ORIGINAL ARTICLE
한국에서 헬리코박터 파일로리 감염에 대한 동시 치료와 순차 치료의 비교: 체계적 문헌고찰과 메타분석
배현진, 김준성, 김병욱, 남윤정
가톨릭대학교 의과대학 인천성모병원 소화기내과
Concomitant or Sequential Therapy as the First-line Therapy for Eradication of Helicobacter pylori Infection in Korea: A Systematic Review and Meta-analysis
Hyun Jin Bae, Joon Sung Kim, Byung-Wook Kim and Yun Jung Nam
Division of Gastroenterology, Department of Internal Medicine, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Incheon, Korea
Background/Aims: In Korea, increasing clarithromycin resistance has led to the need for an alternative first-line therapy for the erad- ication of Helicobacter pylori (H. pylori) infection. Concomitant therapy (CT) and sequential therapy (ST) have been proposed as alter- native regimens. The aim of this study was to compare the eradication rate from using CT and ST in Korea.
Methods: A literature review was performed on studies comparing the efficacy of CT and ST in Korea. Data were pooled to obtain the odds ratio (OR) of the eradication rate with 95% confidence intervals (CIs). The eradication rates were considered both on an intention-to-treat (ITT) and a per-protocol (PP) bases.
Results: Six studies provided data on 1,897 Korean adult patients. The pooled OR was 1.382 (95% CI: 1.031-1.853, p=0.031) for ITT analysis and 2.114 (95% CI: 1.502-2.974, p<0.001) for PP analysis. There was no difference in the rate of adverse events and compliances between the two regimens.
Conclusions: The efficacy of CT was superior to ST in both ITT and PP analyses. Therefore, CT could be an excellent alternative regimen for the eradication of H. pylori as a first-line therapy in Korea. (Korean J Gastroenterol 2018;71:31-37)
Key Words: Helicobacter pylori; Concomitant therapy; Sequential therapy; Meta-analysis
Received October 11, 2017. Revised November 16, 2017. Accepted December 9, 2017.
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2018. Korean Society of Gastroenterology.
교신저자: 김병욱, 21431, 인천시 부평구 동수로 56, 가톨릭대학교 의과대학 인천성모병원 소화기내과
Correspondence to: Byung-Wook Kim, Division of Gastroenterology, Department of Internal Medicine, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 56 Dongsu-ro, Bupyeong-gu, Incheon 21431, Korea. Tel: +82-32-280-5052, Fax: +82-32-280-5987, E-mail: [email protected]
Financial support: None. Conflict of interest: None.
INTRODUCTION
Guidelines for the diagnosis and treatment of Helicoba- cter pylori (H. pylori) infection were first developed in 1998 by the Korean H. pylori study group, and updated in 2009 and 2013.1,2 Most international guidelines have recommended a regimen of triple therapy (TT) consisting of proton pump in- hibitor (PPI), amoxicillin or metronidazole, and clarithromycin
as the first line therapy to eradicate H. pylori. However, the eradication rate from using TT has been declining in the past decades worldwide, and is now considered to be below 80%
in Korea.3,4 Nevertheless, according to the 2013 revised Korean guideline, TT is still recommended as the first line therapy since there is no better option to date. Thus, it is ur- gent to develop a more effective strategy. Concomitant ther- apy (CT) and sequential therapy (ST) have been proposed as
alternatives to TT. They have been studied vigorously in vari- ous countries including Korea. Most of these studies con- cluded that CT showed better outcome compared with ST.
However, previous meta-analyses failed to show the superi- ority of CT compared with ST.5
We assumed that there might be a regional difference in the eradication rate of each regimen and performed a systematic review and meta-analysis of the studies comparing CT and ST in Korea.
