37470
4 OR 1–3 140415 343797
Index test 5 ST2.mp. 1207 1740
6 Suppression of Tumorigenicity 2.mp.
18 17
7 5 OR 6 1205 1764
8 4 AND 7 101 264
PICO: patient-index test-comparators-outcomes, HF: heart fail- ure, OR: odds ratio, ST2: suppression of tumorigenicity 2
are not written in English or Korean; 3) studies that are not original articles, gray literature, case reports; 4) studies not performed ST2 test in HF; 5) studies not reported appropriate outcomes. In cases in which it was unclear, we contacted the study authors for clarification. We resolved disagreements about whether a study should be included by consensus.
Risk of bias
The risk of bias in each study was evaluated by two indepen- dent researchers using Scottish Intercollegiate Guidelines Net- works checklist. Two investigators decided the Level of Evi- dence (1++ to 1-, 2++ to 2-, 3, 4) that led to the pragmatic Grading of Recommendations Assessment, Development, and Evaluation Recommendation (A-D).
Data extraction
A standardized data extraction from was used to extract outcomes of interest and two investigators independently ex- tracted data from selected full test articles using this form
(which reinforced the inclusion and exclusion criteria). Out- comes variables included association with prognosis [risk ratio (RR) or odds ratio (OR), accuracy of forecasting of the prog- nosis, stratification of risk], correlation with the comparators and relevance with clinical symptoms. If the two researchers disagreed on any topic, the disagreement was resolved by con- sultation. Two researchers abstracted the data from the select- ed studies in a blinded manner and all extracted data was checked with 5 experts.
Results
Study selection and characteristics
Searching the databases has retrieved a total of 365 studies, of these, 102 studies were excluded as duplicates. Total of 19 studies were included in the final assessment according to the inclusion and exclusion criteria (Table 2). The majority of the studies (n=108) were excluded as they were gray literature, other reasons for exclusion included studies not reported ap-
Fig. 1. Literature search algorithm (PRISMA 2009 flow diagram).
Records identified through databases searching
(n=365)
Record screened (n=263)
Full-text articles assessed for eligibility
(n=97)
Studies included in qualitative synthesis
(n =19)
Studies included in quantitative synthesis
(n=19)
Records after duplicates removed (n=102)
Records excluded Studies as follows:
- Studies that are not original articles (n=55) - Non-human, pre-clinical studies (n=2) - Not written in English, Korean (n=1) - Gray literature (n=108)
Full-text articles excluded, with reasons - Patients are not heart failure (n=6) - Not use ST2 test (n=10)
- Improper outcomes (n=62)
IdentificationScreeningEligibilityIncluded
propriate outcomes (n=62); studies that are not original arti- cles (n=55); studies not performed ST2 test (n=10); studies not performed in HF (n=6); the non-human, pre-clinical studies (n=2) or studies that are not written in English or Korean (n=1). A study flowchart details these exclusions (Fig. 1). We obtained and reviewed the full-text versions of the final 19 studies. Data extraction for all included studies and assessment of quality were independently performed by two researchers from August until October 2014.
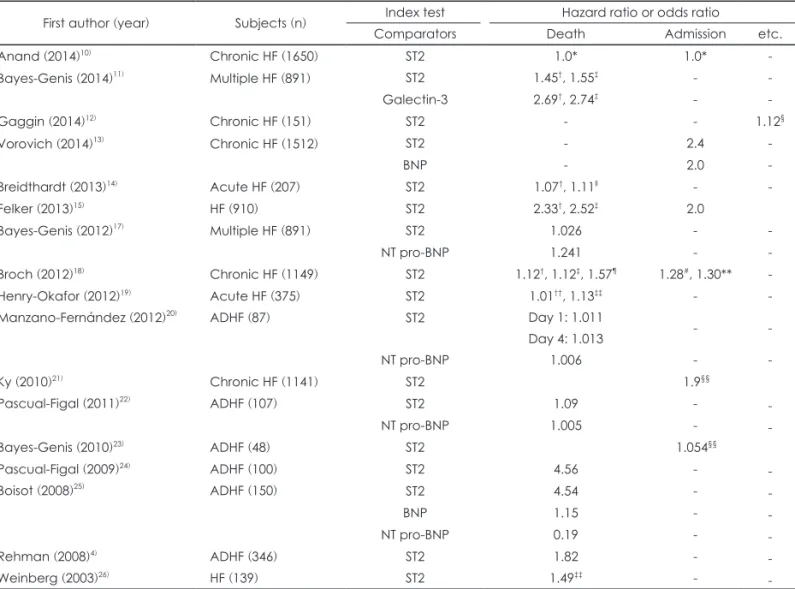
Synthesis of results Association with prognosis
Association with prognosis data were available for 17 peer- reviewed studies. ST2 displayed a RR or OR of 1.01−4.56 for mortality (all-cause mortality, cardiovascular mortality, in- hospital mortality, death due to worsening of HF, etc.). ST2 level was associated with increased risk of hospitalization (RR
1.054−2.4) and risk of cardiovascular event (RR 1.12). BNP, comparative test, displayed the RR of 1.15−2.0 for hospitaliza- tion, the RR or OR of NT pro-BNP and Galectin-3 for mortal- ity was respectively 0.19−1.241, 2.69−2.74 (Table 3).
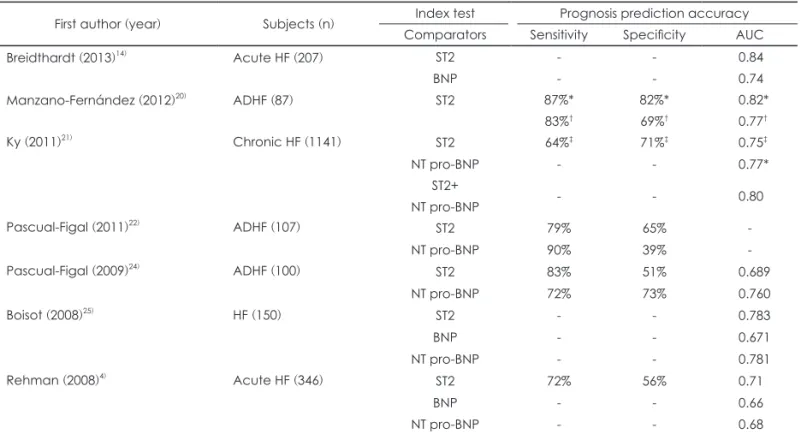
Prognosis prediction accuracy
Prognosis prediction accuracy data were available for 7 studies comparing BNP and NT pro-BNP. When these values were used to predict outcomes, ST2 had 64−87% sensitivity, 51−82% specificity. The area under the ROC curve (AUC) for ST2 mortality measurements was 0.689−0.84. 2 studies report- ed that sensitivity/specificity of NT pro-BNP was respectively 72/73%, 90/39% and AUC is 0.68−0.781. 3 studies reported AUC for BNP was 0.66−0.74 (Table 4).
Risk stratification
Risk stratification data were available for 4 studies. The net reclassification improvement (NRI) indicates the proportion
Table 3. Association with prognosis
First author (year) Subjects (n) Index test Hazard ratio or odds ratio
Comparators Death Admission etc.
Anand (2014)10) Chronic HF (1650) ST2 1.0* 1.0* -
Bayes-Genis (2014)11) Multiple HF (891) ST2 1.45†, 1.55‡ - -
Galectin-3 2.69†, 2.74‡ - -
Gaggin (2014)12) Chronic HF (151) ST2 - - 1.12§
Vorovich (2014)13) Chronic HF (1512) ST2 - 2.4 -
BNP - 2.0 -
Breidthardt (2013)14) Acute HF (207) ST2 1.07†, 1.11ll - -
Felker (2013)15) HF (910) ST2 2.33†, 2.52‡ 2.0
Bayes-Genis (2012)17) Multiple HF (891) ST2 1.026 - -
NT pro-BNP 1.241 - -
Broch (2012)18) Chronic HF (1149) ST2 1.12†, 1.12‡, 1.57¶ 1.28#, 1.30** -
Henry-Okafor (2012)19) Acute HF (375) ST2 1.01††, 1.13‡‡ - -
Manzano-Fernández (2012)20) ADHF (87) ST2 Day 1: 1.011
Day 4: 1.013 - -
NT pro-BNP 1.006 - -
Ky (2010)21) Chronic HF (1141) ST2 1.9§§
Pascual-Figal (2011)22) ADHF (107) ST2 1.09 - -
NT pro-BNP 1.005 - -
Bayes-Genis (2010)23) ADHF (48) ST2 1.054§§
Pascual-Figal (2009)24) ADHF (100) ST2 4.56 - -
Boisot (2008)25) ADHF (150) ST2 4.54 - -
BNP 1.15 - -
NT pro-BNP 0.19 - -
Rehman (2008)4) ADHF (346) ST2 1.82 - -
Weinberg (2003)26) HF (139) ST2 1.49‡‡ - -
*Addition of ST2 to clinical prediction model, †All-cause death, ‡Cardiovascular disease death, §Cardiovascular disease inci- dence, llIn-hospital death, ¶Death due to worsening of HF, #Cardiovascular disease hospitalization, **Hospitalization due to wors- ening of HF, ††Total recidivism, ‡‡ Recidivism due to HF, §§Death or hospitalization or cardiac transplantation. ADHF: acute decom- pensated heart failure, HF: heart failure, ST2: suppression of tumorigenicity 2, BNP: B-type natriuretic peptide, NT pro-BNP: N- terminal pro-BNP
of patients correctly classified when adding a marker to the clinical model.10) Of these, 2 studies reported that NRI for death improved after inclusion of ST2 into the clinical risk fac- tor and NT pro-BNP models (ST2 NRI 9.4, 9.9).11,16) But 1 study reported adding ST2 to models containing the clinical risk factor and NT pro-BNP doesn’t incrementally improve risk prediction for death (ST2 NRI 0.049) (Table 5).15)
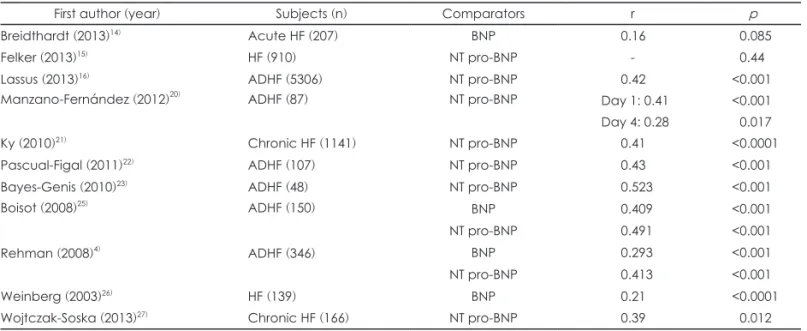
Correlation with comparative test