SUBJECTS AND METHODS
1. Literature search and selection
According to the preferred reporting items for Systemic Reviews and Meta-Analyses (PRISMA) protocols, we searched PubMed, EMBASE, KoreaMed, and Cochrane Library for studies comparing CT with ST for H. pylori infection.6 Combinations of the following key words were used in the search: “Helicobacter pylori”, “concomitant therapy”, “sequential therapy”, “disease eradication”,
“therapeutics”, and “drug therapy”. The results of the search were reviewed by two authors (HJ Bae and JS Kim).
Studies were eligible if they included both CT and ST as the first-line therapy, and met the following criteria:
(1) diagnosis of H. pylori infection by at least one of the following methods: rapid urease test, urea breath test, histology, or culture; (2) confirmation of eradication of in- fection by an appropriate follow-up test; (3) CT consisting of a PPI, amoxicillin, clarithromycin, and metronidazole given concomitantly for 7-14 days; and (4) ST consisting of PPI and amoxicillin for the first 5-7 days, followed by triple therapy, including PPI, clarithromycin, and metroni- dazole for the remaining 5-7 days. Case reports, letters, editorials, commentaries, reviews, and abstracts were excluded.
2. Data extraction
A manual for data extraction was made ahead of time, and two authors (HJ Bae and JS Kim) collected the data independently. The following items were extracted from the selected articles: study design; number of patients enrolled each study in total and in respective treatment groups; diag- nostic methods of testing H. pylori infection before enroll- ment and after the end of treatment; drug regimens; num-
ber of patients who were successfully eradicated for corre- sponding regimens; and the incidence of adverse events.
The extracted data were sorted out independently by the two authors, and disagreements were resolved by consensus. We tried to contact the original authors if we need additional information.
3. Risk of bias in individual studies
We used two different risk assessment tools according to the study designs. The risk of bias for randomized controlled trials (RCTs) was assessed using the tool developed by Cochrane collaboration.7 The criteria were randomization (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), in- complete outcome data (attrition bias), selective reporting (reporting bias), and other biases. Each part was recorded as yes (Y), no (N), or unclear (U), and any disagreements were resolved by consensus. The risk of bias for non- randomized studies was assessed by Newcastle-Ottawa scale.8 It was categorized to three parts: selection (com- posed of four individual questions), comparability of study groups (of two questions), and ascertainment of exposure or outcome (of three questions). Each question was scored for one point, and the studies receiving more than six points were considered as high quality.
4. Statistical analysis
The pooled odds ratio (OR) with 95% confidence intervals (CIs) were calculated. The eradication rates were analyzed on both intention-to-treat (ITT) population and per-protocol (PP) population. Full application of ITT analysis can only be performed for RCTs; thus, we excluded retrospective studies for ITT analysis. We evaluated the heterogeneity between the pooled estimates using Cochran’s Q test and I2 statis- tics. When there was high heterogeneity (p<0.1 or I2>50), the random-effect model should be used to combine the ef- fect sizes of the included studies. However, a nonsignificant test only represents a scarcity of evidence for heterogeneity, as there may have been insufficient power to detect any heterogeneity. Therefore, we decided to take the pooled OR on a conservative approach and used a random-effects model. Subgroup analysis and meta-regression were also performed when needed. To evaluate the discrepancies of
Table 1. Main Characteristics of Included Studies
Study Centers Year of publication Type of patients No. of patients Study duration
Park et al.9 Single 2017 PUD+NUD 341 February 2014 to December 2015
Chung et al.10 Multi 2016 PUD+NUD 346 May 2013 to March 2015
Lee et al.11 Multi 2015 PUD+NUD 340 July 2013 to March 2014
Lim et al.12 Single 2013 PUD+NUD 164 May 2011 to April 2012
Jung et al.13 Single 2016 PUD+NUD 390 September 2012 to March 2015
Kim et al.14 Single 2014 PUD+NUD 316 November 2010 to January 2013
PUD, peptic ulcer disease; NUD, nonulcer dyspepsia.
Fig. 1. Flow diagram of studies included in this meta-analysis. RCT, randomized controlled trial.
small scale studies and publication bias, we also conducted Egger’s test and formed a funnel plot when necessary.