The correlation with comparative test was assessed on the basis of a total of 11 studies. The correlation coefficients with BNP was 0.16−0.409 and with NT pro-BNP was 0.28−0.523.
But 1 study reported that there was no statistical interaction between ST2 and NT pro-BNP (p=0.44) (Table 6).15)
Relevance with clinical symptoms
The relevance with clinical symptoms of ST2 was assessed on the basis of a total of 1 study. Maximum oxygen intake (peak VO2), an index of improvement in respiration function, was reported at 0.30 while the correlation coefficient with 6-minute walk distance, an index of improvement of motor function, was reported at 0.22, both of which were significant.
Discussion
HF is one of the diseases of cardiovascular system with con- tinually increasing prevalence rate and mortality rate. While BNP and NT pro-BNP, which are currently used as indices in predicting the prognosis of the HF patients, reacts to the he-
Table 5. Risk stratification
First author (year) Subjects (n) Criteria model Index test/
comparators
Risk stratification (NRI) Death Admission Bayes-Genis (2014)11) ADHF (891) Clinical risk factor+NT pro-BNP ST2 9.4* -
Galectin-3 0.7* -
Felker (2013)15) HF (910) Clinical risk factor+NT pro-BNP ST2 0.049 * 0.0638
Lassus (2013)16) ADHF (5306) Clinical risk factor ST2 25.5†, 10.3‡ -
BNP 4.4†, 5.5‡ -
NT Pro-BNP 8.8†, 9.1‡ - Bayes-Genis (2012)17) Multiple HF (891) Clinical risk factor+NT pro-BNP ST2 9.9* -
*All-cause death, †30 days death, ‡1 year death. ADHF: acute decompensated heart failure, HF: heart failure, NRI: net reclassifi- cation improvement, ST2: suppression of tumorigenicity 2, BNP: B-type natriuretic peptide, NT pro-BNP: N-terminal pro-BNP Table 4. Prognosis prediction accuracy (mortality)
First author (year) Subjects (n) Index test Prognosis prediction accuracy Comparators Sensitivity Specificity AUC
Breidthardt (2013)14) Acute HF (207) ST2 - - 0.84
BNP - - 0.74
Manzano-Fernández (2012)20) ADHF (87) ST2 87%*
83%†
82%*
69%†
0.82*
0.77†
Ky (2011)21) Chronic HF (1141) ST2 64%‡ 71%‡ 0.75‡
NT pro-BNP - - 0.77*
ST2+
NT pro-BNP - - 0.80
Pascual-Figal (2011)22) ADHF (107) ST2 79% 65% -
NT pro-BNP 90% 39% -
Pascual-Figal (2009)24) ADHF (100) ST2 83% 51% 0.689
NT pro-BNP 72% 73% 0.760
Boisot (2008)25) HF (150) ST2 - - 0.783
BNP - - 0.671
NT pro-BNP - - 0.781
Rehman (2008)4) Acute HF (346) ST2 72% 56% 0.71
BNP - - 0.66
NT pro-BNP - - 0.68
*Day 1 of hospitalization, †Day 4 of hospitalization, ‡Death or cardiac transplantation. AUC: area under the ROC curve, ADHF:
acute decompensated heart failure, HF: heart failure, ST2: suppression of tumorigenicity 2, BNP: B-type natriuretic peptide, NT pro- BNP: N-terminal pro-BNP
modynamic stimulations such as the increase in ventricular volume and pressure overload, etc., ST2 is a biomarker that re- flects the extent of remodeling of ventricles of the heart and myocardial fibrosis.