Statistical analyses were executed by the aid of Compre- hensive meta-analysis software version 2 (Biostat Inc., Englewood, NJ, USA).
RESULTS
1. Study identification and selection
Literature review was initially conducted on 218 studies.
After excluding 193 studies after reviewing the summaries, 25 studies were close examined. Thereafter, 6 studies, in- cluding 4 RCTs 9-12 and 2 observational studies,13,14 met our inclusion criteria for meta-analysis (Fig. 1).
2. Study characteristics
The main characteristics of the studies are presented in Tables 1 and 2. Four studies were single-centered, whereas the remaining two studies were multi-centered design. The enrollment period ranged between 2010 and 2015. Two
studies used pantoprazole, three studies used rabeprazole, and the remaining one study used lansoprazole for CT and ST regimens. Two studies used metronidazole 500 mg three times a day, while the rest used metronidazole two times a day. Treatment durations were 7, 10, and 14 days for CT, and 10 and 14 days for ST.
3. Risk of bias in individual studies
Tables 3 and 4 show summaries of the quality assess- ment of the included studies . Among the four prospective studies, allocation concealment was adequate in only one study. The two authors both assessed the literature de- termined that the two observational studies were relatively well-designed.
4. Eradication rates of ST and CT
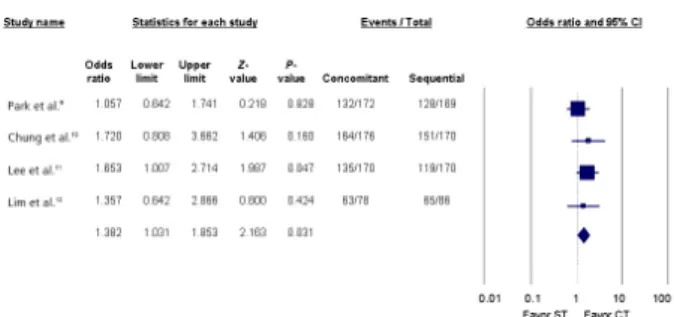
A total of 1897 Korean patients were included; of whom 917 were treated with CT and 980 were treated with ST. The pooled ITT eradication rates were 82.53% (95% CI:
71.0-94.1) for CT and 77.54% (95% CI: 64.8-90.2) for ST.
The pooled PP eradication rates were 85.50% (95% CI:
78.6-92.4) for ST and 91.50% (95% CI: 83.8-99.2) for CT.
The pooled OR of ITT eradication rates was 1.382 (95% CI:
1.031-1.853, p=0.031) (Fig. 2). The pooled OR of PP erad- ication rates was 2.114 (95% CI: 1.502-2.974, p<0.001) (Fig. 3). The pooled OR of PP eradication rates for RCTs was 2.102 (95% CI: 1.346-3.282, p=0.001).
There was some funnel plot asymmetry (Fig. 4), which was compatible with publication bias; however, statistical analysis using Egger’s test showed no significance (p=0.426). These results should be interpreted with caution because the asymmetry test is probably underpowered as there were only six studies included in this meta-analysis.
Table 2. Data Extracted from Included Studies
Studies
Tests for confirming
infection
Tests for confirming eradication
Duration
of CT CT regimen Duration
of ST
ST regimen (first 5 or 7 days)
ST regimen (second 5 or 7 days) Park et al.9 RUT or histology UBT or RUT or
histology
10, 14 Pantoprazole 40 mg bid Amoxicillin 1 g bid Clarithromycin 500 mg bid Metronidazole 500 mg bid
10, 14 Pantoprazole 40 mg bid Amoxicillin 1 g bid
Pantoprazole 40 mg bid Clarithromycin 500 mg bid Metronidazole 500 mg bid
Chung et al.10 Histology UBT 10 Pantoprazole 40 mg bid Amoxicillin 1 g bid Clarithromycin 500 mg bid Metronidazole 500 mg bid
10 Pantoprazole 40 mg bid Amoxicillin 1 g bid
Pantoprazole 40 mg bid Clarithromycin 500 mg bid Metronidazole 500 mg bid
Lee et al.11 Histology UBT 7 Rabeprazole 20 mg bid Amoxicillin 1 g bid Clarithromycin 500 mg bid Metronidazole 500 mg tid
10 Rabeprazole 20 mg bid Amoxicillin 1 g bid
Rabeprazole 20 mg bid Clarithromycin 500 mg bid Metronidazole 500 mg tid
Lim et al.12 RUT or histology UBT 14 Rabeprazole 20 mg bid Amoxicillin 1 g bid Clarithromycin 500 mg bid Metronidazole 500 mg bid
14 Rabeprazole 20 mg bid Amoxicillin 1 g bid
Rabeprazole 20 mg bid Clarithromycin 500 mg bid Metronidazole 500 mg bid
Jung et al.13 Histology UBT 7 Rabeprazole 20 mg bid Amoxicillin 1 g bid Clarithromycin 500 mg bid Metronidazole 500 mg tid
10 Rabeprazole 20 mg bid Amoxicillin 1 g bid
Rabeprazole 20 mg bid Clarithromycin 500 mg bid Metronidazole 500 mg tid
Kim et al.14 UBT or RUT or histology
UBT 10 Lansoprazole 30 mg bid Amoxicillin 1g bid Clarithromycin 500 mg bid Metronidazole 500 mg bid
10 Lansoprazole 30 mg bid Amoxicillin 1 g bid
Lansoprazole 30 mg bid Clarithromycin 500 mg bid Metronidazole 500 mg bid
CT, concomitant therapy; ST, sequential therapy; RUT, rapid urease test; UBT, urea breath test.
Table 4. Quality Assessment and Characteristics of Included Retrospective Studies
Study Selection Comparability Exposure Total
Jung et al.13 **** * ** 7 points
Kim et al.14 **** * ** 7 points
“*” indicates one point.
Table 3. Quality Assessment and Characteristics of Included Studies Study Randomization Allocation
concealment
Blinding of participants and personnel
Blinding of outcome assessment
Incomplete outcome data
Selective
reporting Other bias
Park et al.9 Yes Yes No No Yes Yes Yes
Chung et al.10 Yes Unclear No Unclear Yes Yes Yes
Lee et al.11 Yes Unclear No No Yes Yes Yes
Lim et al.12 Yes Unclear No No Yes Yes Yes
Jung et al.13 No No No No Unclear Yes Yes
Kim et al.14 No No No No Yes Yes Yes
"Yes" indicates a low risk of bias and "No" indicates high risk of bias. "Unclear" indicates insufficient or unknown details.
5. Adverse events and compliances
No significant heterogeneity was observed among the studies for adverse events (p=0.1401, I2=42.21%). The pooled OR for adverse events was 1.171 (95% CI:
0.883-1.554, p=0.274) and the corresponding rates were 39.50% (95% CI: 30.3-48.7) for CT and 37.79% (95% CI:
31.7-43.9) for ST (Fig. 5). Low heterogeneity was observed among the studies for compliance to the medications (p=0.7056, I2=0.0%). The pooled OR for compliance was 0.734 (95% CI: 0.407-1.322, p=0.303) and the corre- sponding rates were 96.78% (95% CI: 95.1-98.4) for CT and 96.95% (95% CI: 94.0-99.9) for ST.
Fig. 2. Forest plot of intention-to-treat analysis of CT compared with ST. CI, confidence interval; ST, sequential therapy; CT, concomitant therapy.
Fig. 3. Forest plot of per-protocol analysis of CT compared with ST.
CI, confidence interval; ST, sequential therapy; CT, concomitant therapy.
Fig. 4. Funnel plot asymmetry test for the detection of bias within the studies for the eradication rate of concomitant therapy com- pared with sequential therapy.