Nemerous studies of biomarker testing for prognosis have suggested potential utility of a wide array of assays when mea- sured in patients with HF. Recent statements call for, a more standardized, through, and rigorous approach to evaluating HF biomarkers, including assessing them in a wide range of patients, and using contemporary, comprehensive, standard- ized when comparing biomarkers to each other and to clinical variables.
This study provides an effectiveness of the clinical studies that have led to the establishment of ST2 as a guideline-en- dorsed biomarker of cardiovascular risk. The guidelines note that not only is ST2 predictive of hospitalization and death in patients with HF, but information gleaned from ST2 measures provides additive prognostic value to that from natriuretic peptides.9)
Felker et al.15) evaluated the association of ST2 levels with functional capacity and long-term clinical outcomes in a co- hort of HF enrolled in the HF: A Controlled Trial Investigating Outcomes of Exercise Training (HF-ACTION) study, which was a multicenter randomized study of exercise training in HF.
HF-ACTION randomized 2331 patients with left ventricular ejection fractions <35% and New York Heart Association class II to IV HF to either an exercise program or usual care. ST2 was analyzed in a subset of 910 patients with evaluable plasma samples. In this analysis of a large clinical study cohort, ST2 el- evation was significantly associated with long-term outcomes, especially disease-specific outcomes. These associations were relatively robust for disease-specific end points such as cardio-
vascular death and HF hospitalization in traditional multivari- ate adjustment, including adjustment for demographics, clini- cal variables, and NT pro-BNP levels.
Accordingly, our study assessed the prediction of prognosis (association with prognosis, accuracy of prognosis and stratifi- cation of risks), correlation with comparators and the rele- vance with the clinical symptoms in order to evaluate the ef- fectiveness of ST2 in heart failure.
As the result of assessment, ST2 is an independent factor for predicting the prognosis of the HF patients including mortali- ty rate and hospitalization rate. It was of the opinion that the accuracy of ST2 in predicting the prognosis is at a level similar to those of the existing comparators, and it would be clinically helpful in predicting and treating the conditions of the patient with ST2 test. In addition, although the correlation coefficient with the comparators was reported to be somewhat low, it was statistically significant. Moreover, BNP, NT pro-BNP and ST2 reflect mutually different pathological physiology mechanisms, thereby demonstrating that ST2 has mutually supplementary relationship with the comparators. Therefore, it is significant in itself even though the correlation coefficients with the com- parators are found to be somewhat low.