Fig. 5. Forest plot of adverse events of concomitant therapy CT com- pared with sequential therapy ST. CI, confidence interval; ST, se- quential therapy; CT, concomitant therapy.
6. Subgroup analysis according to the duration of CT Except for one study, all other studies included a sequen- tial therapy of 10 days. However, the duration of CT varied, from 7, to 14 days. Hence, we performed a subgroup analy- sis based on the duration of CT. Three studies compared 10 days of concomitant therapy with 10 days of sequential
therapy. The pooled OR of eradication rates were 2.617 (95% CI: 1.484-4.615, p=0.001) favoring CT. Two studies compared 7 days of concomitant therapy with 10 days of ST.
The pooled OR of eradication rates were 2.079 (95% CI:
1.073-4.029, p=0.030) favoring CT. We did not perform a subgroup analysis if the duration of CT was longer than the duration of ST. Moreover, because all but one study tested a sequential therapy lasting 10 days, a subgroup analysis ac- cording to the duration of ST was not performed.
DISCUSSION
The eradication rate of TT for H. pylori has been declining recently in Korea.4 The main cause of this tendency is likely due to increased antibiotic resistance of H. pylori.15 Many Korean gastroenterologists are struggling to find a regimen that can overcome this issue. CT and ST have been pro- posed as alternative regimens by various countries16-18 and studied vigorously for the past several years in Korea.16,17,19
Previous meta-analyses have compared the eradication rates of ST and CT. One meta-analysis reported that CT did not achieve a higher eradication rate compared with ST.5 However, a recent meta-analysis, including 20 randomized controlled trials, reported that 10 days of CT regimen ap- pears to be superior to a 10 days of ST regimen.18 Korea is a region with high antibiotic resistance to clarithromycin and metronidazole. Therefore, we decided to perform a meta-analysis regarding studies performed only in Korea.
This meta-analysis showed that CT was superior com- pared with ST with respect to the eradication of H. pylori in Korea. There was no difference in adverse events and com- pliance between the two regimens. To the best of our knowl- edge, this is the first meta-analysis comparing CT and ST as
first-line therapy based only on the Korean population.
Considering that the eradication rate of TT is rapidly declin- ing in Korea, CT might replace TT as the first line therapy.
However, we could not conclude the optimal duration of CT through our analysis. Subgroup analysis showed both 7-day and 10-day regimen of CT to be better than10-day of ST; however, direct comparison between 7 and 10 days of CT has not been performed due to limited data.
The results of our study correlates to previous studies and further shows that ST is inferior to CT. High metronida- zole resistance rates may be the reason for these results. It is known that metronidazole resistance can be partially overcome by increasing the dose, frequency, and duration of antibiotics.16 While a regimen of ST provides metronida- zole for 5-7 days, a regimen of CT provides metronidazole for 10-14 days. The longer duration of metronidazole use might overcome resistance, resulting in increased eradication rates for the CT regimen.
There are some limitations to consider when interpreting our findings. First, the studies included in this analysis were small, and there were two retrospective studies included.
Hence, we could not precisely measure the publications bias and examine correlation between the duration of CT and eradication rates. Second, there was no single study that reported antibiotics resistance and its association with the eradication rates. At first, CT and ST were developed due to increasing antibiotics resistance. However, since anti- biotic resistance was not available in any study, we were un- able to compare which regimen was more superior to anti- biotic-resistant strains.
In conclusion, for the Korean population, it seems, with statistical significance, that CT is more effective than ST as the first line therapy to eradicate H. pylori infection. There were no differences in adverse events and compliance be- tween the two regimens. Further prospective studies regard- ing the optimal duration of CT, with an investigation of its ef- fectiveness on antibiotic-resistant strains are necessary.
REFERENCES
1. Kim N, Kim JJ, Choe YH, et al. Diagnosis and treatment guidelines for Helicobacter pylori infection in Korea. Korean J Gastroenterol 2009;54:269-278.
2. Kim SG, Jung HK, Lee HL, et al. Guidelines for the diagnosis and treatment of Helicobacter pylori infection in Korea, 2013 revised edition. Korean J Gastroenterol 2013;62:3-26.
3. Papastergiou V, Georgopoulos SD, Karatapanis S. Current and future insights in H. pylori eradication regimens: the need of tai- loring therapy. Curr Pharm Des 2014;20:4521-4532.
4. Kim YK, Kim JS, Kim BW. Recent trends of Helicobacter pylori eradication therapy in Korea. Korean J Helicobacter Up Gastr- ointest Res 2012;12:219-223.
5. Kim JS, Park SM, Kim BW. Sequential or concomitant therapy for eradication of Helicobacter pylori infection: a systematic review and meta-analysis. J Gastroenterol Hepatol 2015;30:1338-1345.
6. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration.
J Clin Epidemiol 2009;62:e1-e34.
7. Higgins JPT, Altman DG, Sterne JAC. Cochrnae handbook for sys- tematic reviews of interventions, version 5.1.0. Chapter 8: as- sessing risk of bias in included studies. [Internet]. London:
Cochrane Training; 2006 Sep [updated Mar 2011; cited 2016 Jan 31]. Available from: http://handbook.cochrane.org/chap- ter_8/8_assessing_risk_of_bias_in_included_studies.htm 8. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the
assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 2010;25:603-605.
9. Park SM, Kim JS, Kim BW, Ji JS, Choi H. Randomized clinical trial comparing 10- or 14-day sequential therapy and 10- or 14-day concomitant therapy for the first line empirical treatment of Helicobacter pylori infection. J Gastroenterol Hepatol 2017;32:
589-594.
10. Chung JW, Han JP, Kim KO, et al. Ten-day empirical sequential or concomitant therapy is more effective than triple therapy for Helicobacter pylori eradication: a multicenter, prospective study.
Dig Liver Dis 2016;48:888-892.
11. Lee HJ, Kim JI, Lee JS, et al. Concomitant therapy achieved the best eradication rate for Helicobacter pylori among various treat- ment strategies. World J Gastroenterol 2015;21:351-359.
12. Lim JH, Lee DH, Choi C, et al. Clinical outcomes of two-week se- quential and concomitant therapies for Helicobacter pylori erad- ication: a randomized pilot study. Helicobacter 2013;18:180-186.
13. Jung SM, Cheung DY, Kim JI, Kim I, Seong H. Comparing the effi- cacy of concomitant therapy with sequential therapy as the first-line therapy of Helicobacter pylori eradication. Gastroenter- ol Res Pract 2016;2016:1293649.
14. Kim SY, Park DK, Kwon KA, Kim KO, Kim YJ, Chung JW. Ten day concomitant therapy is superior to ten day sequential therapy for Helicobacter pylori eradication. Korean J Gastroenterol 2014;
64:260-267.
15. Lee JW, Kim N, Kim JM, et al. Prevalence of primary and secon- dary antimicrobial resistance of Helicobacter pylori in Korea from 2003 through 2012. Helicobacter 2013;18:206-214.
16. Chey WD, Leontiadis GI, Howden CW, Moss SF. ACG clinical guide- line: treatment of Helicobacter pylori infection. Am J Gastroenter- ol 2017;112:212-239.
17. Fock KM, Katelaris P, Sugano K, et al. Second Asia-Pacific con- sensus guidelines for Helicobacter pylori infection. J Gastroen- terol Hepatol 2009;24:1587-1600.
18. Wang Y, Zhao R, Wang B, et al. Sequential versus concomitant therapy for treatment of Helicobacter pylori infection: an updated
systematic review and meta-analysis. Eur J Clin Pharmacol 2018;74:1-13.
19. Malfertheiner P, Megraud F, O'Morain CA, et al. Management of
Helicobacter pylori infection-the Maastricht V/Florence con- sensus report. Gut 2017;66:6-30.