However, the limitations of this study include, first, the fact that clinical study on the long-term prognosis on a large num- ber of patients as the subjects was not executed. Nonetheless, statistical analysis that enabled comparison with the existing researches was possible, and it was appropriate to reach con- clusion by using the pooled data since extensive researches had already been executed. Second, unified single test kit was not used as the method of test. However, there was no problem in statistical analysis since the same test kits were used on all the patients in the same research. Third, there was no research that
Table 6. Correlation with comparators
First author (year) Subjects (n) Comparators r p
Breidthardt (2013)14) Acute HF (207) BNP 0.16 0.085
Felker (2013)15) HF (910) NT pro-BNP - 0.44
Lassus (2013)16) ADHF (5306) NT pro-BNP 0.42 <0.001
Manzano-Fernández (2012)20) ADHF (87) NT pro-BNP Day 1: 0.41
Day 4: 0.28
<0.001 0.017
Ky (2010)21) Chronic HF (1141) NT pro-BNP 0.41 <0.0001
Pascual-Figal (2011)22) ADHF (107) NT pro-BNP 0.43 <0.001
Bayes-Genis (2010)23) ADHF (48) NT pro-BNP 0.523 <0.001
Boisot (2008)25) ADHF (150) BNP 0.409 <0.001
NT pro-BNP 0.491 <0.001
Rehman (2008)4) ADHF (346) BNP 0.293 <0.001
NT pro-BNP 0.413 <0.001
Weinberg (2003)26) HF (139) BNP 0.21 <0.0001
Wojtczak-Soska (2013)27) Chronic HF (166) NT pro-BNP 0.39 0.012
ADHF: acute decompensated heart failure, HF: heart failure, BNP: B-type natriuretic peptide, NT pro-BNP: N-terminal pro-BNP
made report on the treatment reaction to this test. This is a task that should be implemented by applying ST2 in clinical settings in the future.
In spite of the limitations of this study, ST2 has the level of diagnostic accuracy that is similar to BNP and NT pro-BNP on the basis of literary evidences. Moreover, it is significant that ST2 has mutually supplementary relationship with the comparators. Therefore, it is determined that ST2 is effective in determining the prognosis of the HF patients. In addition, it is determined that researches on its influence on the results of treatment of patients after having used in the actual clinical settings in the future are necessary.
Conclusions
In conclusion, ST2 is a cardiac biomarker that adds inde- pendent prognostic information, and provides incremental val- ue to natriuretic peptides for risk stratification in HF patients.
The ST2 appears promising in determining the prognosis in HF, and may assist in clinical decision making.
REFERENCES
1) McKee PA, Castelli WP, McNamara PM, Kannel WB. The natural history of congestive heart failure: the Framingham study. N Engl J Med 1971;285:1441-1446.
2) Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cush- man M, et al. Heart disease and stroke statistics--2015 update: a re- port from the American Heart Association. Circulation 2015;131:e29- e322.
3) CDC. Heart failure fact sheet. Available from: http://www.cdc.gov/
DHDSP/data_statistics/fact_sheets/fs_heart_failure.htm. Accessed September 2, 2014.
4) Rehman SU, Mueller T, Januzzi JL Jr. Characteristics of the novel interleukin family biomarker ST2 in patients with acute heart fail- ure. J Am Coll Cardiol 2008;52:1458-1465.
5) Melander O, Newton-Cheh C, Almgren P, Hedblad B, Berglund G, Engström G, et al. Novel and conventional biomarkers for predic- tion of incident cardiovascular events in the community. JAMA 2009;
302:49-57.
6) Manabe I, Shindo T, Nagai R. Gene expression in fibroblasts and fi- brosis: involvement in cardiac hypertrophy. Circ Res 2002;91:1103- 1113.
7) Bartunek J, Delrue L, Van Durme F, Muller O, Casselman F, De Wi- est B, et al. Nonmyocardial production of ST2 protein in human hy- pertrophy and failure is related to diastolic load. J Am Coll Cardiol 2008;52:2166-2174.
8) Schmitz J, Owyang A, Oldham E, Song Y, Murphy E, McClanahan TK, et al. IL-33, an interleukin-1-like cytokine that signals via the IL-1 receptor-related protein ST2 and induces T helper type 2-asso- ciated cytokines. Immunity 2005;23:479-490.
9) Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/
American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2013;62:e147-e239.
10) Anand IS, Rector TS, Kuskowski M, Snider J, Cohn JN. Prognostic value of soluble ST2 in the Valsartan Heart Failure Trial. Circ Heart Fail 2014;7:418-426.
11) Bayes-Genis A, de Antonio M, Vila J, Peñafiel J, Galán A, Barallat J, et al. Head-to-head comparison of 2 myocardial fibrosis biomarkers for long-term heart failure risk stratification: ST2 versus galectin-3.
J Am Coll Cardiol 2014;63:158-166.
12) Gaggin HK, Szymonifka J, Bhardwaj A, Belcher A, De Berardinis B, Motiwala S, et al. Head-to-head comparison of serial soluble ST2, growth differentiation factor-15, and highly-sensitive troponin T measurements in patients with chronic heart failure. JACC Heart Fail 2014;2:65-72.
13) Vorovich E, French B, Ky B, Goldberg L, Fang JC, Sweitzer NK, et al. Biomarker predictors of cardiac hospitalization in chronic heart failure: a recurrent event analysis. J Card Fail 2014;20:569-576.
14) Breidthardt T, Balmelli C, Twerenbold R, Mosimann T, Espinola J, Haaf P, et al. Heart failure therapy-induced early ST2 changes may offer long-term therapy guidance. J Card Fail 2013;19:821-828.
15) Felker GM, Fiuzat M, Thompson V, Shaw LK, Neely ML, Adams KF, et al. Soluble ST2 in ambulatory patients with heart failure: as- sociation with functional capacity and long-term outcomes. Circ Heart Fail 2013;6:1172-1179.
16) Lassus J, Gayat E, Mueller C, Peacock WF, Spinar J, Harjola VP, et al. Incremental value of biomarkers to clinical variables for mortali- ty prediction in acutely decompensated heart failure: the Multina- tional Observational Cohort on Acute Heart Failure (MOCA) study.
Int J Cardiol 2013;168:2186-2194.
17) Bayes-Genis A, de Antonio M, Galán A, Sanz H, Urrutia A, Ca- banes R, et al. Combined use of high-sensitivity ST2 and NTproB- NP to improve the prediction of death in heart failure. Eur J Heart Fail 2012;14:32-38.
18) Broch K, Ueland T, Nymo SH, Kjekshus J, Hulthe J, Muntendam P, et al. Soluble ST2 is associated with adverse outcome in patients with heart failure of ischaemic aetiology. Eur J Heart Fail 2012;14:268- 19) Henry-Okafor Q, Collins SP, Jenkins CA, Miller KF, Maron DJ, 277.
Naftilan AJ, et al. Soluble ST2 as a diagnostic and prognostic marker for acute heart failure syndromes. Open Biomark J 2012;2012:1-8.
20) Manzano-Fernández S, Januzzi JL, Pastor-Pérez FJ, Bonaque- González JC, Boronat-Garcia M, Pascual-Figal DA, et al. Serial mon- itoring of soluble interleukin family member ST2 in patients with acutely decompensated heart failure. Cardiology 2012;122:158-166.
21) Ky B, French B, McCloskey K, Rame JE, McIntosh E, Shahi P, et al.
High-sensitivity ST2 for prediction of adverse outcomes in chronic heart failure. Circ Heart Fail 2011;4:180-187.
22) Pascual-Figal DA, Manzano-Fernández S, Boronat M, Casas T, Garrido IP, Bonaque JC, et al. Soluble ST2, high-sensitivity troponin T- and N-terminal pro-B-type natriuretic peptide: complementary role for risk stratification in acutely decompensated heart failure.
Eur J Heart Fail 2011;13:718-725.
23) Bayes-Genis A, Pascual-Figal D, Januzzi JL, Maisel A, Casas T, Val- dés Chávarri M, et al. Soluble ST2 monitoring provides additional risk stratification for outpatients with decompensated heart failure.
Rev Esp Cardiol 2010;63:1171-1178.
24) Pascual-Figal DA, Ordoñez-Llanos J, Tornel PL, Vázquez R, Puig T, Valdés M, et al. Soluble ST2 for predicting sudden cardiac death in patients with chronic heart failure and left ventricular systolic dys- function. J Am Coll Cardiol 2009;54:2174-2179.
25) Boisot S, Beede J, Isakson S, Chiu A, Clopton P, Januzzi J, et al. Se- rial sampling of ST2 predicts 90-day mortality following destabi- lized heart failure. J Card Fail 2008;14:732-738.
26) Weinberg EO, Shimpo M, Hurwitz S, Tominaga S, Rouleau JL, Lee RT. Identification of serum soluble ST2 receptor as a novel heart failure biomarker. Circulation 2003;107:721-726.
27) Wojtczak-Soska K, Pietrucha T, Sakowicz A, Lelonek M. Soluble ST2 protein in chronic heart failure is independent of traditional fac- tors. Arch Med Sci 2013;9:21-26.